
Abstract
Negative pressure wound therapy (NPWT) has transformed the management of complex wounds across surgical disciplines. However, widespread adoption in low- and middle-income countries is constrained by the high cost and proprietary nature of commercial systems. This narrative review examines appropriate low-cost NPWT alternatives and discusses strategies to mitigate commonly cited limitations through protocol-driven care. Wider adoption supported by pragmatic evaluation and standardized protocols offers an opportunity to expand equitable access to advanced wound care in resource-constrained settings.
Keywords
Introduction
The application of effective negative pressure wound therapy (NPWT) has revolutionized the outcome of complex wounds. By applying controlled suction over a sealed wound environment, NPWT reduces infection and accelerates healing.1,2 This understanding, as ‘glass cupping’, was used in earlier centuries to promote healing. More efficient and effective methods were developed during the Russian–Afghan war by Nail Bagautdinov in 1985. 3 The technique and technology was subsequently pilfered and publicized from the USA without regard to its inventor,1,2 leading to legal battles over patents and proprietary and rights. 4
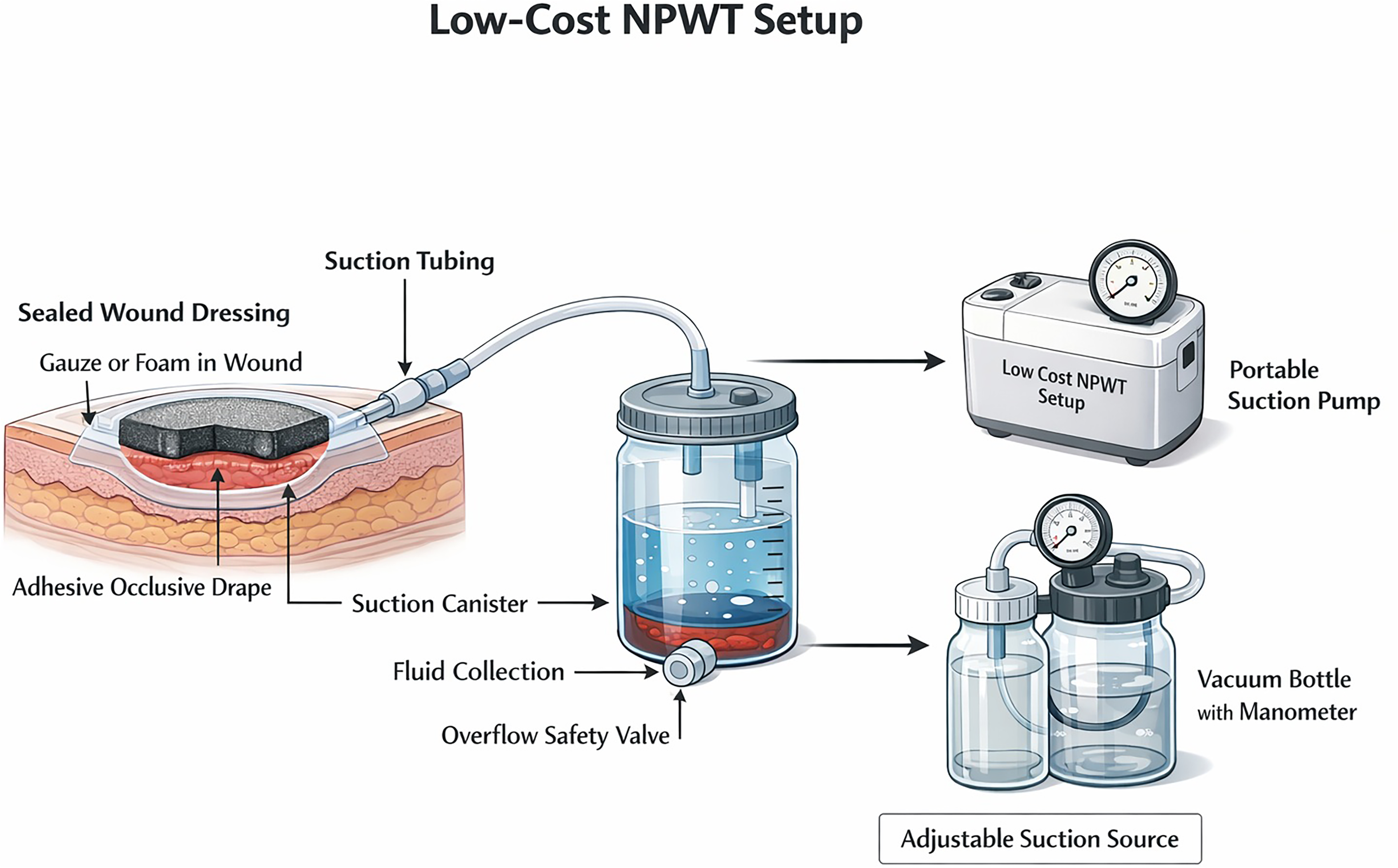
NPWT involves placing a porous interface (usually foam or gauze) into the wound bed, sealing the wound with an adhesive drape, and applying controlled negative pressure through a vacuum source to evacuate exudate (Fig. 1). The core therapeutic mechanisms include
1
as follows:
Macro-deformation: Bringing wound edges together. Micro-deformation: Mechanical stimulation of cells that promotes angiogenesis and granulation tissue formation. Fluid management: Continuous removal of exudate and bacteria-laden fluid, reducing local oedema and bacterial bio-burden.
Schematic representation of a negative pressure wound therapy (NPWT) system.
These effects translate into faster granulation, reduced dressing frequency, lower infection rates, and accelerated healing. These benefits have been documented across trauma, orthopaedic, plastic, vascular, and general surgery.5,6 NPWT has accordingly become a go-to tool for suboptimal wounds.
However, the high cost and proprietary nature of commercial devices limit accessibility in low- and middle-income countries (LMICs) and resource-poor clinical settings. Despite strong evidence for NPWT benefits, equity of access remains a global challenge. Commercial NPWT systems (e.g. VAC systems, portable battery-powered units) are typically designed for hospital infrastructure in high-income settings and their high cost reflects the following:
Specialized engineering: Accurate pressure sensors, vacuum pumps, feedback systems, and safety alarms require precision design. Proprietary consumables: Dressings, canisters, and tubing are designed for sterility and performance, and often have no generic alternatives due to patent protection. Regulatory compliance: Devices must meet strict medical device regulations, which increase development and testing costs. Service infrastructure: Customer support, training, maintenance, and warranty services are bundled into price. Market structure: Low volume of high-end buyers and limited competition keep prices elevated.
Thus, the costs of NPWT lead to prices of $1000–2000 US (with additional costs of c. $75 per change of dressing. This drastically limits use in low-resource contexts, where the burden of complex wounds is highest from trauma, infection, diabetes, and vascular disease. In such contexts, low-cost NPWT models provide a pragmatic option that preserves the clinical advantages of NPWT while overcoming financial barriers to care. Such systems follow similar principles using locally available components (Fig. 2) and cost $5-10 to make and < $5 for each dressing change.
7
Core components of a basic model include:
Sealed wound dressing: Sterile gauze and foam. Occlusive drape: Transparent adhesive film or op-site equivalents. Suction source: Wall suction, portable suction machine, or vacuum bottles with manometer. Collection reservoir: Sterile jar or suction canister. Tubing and connectors: Standard suction tubing, three-way connectors.

Locally available material to assemble negative pressure wound therapy (NPWT) system.
While commercial NPWT systems are technologically sophisticated, many of their advantages relate to automation rather than fundamentally different wound-healing science. In low-resource settings, inability to use intermittent suction, non-portability, the need to treat patients on an inpatient basis, an absence of built-in pressure sensors, alarms, or proprietary foams have all been cited as a limitation of improvised NPWT systems. 7 However, these limitations may be effectively mitigated through simple, low-cost strategies (Table 1).
Commercial versus low-cost NPWT: Limitations and pragmatic solutions.
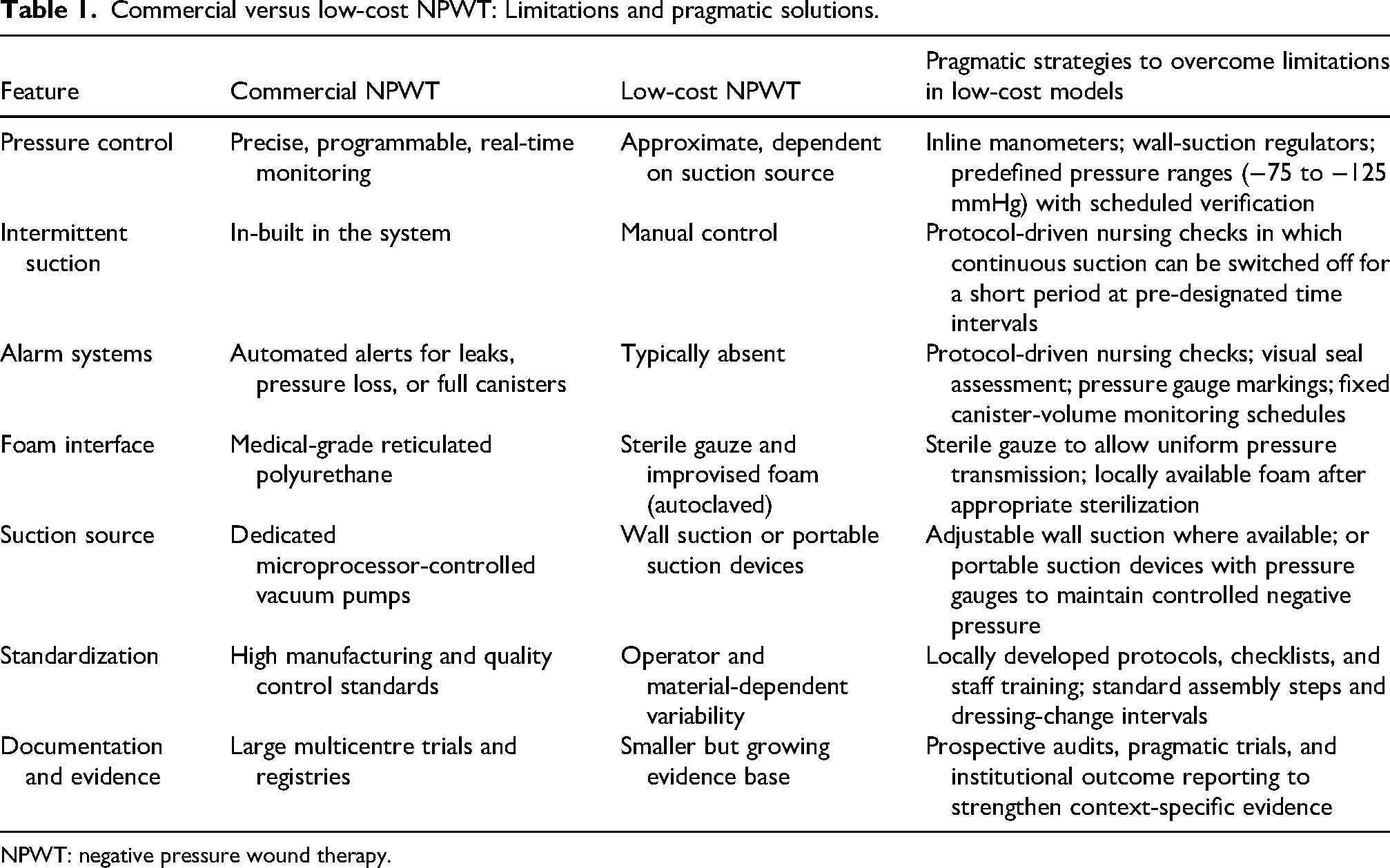
NPWT: negative pressure wound therapy.
Discussion
NPWT has become an integral component of modern wound care because it addresses fundamental biological processes underpinning wound healing: removal of excess exudate, reduction of tissue oedema, mechanical stimulation of granulation tissue, and maintenance of a protected wound environment. Importantly, these mechanisms are independent of the proprietary nature of the delivery device. Commercial NPWT devices offer automation, precision engineering, and built-in safety features to reduce reliance on human monitoring. In contrast, low-cost NPWT systems intentionally trade automation for affordability, adaptability, and scalability. They illustrate how effective surgical technology can be recreated to align with the realities of resource-constrained health systems. This is a successful contextually appropriate adaptation of the same therapeutic principle for settings where commercial solutions are neither affordable nor sustainable. By prioritizing affordability, availability, and system compatibility overautomation, such an approach ensures advances in wound care are accessible, equitable, and responsive to local needs.
By using readily available materials and familiar suction sources, these systems do not require additional capital investment or specialized maintenance. 7 The reliance on protocol-driven monitoring rather than automated alarms further aligns with settings where human resources are available but advanced technology is not.
Low-cost NPWT limitations, when examined pragmatically, can be mitigated through simple solutions (Table 1). In such environments, process reliability can substitute for device complexity, a principle well recognized in global health delivery models.
Importantly, the growing body of observational studies, pragmatic trials, and institutional audits from LMICs suggests that low-cost NPWT can achieve outcomes comparable to commercial systems.8,9 While large multicentre randomized trials remain limited, this reflects structural research inequities rather than lack of clinical effectiveness. Implementation-focused evidence—cost-effectiveness analyses, feasibility studies, and real-world outcome reporting—may be more relevant than traditional efficacy trials when evaluating such innovations.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.