
Abstract

Keywords
Sir,
We read with interest the report of a 49-year old man from South India with disseminated melioidosis and recurrent pulmonary disease. 1
Recently, we had a case of pulmonary melioidosis in a patient from Mexico. The main endemic areas for melioidosis are Asia and Australia, including Puerto Rico in Latin America, 2 but in Mexico, this disease is not common. We present a case highlighting differences and important lessons not previously mentioned.
Our 52-year old man from Paso del Cedro, Veracruz, with a history of type 2 diabetes, treated with insulin 30 IU od, was admitted after surviving drowning while rescuing his cattle from a flood caused by tropical storms. He initially had a cough, fever, general malaise, and chills. A week later, on admission, he was dyspnoeic, febrile (38.9 °C). On physical examination, hepresented with pallor, drowsiness, respiratory rales, abdominal breathing with a respiratory rate of 26 breaths per minute, a blood pressure of 135/75, and an oxygen saturation of 89%, and tachycardia of 123 beats per minute. The initial chest radiograph showed consolidation in the right lung. Results showed no anaemia (Hb 150 g/L), a leucocytosis (18.0 × 109/L, with neutrophils 14.0 × 109/L), hyperglycaemia (glucose 23.59 mmol/L), but normal creatinine (110 µmol/L), and platelet (330 109/L) levels. A lung CT scan revealed cavitation in the left hemithorax (Fig. 1A), thus suggesting a diagnosis of pulmonary tuberculosis (TB), for which antitubercular therapy (ATT) was initiated.
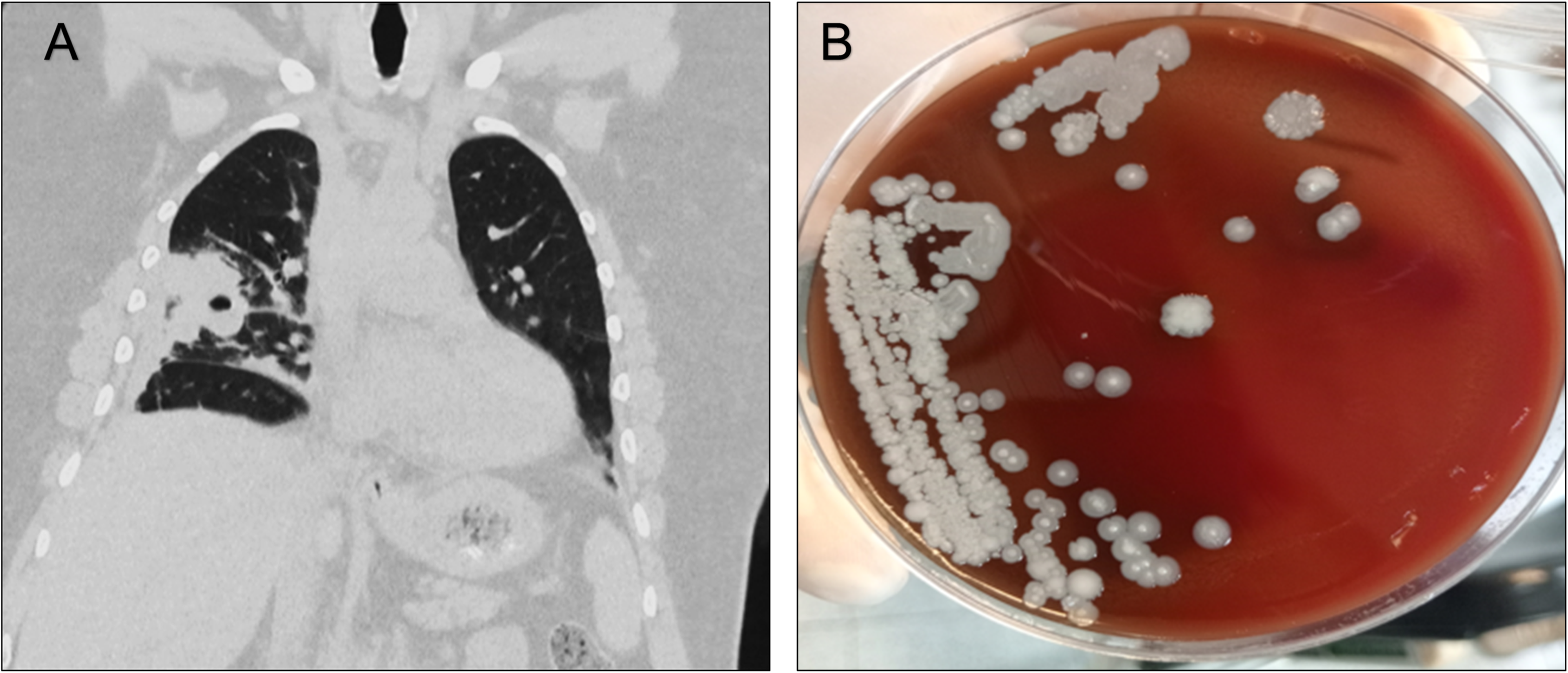
A) Chest CT Scan simple coronal section, showing cavitation in the right hemithorax and consolidation areas. B) Blood agar with the growth of Burkholderia pseudomallei bacilli.
Despite two months of this, prostration continued with fever, with the formation of pressure ulcers, episodes of delirium, and pain and swelling of the left knee. Culture of arthrocentesis grew Burkholderia pseudomallei, thus diagnosing melioidosis (Fig. 1B) instead of TB. ATT was therefore discontinued, and substituted by meropenem 1 g tds for four weeks, trimethoprim/sulfamethoxazole 160/800 mg bd, together with blood transfusions on two occasions. Subsequently, the fever and dyspnoea subsided, and his laboratory results now showed only an anaemia (Hb 70 g/L). An additional unit of packed red blood cells was transfused. Another blood culture showed no growth after 48 h, allowing discharge and rehabilitation.
In Mexico, melioidosis is little known by physicians, 3 which will be an obstacle to its diagnosis. In Kamat's patient, 1 there was disseminated melioidosis with abscess formation in the liver, a characteristic of the disease. 4 In contrast, the dissemination in our patient was from the lung to the knee joint. Our patient reported exposure to flood waters, which have been related, on an increased number of cases, to melioidosis infection. 5 Treatment for Burkholderia pseudomallei followed standard advice, since no antibiograms are available for this pathogen in Mexico.2,3 The most important lesson is distinguishing between pulmonary TB and melioidosis, particularly in TB-endemic regions. Inappropriate treatment had led in our case to two months’ delay resulting in severe febrile illness, delirium, and decubitus ulceration, narrowly avoiding death.
Footnotes
Patient consent
Written informed consent was obtained from the patient for publication of this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.