
Abstract
Diarrhoeal illnesses in renal transplant recipients are common in tropical regions but may have significant implications beyond gastro-intestinal morbidity. Cryptosporidiosis, although common in tropical settings, may present as acute allograft dysfunction through a haemodynamic mechanism, closely mimicking rejection. Recognition of this reversible cause is essential to avoid unnecessary escalation of immuno-suppression and to ensure timely management. Gastro-intestinal infections are often considered benign and self-limiting, but their systemic consequences in immunosuppressed hosts are frequently under-recognised.
Case report
A 34-year old male with end-stage kidney disease secondary to IgA nephropathy underwent live-related ABO-compatible renal transplantation in 2019. He previously had 18 months dialysis via a left radiocephalic arterio-venous fistula. Post-transplant, his lowest creatinine reached was 70 µmol/L, and he was maintained on tacrolimus (3 mg bd), mycophenolate mofetil (1 g bd), and prednisolone (10 mg od).
He presented with a 1-week history of diarrhoea, characterized by approximately five episodes of watery stools per day. On admission, he was hypotensive (90/60 mmHg) with a tachycardia of 96/min, but his remaining systemic examination was unremarkable.
Laboratory evaluation revealed a rise in serum creatinine from 76 µmol/L to 120 µmol approximately 1 week later. His haemoglobin was 91 g/L, total leucocyte count 7.6 × 109/L, and platelet count 216 × 109/L. Urinalysis was normal. Tacrolimus trough level was 8.4 ng/mL. Blood and urine cultures were sterile, and cytomegalovirus DNA PCR was negative.
Given his persistent diarrhoea, stool examination using modified acid-fast staining was performed and demonstrated oocysts of Cryptosporidium (Fig. 1). Mycophenolate mofetil was switched to enteric-coated mycophenolate sodium (720 mg bd), but diarrhoea persisted, suggesting an infectious rather than drug-induced aetiology.
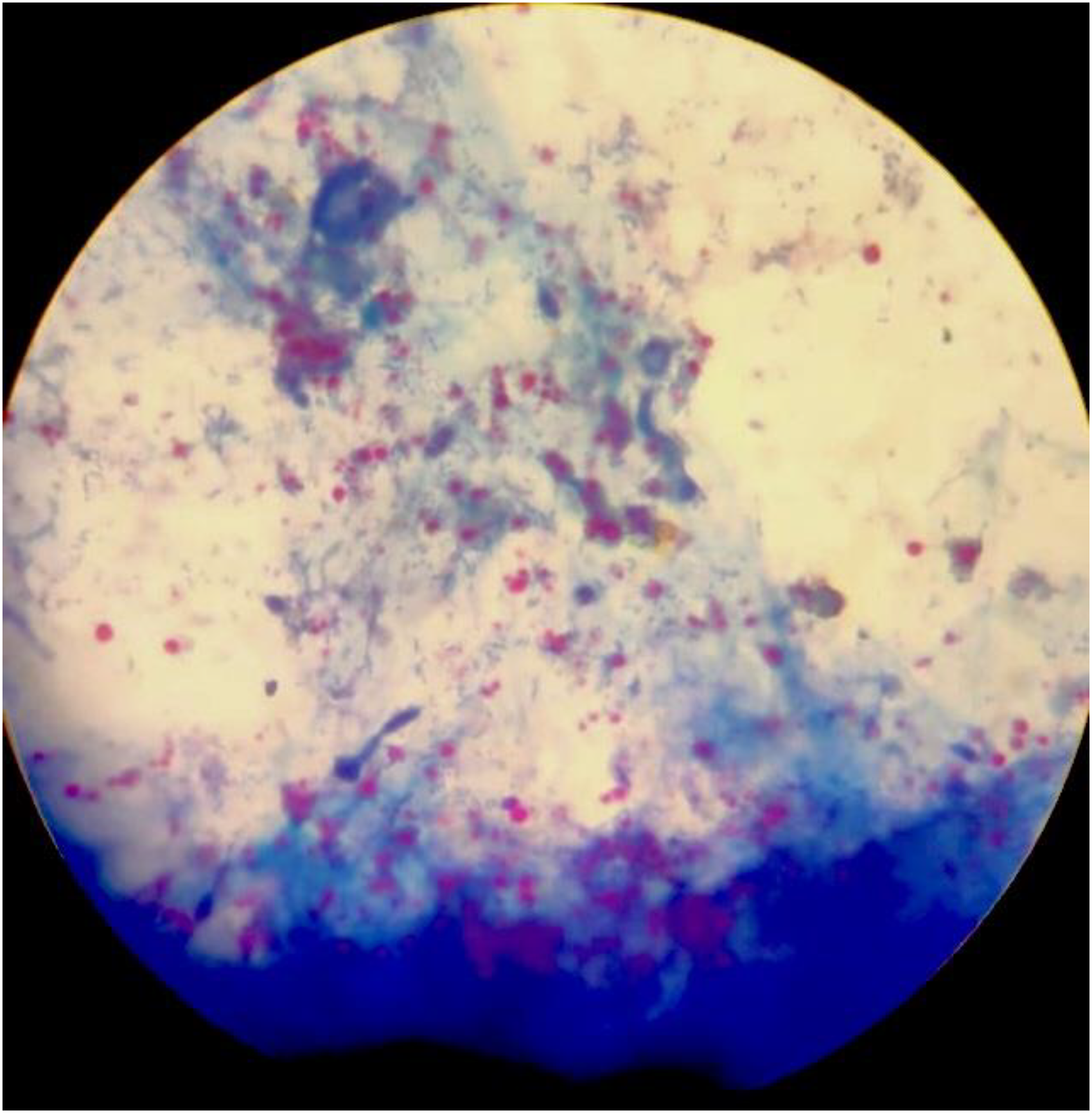
Modified acid-fast stained stool smear showing multiple acid-fast oocysts of cryptosporidium (pink-red spherical structures) against a blue background.
Nitazoxanide 500 mg bd for 2 weeks was started with intravenous rehydration, and with targeted therapy and supportive management, diarrhoea resolved with subsequent normalization of renal function to 80 µmol/L over the following 2 weeks.
Discussion
Cryptosporidiosis is a well-recognised cause of diarrhoea in immuno-compromised individuals, particularly in tropical regions where environmental exposure is common.1,2 In renal transplant recipients, the infection may be prolonged and severe, reflecting impaired cellular immunity. This distinction is particularly important in transplant settings, where an incorrect diagnosis of rejection may lead to inappropriate intensification of immuno-suppression.
Beyond gastro-intestinal symptoms, diarrhoeal illness may significantly impact graft function by inducing intravascular volume depletion, electrolyte disturbances, and alterations in the pharmacokinetics of immunosuppressive agents.1,3
Cryptosporidiosis is recognized as an important cause of persistent diarrhoea in transplant recipients.1,2 While its gastro-intestinal manifestations are well described, its potential to precipitate acute allograft dysfunction remains less clearly emphasized in clinical practice.
The most likely mechanism of renal impairment in our patient was pre-renal acute kidney injury secondary to volume depletion, rapidly reversed with hydration. 3 The delayed rise in serum creatinine relative to the onset of diarrhoea suggests a cumulative haemodynamic insult rather than primary graft injury, supporting a reversible pre-renal mechanism.
In addition, diarrhoea may influence the pharmacokinetics of immunosuppressive agents, particularly calcineurin inhibitors, potentially contributing to graft dysfunction. 4 Although tacrolimus levels remained within the therapeutic range in our case, this interaction remains clinically relevant.
A key learning point is that infection-associated diarrhoea should be viewed as a haemodynamic stressor capable of inducing reversible allograft dysfunction, rather than merely a gastro-intestinal complication. Similar observations have been reported previously, including prior reports highlighting the severity of cryptosporidiosis in immunocompromised hosts, including patients with systemic lupus erythematosus. 5
Conclusion
Cryptosporidiosis should be considered in renal transplant recipients presenting with diarrhoea and acute allograft dysfunction. Recognition of infection-induced reversible pre-renal allograft dysfunction is critical in transplant nephrology, as timely correction of reversible factors can restore graft function and prevent unnecessary escalation of immuno-suppression.
Footnotes
Patient consent
Written informed consent for publication was obtained from the patient.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.