
Abstract
Methotrexate, a commonly used disease-modifying anti-rheumatoid drug, rarely causes bone marrow suppression and pancytopenia. Consequently, we made a retrospective analysis of all patients who were admitted with pancytopenia following low-dose methotrexate intake between 2019 and 2025. Factors that were associated with the development of toxicity, clinical features and outcomes were evaluated. Among those who developed early toxicity, the majority had inadvertently taken daily instead of weekly doses. Renal failure, elderly age and hypoalbuminaemia contributed to delayed toxicity. All were given Folinic acid rescue therapy and 20% needed transfusion support. Two succumbed due to severe neutropenia-related sepsis. Simple patient education on once a week use, dose adjustment and frequent monitoring in the elderly and those with renal failure may help to reduce toxicity.
Introduction
Methotrexate at its low, once weekly dose, used as a disease-modifying anti-rheumatoid drug (DMARD), has a very favourable efficacy/toxicity ratio and is well tolerated. It acts by inhibiting the action of dihydro-folate reductase, an enzyme responsible for converting this to tetrahydro-folate. This results in a decrease in thymidylate and purine biosynthesis and eventually causes a halt to cell replication. 1 This mechanism is responsible for many of the side effects of methotrexate including mucositis, haematological toxicity causing bone marrow suppression, pancytopenia and increased risk of infection.
Studies have shown clinically significant pancytopenia in 1–2% of patients on methotrexate therapy for rheumatoid arthritis. 2 Concomitant administration of folic acid at 1–3 mg/day doses decreases the frequency of toxicity. 3
Materials and methods
Ours was a retrospective study conducted at a tertiary care hospital in Chennai, India.
All adult patients >18 years of age, who were taking methotrexate therapy and admitted to the hospital with pancytopenia between June 2019 and May 2025 were included. Permission was obtained from the hospital ethics committee with waiver of informed consent in view of the retrospective nature of the study.
Pancytopenia was defined as a haemoglobin <120 g/l, total white cell count (WBC) < 4 × 109/l and platelets of <150 × 109/l. 4 Severe pancytopenia was defined as Hb <100 g/l, WBC <2.0 × 109/l, and platelet count <50 × 109/l.
Patients were divided into two groups – those who developed symptoms within a year of starting the drug and those beyond one year. Data were analysed using SPSS software version 23.
Results
A total of 24 patients with methotrexate-induced pancytopenia were included of whom 16 were female. Its most common indication was Rheumatoid Arthritis (15 patients), followed by psoriatic arthritis (5 patients) 5 and one each of ankylosing spondylitis and vitiligo. Twelve were started on the drug by private practitioners and subsequently referred to our hospital after they had developed complications. Background details of the two groups are given in Table 1.
Background details, clinical features and complete blood count.
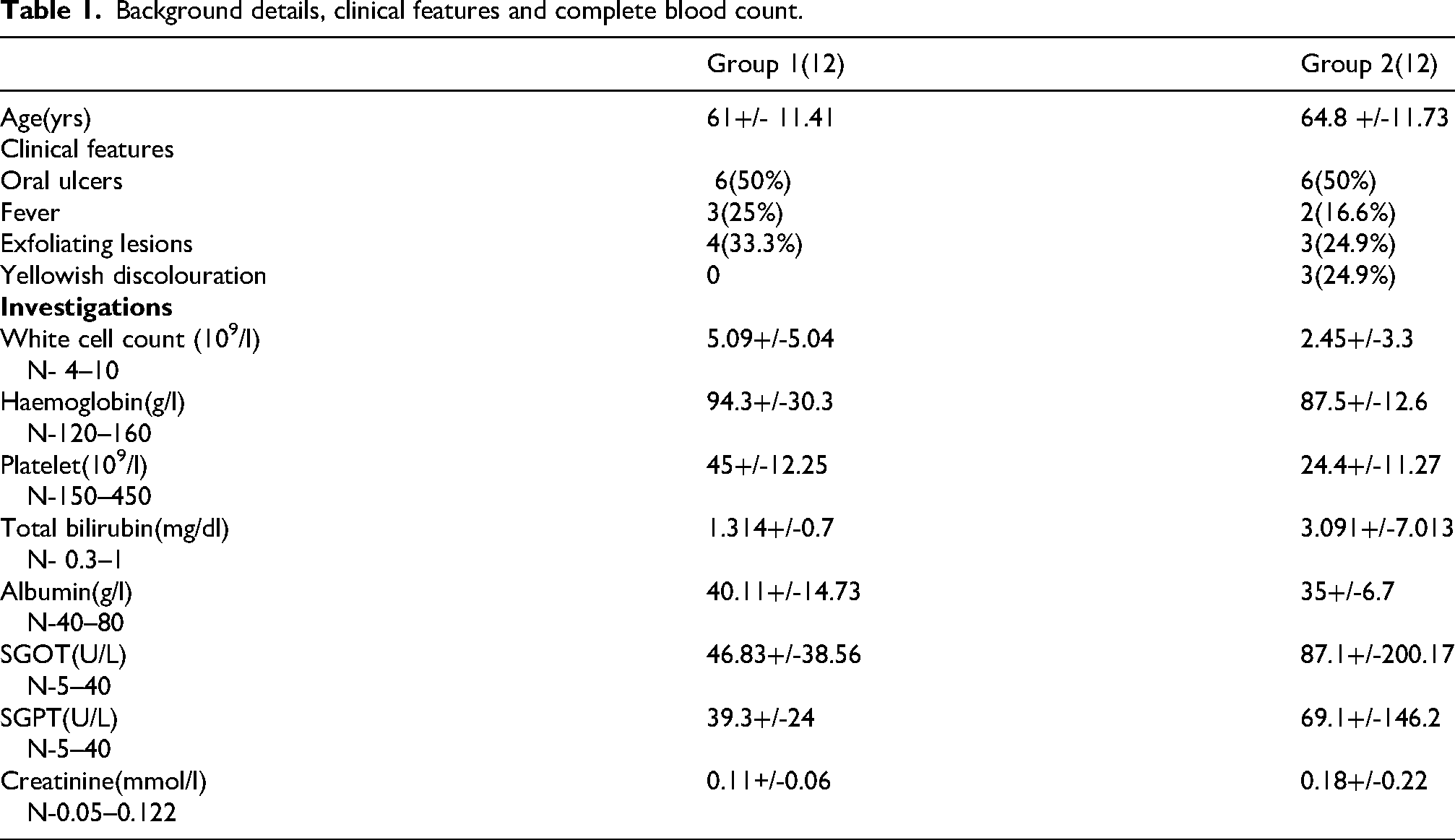
Some 18 patients received regular folic acid supplementation (5 mg per day for 6 days per week), four were advised folic acid but took it infrequently, and two did not take any.
The mean age of patients was 61+/- 11.4 in the first group and 64.8 +/-11.7 in the second with the lowest age being 28 and the highest 88. Six developed toxicity within 10 days of starting drug, six more within a year, four had used the drug between 1 and 5 years, and eight had taken it for >5 years. Among those who developed toxicity within the first 10 days, 5/6 (83%) took the drug daily instead of once weekly. All the others were taking the recommended once-a-week dosage.
The most common presenting symptom was oral ulceration (12 patients) due to mucositis. Fever was seen in five, and exfoliating skin lesions in seven. Some were detected after routine blood investigations done as part of monitoring. Many were taking other drugs including NSAIDs, hydroxychloroquine, PPIs, or low-dose steroids concomitantly. Twelve patients had severe pancytopenia.
All were treated with intravenous folinic acid at 15 mg qds as rescue therapy. Granulocyte colony stimulating factor was administered in 12, and one received Elthrombopag.
Nearly 20% needed transfusion support: four had platelet concentrates and three received packed red cell transfusions. Two patients in the second group succumbed, both having absolute neutrophil counts of <150 × 109/L and had developed septicaemia.
Discussion
Methotrexate, first introduced in the 1980s as a treatment for rheumatoid arthritis, 6 remains a commonly used DMARD even after the advent of biological agents. It should be started at a dose of 5–10 mg/week and slowly increased to a maximum dose of 25 mg/week. It acts through multiple mechanisms, including folate antagonism, adenosine signalling, generation of reactive oxygen species, decrease in adhesion molecules, alteration of cytokine profiles, and polyamine inhibition. 1
Side effects of low-dose methotrexate are mainly gastrointestinal, whereas other side effects such as stomatitis, hepatotoxicity, skin rash, hair loss, pulmonary and haematological toxicity are encountered less frequently. 5
Haematological complications were seen in acute, subacute and chronic users of methotrexate. Acute pancytopenia is thought to be an allergy-like reaction with rapid onset, while the progression in chronic pancytopenia is insidious. 5
Almost all patients who developed pancytopenia within ten days of commencement were using incorrect dosage daily instead of weekly, and all were elderly. Worldwide, such medication errors are most common. 7 Time therefore spent explaining with patience how to take the drug weekly together with early monitoring gives dividends.
Among those who developed pancytopenia after a longer duration of therapy, renal failure (5/12), hypalbuminaemia (3/12) and age>65 years were found to be contributing factors. As methotrexate is filtered by glomeruli and undergoes tubular secretion and reabsorption, age-related renal insufficiency is an obvious contributory factor to toxicity. 8 Hypalbuminaemia also results in increased levels of free drug as lower binding to serum albumin occurs, resulting in increased myelotoxicity. 9
The elderly are also at higher risk of toxicity owing to hepatic and renal dysfunction, polypharmacy and unintentional forgetful consumption of extra drug doses. 10
Footnotes
Author contributions
SG was involved in concept, design, and drafted the article. PD was involved in acquisition of data, interpretation, and approved final version of article. PA was involved in concept, revised article and approved final version.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.