
Abstract
Methanol poisoning is a life-threatening condition frequently associated with severe metabolic acidosis, organ failure, and death, particularly in low- and middle-income countries. Early identification of patients at high risk of deterioration is essential for timely intensive management. Unfortunately, patients typically present late after ingestion. Most required intensive care support.
Introduction
Methanol poisoning remains a major cause of morbidity and mortality worldwide, where illicit alcohol consumption is common.1–3 Toxicity results from the accumulation of formic acid, leading to severe metabolic acidosis, visual impairment, and multi-organ failure.4,5
Clinical presentation is often delayed and heterogeneous, making early risk stratification challenging. Several parameters have been associated with poor outcomes, including methanol concentration and arterial pH. The identification of simple and reliable clinical markers to guide early decision-making is crucial.
Methods
Ours is a retrospective observational study conducted at the Emergency Centre of Thai Nguyen Medical University Hospital, Vietnam.
We included consecutive adult patients admitted with confirmed methanol poisoning between February 2021 and August 2024. Diagnosis was confirmed by blood methanol concentration. Patients with co-ingestion of other toxic alcohols without methanol confirmation were excluded.
Data were extracted from medical records, including:
- demographic characteristics, - time from exposure to hospital presentation, blood methanol concentration, - arterial blood gas parameters, treatment modalities, and clinical outcomes. - intensive care need, - mechanical ventilation, vasopressor requirement, renal replacement therapy or death.
Severe outcome was defined as more than one of the following:
Continuous variables were summarized as mean ± SD or median (IQR), and categorical variables as frequencies and percentages. Comparisons between groups were performed using appropriate statistical tests. Multivariable logistic regression analysis was conducted to identify independent predictors of severe outcomes. A p-value < 0.05 was considered statistically significant.
Given the relatively small sample size and the predominance of severe cases in this cohort, results from multivariable analysis should be interpreted with caution.
Results
A total of 31 patients were included, with a median age of 55 years; 93.5% were male. Most presented late after ingestion, with a median delay of 48 h.
Severe outcomes occurred in 83.9%, the majority requiring intensive care (67.7%), with many developing respiratory failure (58.1%), shock, or needing renal replacement therapy (74.2%), with a mean delay of 28 h.
Patients with severe outcomes had lower Glasgow Coma Scale scores and significantly higher methanol concentrations. Other clinical and laboratory parameters were not consistently associated with severity.
All patients received ethanol as an antidote.
In multivariable analysis, methanol concentration was the only independent predictor of severe outcome (OR 1.043, 95% CI 1.006–1.082; p = 0.022). Arterial pH was not independently associated with severity.
Discussion
A notable finding is the very high proportion of severe cases, reflecting the real-world burden of methanol poisoning in our referral centers. Delayed presentation contributes to the high rates of metabolic complications, organ failure, and need for intensive care.3,5
Methanol concentration emerges as the most clinically relevant predictor of severity. This is biologically plausible, as higher methanol levels lead to greater accumulation of formic acid, the primary toxic metabolite responsible for metabolic acidosis and cellular injury.4,6
In contrast, arterial pH was not independently associated with severe outcomes; although it is a hallmark of methanol poisoning, pH may be influenced by multiple factors, including timing of presentation, prior treatment, and individual physiological responses.7–9 In clinical practice, methanol concentration therefore seems to provide a more direct and stable indicator of toxic burden.
From a clinical perspective, this finding has important implications; in resource-limited settings, where access to advanced monitoring may be restricted, early measurement of methanol concentration may therefore help identify patients at high risk of deterioration. Those patients with elevated methanol levels should be considered for early intensive care, close monitoring, and timely initiation of extracorporeal treatment, preferably before severe acidosis develops.1,2
Baseline characteristics of patients with acute methanol poisoning according to outcome severity.
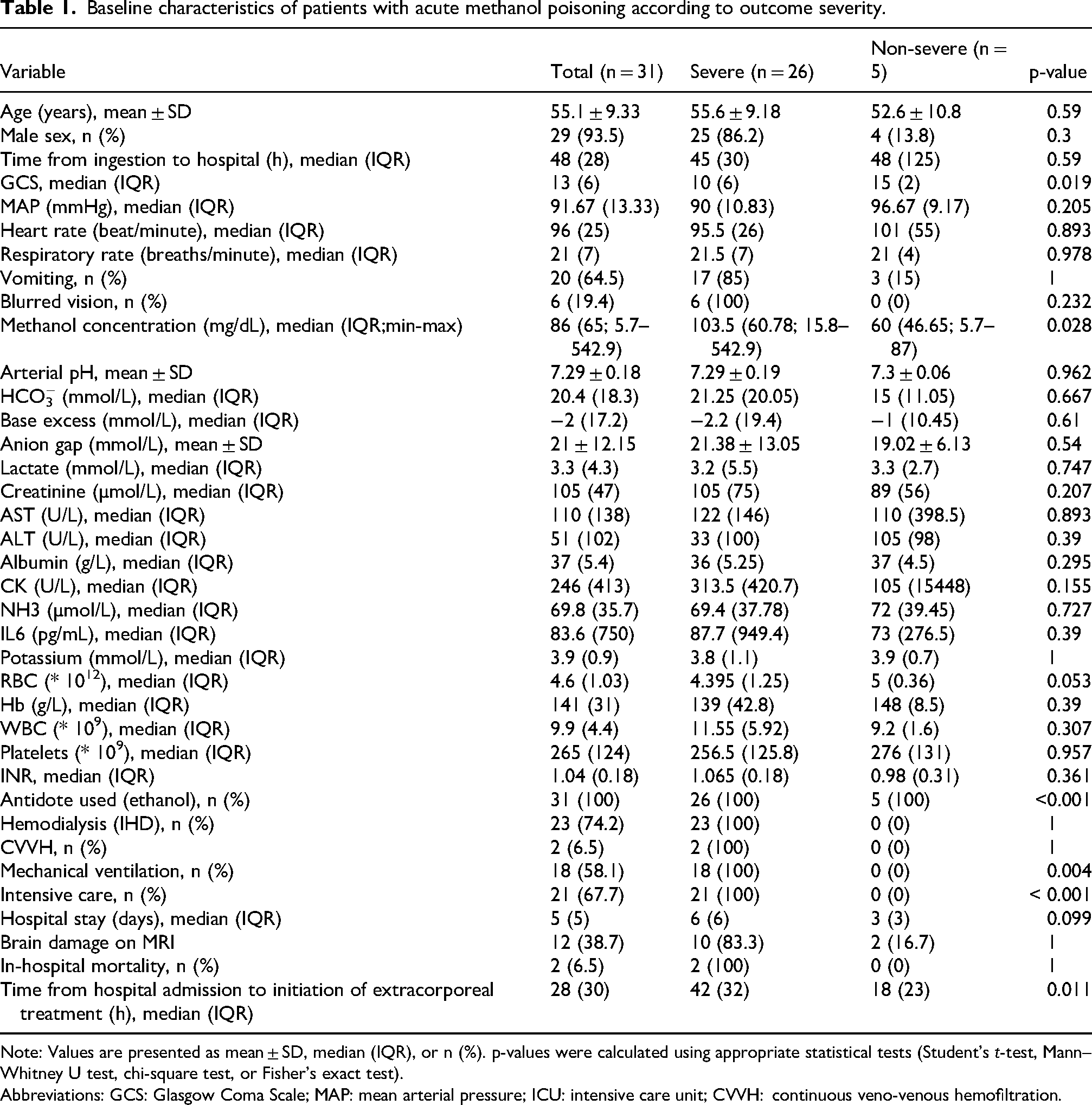
Note: Values are presented as mean ± SD, median (IQR), or n (%). p-values were calculated using appropriate statistical tests (Student's t-test, Mann–Whitney U test, chi-square test, or Fisher's exact test).
Abbreviations: GCS: Glasgow Coma Scale; MAP: mean arterial pressure; ICU: intensive care unit; CVVH: continuous veno-venous hemofiltration.
Multivariable logistic regression analyses of predictors of severe outcome.

Multivariable model: methanol concentration + arterial pH.
Footnotes
Ethical approval
Approved by the Institutional Review Board of Thai Nguyen Medical University Hospital (Approval No. TNMUH-2021-2).
Consent to participate
Waived due to retrospective design.
Author contributions
NDD drafted and revised the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Data available from the corresponding author upon reasonable request.