
Abstract

Keywords
Introduction
Primary immunodeficiencies, also known as inborn errors of immunity (IEI), are a group of heterogeneous disorders, comprising of a plenitude of single gene defects, resulting in the impairment of the structure or function of the immune system. They account for a significant health burden in the community due to their increased susceptibility to infections, allergies, malignancy, inflammatory disorders, autoimmune diseases and bone marrow failure. The most common presentation of IEI is severe, intractable, recurrent or unusual infections caused by a single organism or a group of organisms.1 Combined immunodeficiencies result in increased susceptibility to a broad range of pathogens due to defects involving multiple components of the immune system simultaneously.
Case report
A 2-year old boy, born to non-consanguineous parents at full term, second in birth order, presented as an emergency with recurrent episodes of fever, cough and coryza since early infancy, requiring admission for the same. He also had abdominal distension since six months of age, with large, greasy, bulky stools, as well as excessive flatus, repeated episodes of loose stools, and failure to gain weight. During a previous admission at a different hospital, he was deemed to have chronic diarrhoea secondary to malabsorption, with global developmental delay, septic (paralytic) ileus, and severe acute malnutrition.
On anthropometry, both weight and height were below −3 standard deviations. His haemoglobin was 96 g/L, while total leucocyte count, differential leucocyte count, platelet count, liver and kidney function tests were within normal limits. Ultrasonography and contrast-enhanced abdominal computed tomography (CT) showed ileo-ileal intussusception, while barium enema was suggestive of functional constipation.
On microbiological examination, Shigella flexneri was isolated on stool culture. Stool microscopy also revealed Giardia lamblia cysts and fertilised eggs of Ascaris lumbricoides. Cryptosporidium oocysts were seen on modified acid-fast stain along with budding yeast cells (Fig.1). The stool specimen also tested positive for G. lamblia and Cryptosporidium spp. by enzyme immunoassay-based rapid test (Hangzhou AllTest Biotech Co., Ltd). Duodenal biopsy was suggestive of giardiasis with mild duodenitis. Blood and urine cultures were sterile. Our patient was administered ceftriaxone 600 mg intravenously od, metronidazole 360 mg intravenously qds and azithromycin 120 mg intravenously od.
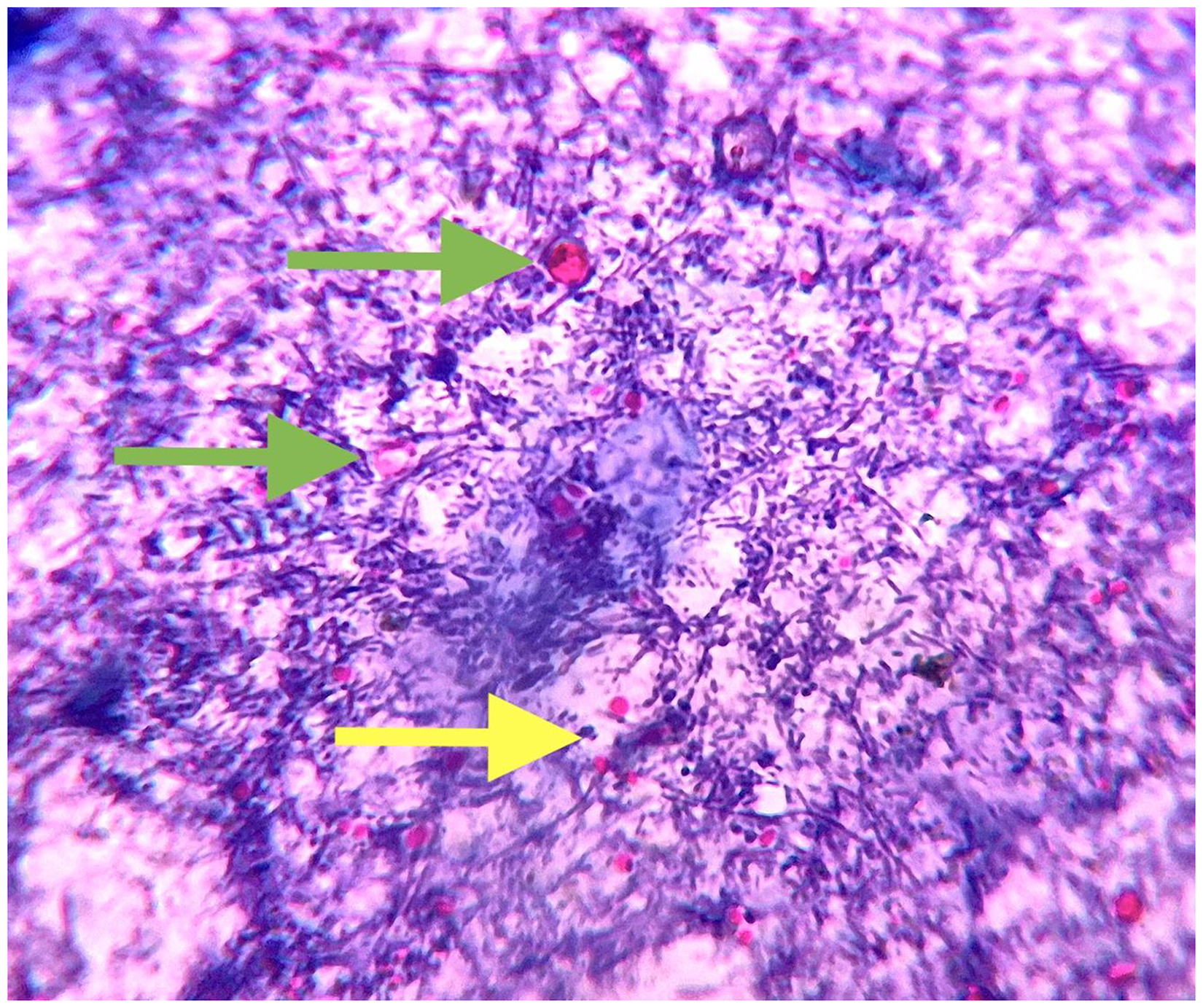
Image (at 1000× magnification) showing Cryptosporidium oocysts (green arrow) in stool specimen surrounded by budding yeast cells (yellow arrow) following modified acid-fast stain (1% sulphuric acid).
A few days later, he developed respiratory distress and was started on oxygen via nasal prongs. Meropenem 480 mg and vancomycin 180 mg intravenously qds, and salbutamol 2.5 mg nebulisation were initiated. A chest CT scan showed ground-glass attenuation of both lower lobes, peribronchial nodules, consolidation, with perihilar lymphadenopathy.
On primary immunodeficiency workup, the following findings were observed: IgG 3.25 g/L (normal: 7–16 g/L), IgA > 8 g/L (normal: 7–40 g/L), IgM > 4 g/L (normal: 4–23 g/L) CD3+ 30.2% (56–75%), CD4+ 20.9% (28–47%), CD4:CD8 ratio 0.44 (0.9–3.3), CD19 2.24% (14–33%) and CD20 2.13% (14–33%). These findings were suggestive of a combined immunodeficiency disorder.
Our patient was referred to a higher centre where his condition continued to deteriorate with frequent, intense bloody, mucopurulent stools (Fig.2) and progressing respiratory distress. The family took their child home, where he unfortunately demised two weeks later.
The diaper of the patient showing intense, bloody, mucopurulent stools.
Discussion
This case presents a complex diagnostic challenge: the clinical constellation, microbiological findings, imaging studies, and immunological profile collectively suggest an underlying combined immunodeficiency disorder, probably contributing to his recurrent infections and poor clinical progression.
Combined immunodeficiencies are usually characterised by survival beyond infancy, multiple infections appearing in the initial 2 years of age, a syndromic nature of clinical presentation, and can even present with infections, inflammatory disorders, autoimmune diseases, and malignancy in late childhood or adulthood.1,2
The child's stool microscopy, culture and enzyme immunoassay revealed multiple gastrointestinal infections. This combination is exceedingly rare, even in immuno-compromised hosts. A duodenal biopsy further contributed to confirmation of pathology. Ileo-ileal intussusception was probably caused by chronic inflammatory changes in the gut, possibly aggravated by lymphoid hyperplasia, commonly reported in immunodeficient states.
In fact, chronic diarrhoea and colitis are observed in 5% to 50% of individuals with IEI, including combined immunodeficiency.1 While multiple simultaneous gastro-intestinal pathogens have been reported in other immuno-deficiency disorders such as HIV/AIDS, their prevalence in combined immunodeficiency is rarely reported.3
Yeasts such as Candida, Saccharomyces, and Wickerhamomyces – commensals of the gastrointestinal tract – can sometimes retain carbol fuchsin and appear acid-fast, thereby mimicking coccidian parasites.4
However the most common infective syndromes associated with combined immunodeficiency are recurrent sinopulmonary infections (otitis, sinusitis, rhinosinusitis, mastoiditis, bronchitis and pneumonia) caused usually by pathogens such as Streptococcus pneumoniae, Pseudomonas aeruginosa, Staphylococcus aureus, Cytomegalovirus (CMV), Varicella zoster virus (VZV) and Pneumocystis jirovecii.1 Respiratory deterioration observed in our patient, supported by lung CT findings of ground-glass opacities, nodular consolidations, and lymphadenopathy, may suggest tuberculosis, Pneumocystis jirovecii, viral pneumonitis, or atypical bacterial infections. Although a specific organism was not identified in our case, the empiric initiation of broad-spectrum antibiotics and respiratory support was warranted.
Some of the preventive strategies against infections in individuals with IEI include avoidance of contact with sick individuals, avoiding unnecessary hospital visits, personal and environmental hygiene, use of irradiated blood products, immuno-globulin replacement, immunisation and antimicrobial prophylaxis. Therapeutic interventions such as haematopoietic stem cell transplantation and gene therapy might be necessary, especially in cases of infections that are not preventable with prophylactic measures. Therefore, accurate diagnosis is essential in determining empiric treatment of infections and other management strategies.1
Our case thus highlights the possibility of multiple simultaneous gastrointestinal pathogens in patients with immunodeficiency disorders other than HIV/AIDS. Timely diagnosis and immunological intervention are essential to improve the prognosis of such children, who otherwise face high morbidity and mortality just as AIDS victims. Although combined immuno-deficiency itself is of limited relevance to tropical practice because of its rarity and lack of curative treatment, the possibility of combined infections, as in the case described here, makes it a compelling medical entity to consider even in tropical settings.
Footnotes
Acknowledgements
The authors are grateful to our colleagues in the Department of Paediatrics and the laboratory personnel in the Department of Microbiology, Maulana Azad Medical College and the associated Lok Nayak Hospital for their support and contribution to this work.
Informed consent
Informed consent was obtained from the patient for publication of this report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.