
Abstract
Leptospirosis is a zoonotic infection predominantly affecting marginalized populations in tropical regions, often resulting from exposure to contaminated water or contact with animal reservoirs, especially rodents. The disease typically manifests in a biphasic nature; beginning with an incubation period ranging from several days to a few weeks, followed by a septicaemic phase, an interphase where symptoms resolve temporarily, and finally an immune phase. While most infections are mild, approximately 10% progress to severe disease involving multi-organ complications, typically manifesting during the immune phase. We report a case of myocarditis and septic shock during the acute phase of leptospirosis.
Case report
A 43-year old male was referred to our hospital with an initial diagnosis of ST-elevation myocardial infarction. He presented initially with a high fever for three days, accompanied by severe abdominal pain in all quadrants, persistent diarrhoea and vomiting >10 times a day, with no evidence of blood staining. He gave a history of actively smoking 240 pack-years.
Upon arrival, he was hypotensive (blood pressure 70/43 mmHg) with hypoxia (oxygen saturation 89% on room air). The initial electrocardiogram showed ST-segment elevation in leads V1–V3, leading to an assessment of anteroseptal myocardial infarction and referral for primary coronary intervention.
When he arrived at our emergency department, he had developed worsening abdominal pain, increased shortness of breath and ongoing diarrhoea.
There was no history of an underlying medical condition, and he was currently employed as a garbage collector.
On examination, he was lethargic, hypotensive (blood pressure 87/51 mmHg) while receiving norepinephrine at 0.3 µg/kg/min and dobutamine at 5 µg/kg/min, tachycardic (rate 122 bpm), febrile (temperature 39°C), with oxygen saturation 99% with simple mask at 10 L/min. There was conjunctival suffusion, icteric sclera, bilateral pulmonary crackles and abdominal tenderness in all quadrants. No gastrocnemius pain was elicited. Chest radiography demonstrated increased bilateral pulmonary vascular markings.
Laboratory evaluation showed thrombocytopenia (platelet count 47 × 109/L), hypoglycaemia (blood glucose 3.22 mmol/L, hyperbilirubinemia (total bilirubin 0.026 mmol/L), with impaired renal function (creatinine 0.25 mmol/L, eGFR 25.7 mL/min/1.73 m2, with markedly elevated lactate (4.4 mmol/L), procalcitonin (>100 ng/mL) and troponin levels (1238 ng/L).
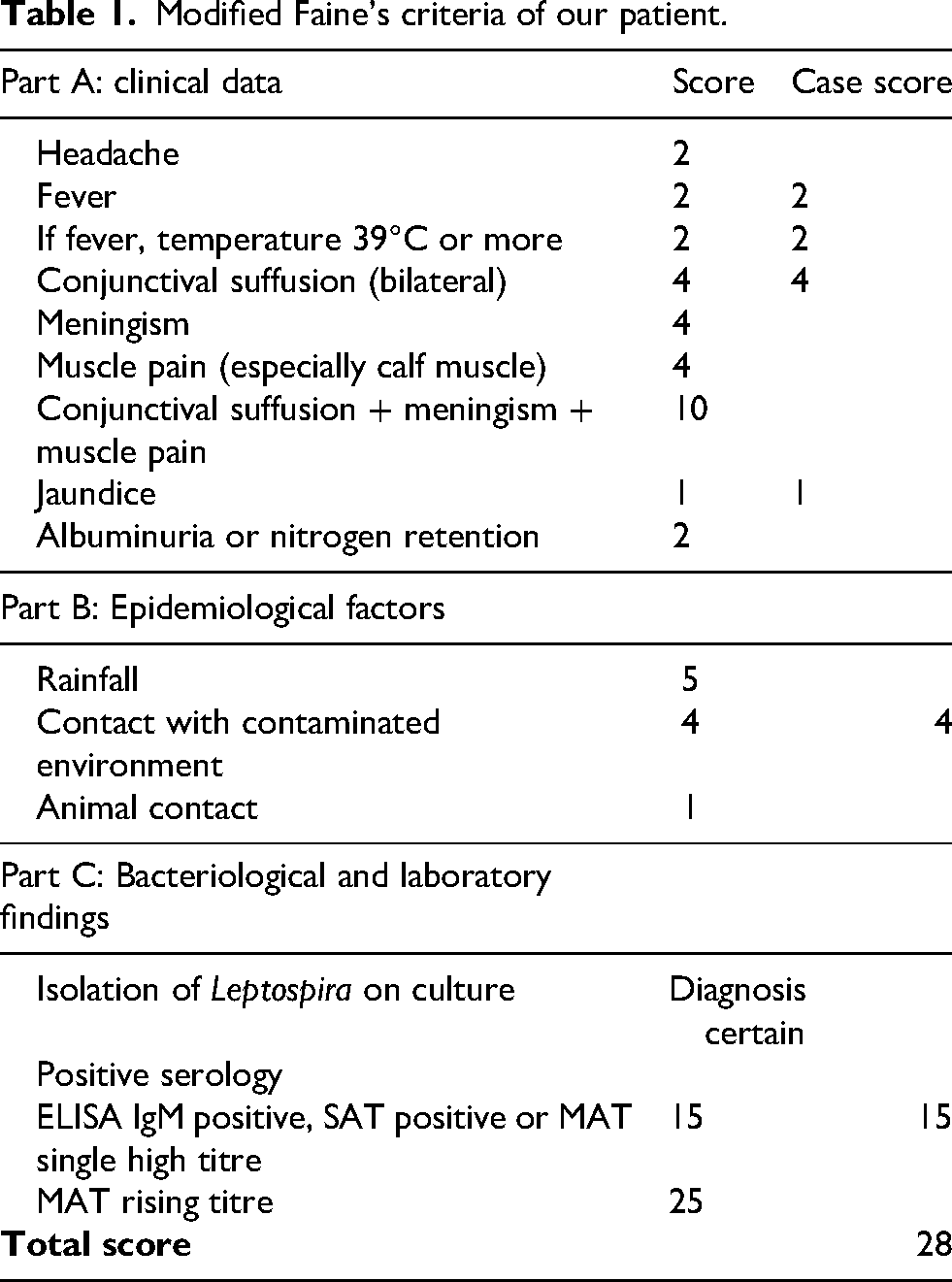
Assessment using the modified Faine's criteria 1 yielded a score of 13 without laboratory test (Table 1).
Modified Faine’s criteria of our patient.
Bedside abdominal and cardiac ultrasound showed no significant abnormalities. Owing to his persistent severe abdominal pain, an abdominal CT scan with contrast was performed, revealing only mild bowel inflammation.
Ultimately, IgM anti-leptospiral antibody test was shown to be positive. Treatment with Meropenem for seven days caused his symptoms to resolve. Vasoconstrictors were gradually reduced after three days of antibiotics and discontinued after five days.
Discussion
Leptospira bacteria enter the human body through abrasions, open wounds or mucous membranes. After entry, they are disseminated via the bloodstream to various organs – including the liver, spleen, lungs and kidneys. 2 Notably, unlike most bacterial pathogens whose lipopolysaccharides are recognized by Toll-like receptor 4 (TLR-4), Leptospira is primarily detected by TLR-2, which initiates intracellular signaling cascades activating nuclear factor kappa B and activator protein-1. These signaling pathways induce the production of prostaglandins, nitric oxide and pro-inflammatory cytokines such as interleukin (IL)-6, IL-2, IL-1β, tumour necrosis factor-alpha and interferon gamma. 3 In susceptible individuals, cytokine production may be delayed and sustained, potentially triggering a cytokine storm and subsequent sepsis-like manifestations. As in our case, our patient presented with extremely high procalcitonin levels and life-threatening organ damage, requiring a high dose of vasoconstrictor support. 4
Although diagnostic modalities such as culture, serological testing and molecular techniques are available, clinical assessment remains the cornerstone of disease diagnosis in resource-limited settings. In 1982, the World Health Organization introduced Faine's criteria for the diagnosis of leptospirosis, which integrate clinical presentation and epidemiological exposure, supported by laboratory findings. 5 In 2012, these criteria were revised to improve diagnostic performance (sensitivity: 41.9% vs. 58%, specificity: 84.9% vs. 97.4%) by incorporating rainfall as an epidemiological parameter and rapid immuno-chromatographic assays as a laboratory component, thereby enhancing practicality and usability. 1 A Modified Faine's criteria score of ≥26 is considered diagnostic. In our case, the clinical and epidemiological components yielded a total of 13 points. If the laboratory component were positive, the cumulative score would reach 28, thereby meeting the diagnostic threshold.
Consequently, further evaluation was pursued using rapid immuno-chromatographic assays.
Myocarditis, pulmonary injury and kidney failure associated with leptospirosis typically arise during the immunogenic phase, approximately between days 5 and 7 post-infection, when a cytokine storm provokes myocardial inflammation. 4 Histopathological analysis frequently shows epicardial mononuclear cell infiltration and interstitial myocarditis. Some studies have also reported endothelial proliferation without evidence of atherosclerosis or infarction, suggesting coronary artery endotheliitis. These findings indicate that ST-segment elevation observed in leptospirosis patients may not necessarily indicate myocardial infarction. 6 Thrombocytopenia, as seen in our case, may reflect platelet consumption due to immune-mediated platelet destruction caused by antiplatelet antibodies and inhibited platelet production by the bone marrow.
We suspect that, owing to a history of active smoking totaling 240 pack-years, microvascular endothelial damage occurred in our patient. When Leptospira enters and a cytokine storm ensues, endothelial oedema can ensue, allowing bacteria to enter the systemic circulation more readily, which may accelerate septicemia and precipitate earlier organ damage. Fortunately, our patient recovered with antibiotic therapy.
Conclusion
Leptospirosis still poses a major problem, especially in areas dealing with poor hygiene and sanitation. Most cases were mild or asymptomatic, but about 10% may be life-threatening. Leptospirosis usually manifests in a biphasic course, and severe manifestations typically occur during the second phase. Our case serves as a reminder that in patients with risk factors for microvascular endothelial damage, severe manifestations of septicaemia in leptospirosis may occur earlier.
Footnotes
Informed consent statement
Patient had given approval for his information to be published in this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.