
Abstract

Keywords
Introduction
Temporary central venous catheterisation is frequently used for haemodialysis, through which. infection (CRBSI) may cause a major complication, particularly with Staphylococcus aureus. 1 Septic pulmonary embolism (SPE) is an important but under-recognised consequence and typically manifests radiologically as bilateral peripheral nodules, wedge-shaped infiltrates and cavitary lesions. 2 Progression to hydropneumothorax from rupture of necrotising cavitating lesions is, however, uncommon. 3 This may be presumed to represent tuberculosis.
Case report
A 15-year old boy with underlying auto-immune kidney disease required haemodialysis initially via a temporary femoral venous catheter, and then, for prolonged use, through a right internal jugular venous catheter. He was receiving immuno-suppressive therapy prior to admission.
A fortnight after catheter placement, he developed high-grade fever and acute dyspnoea. His blood pressure was 140/90 mm Hg, and clinical examination revealed left side decreased breath sounds. Blood cultures grew Staphylococcus aureus, which was also obtained from sputum. A computed tomography (CT) chest scan demonstrated multiple bilateral peripheral cavitating lesions with surrounding nodular opacities. Several lesions showed air–fluid levels, suggesting necrotising infection. Multiple wedge-shaped peripheral consolidations suggestive of septic pulmonary emboli were also identified. 2 A left-sided partial hydropneumothorax was present 3 (Figure 1). The central venous catheter tip was correctly positioned within the superior vena cava.
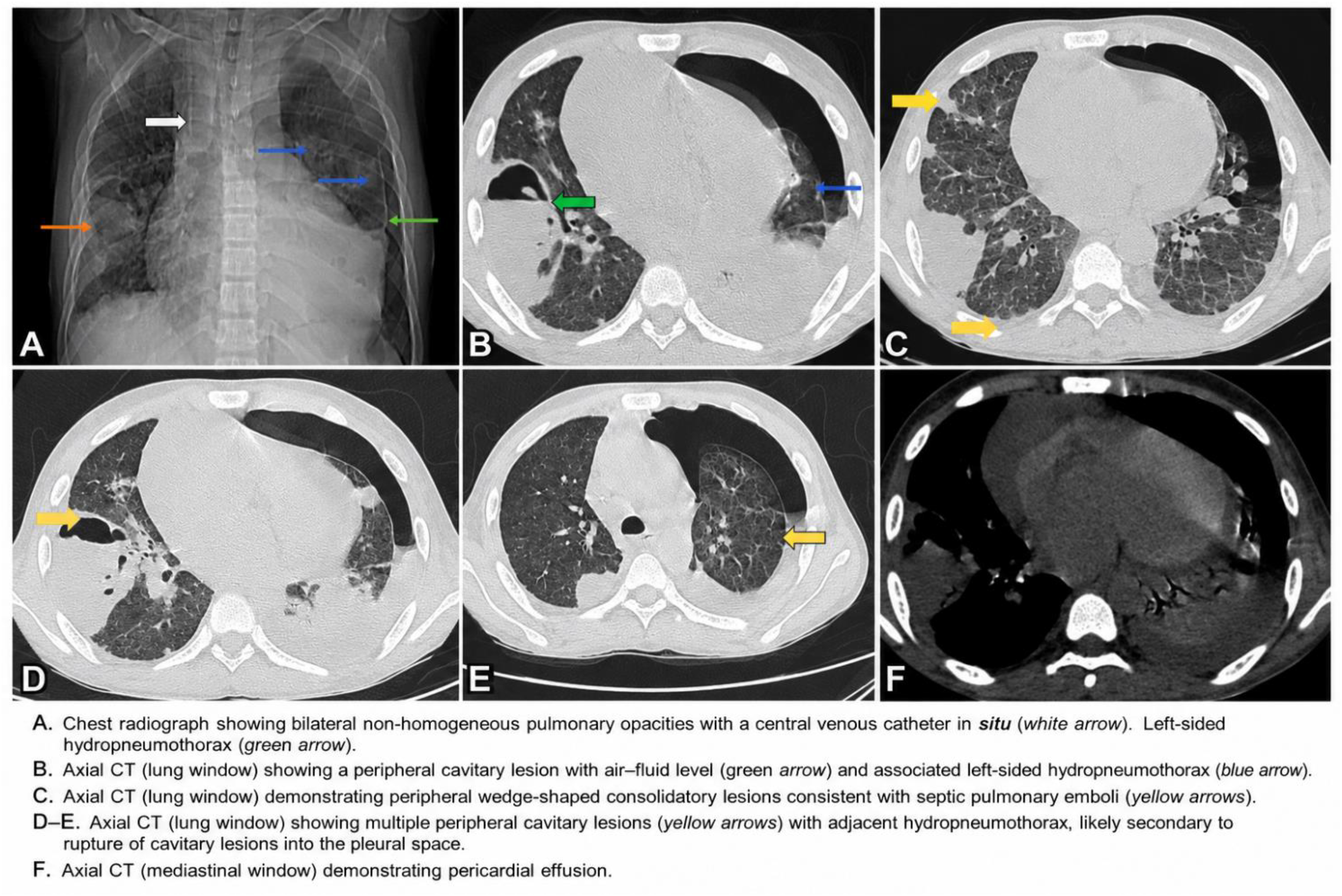
CT chest demonstrating multiple bilateral peripheral cavitary lesions with air–fluid levels (black arrows), wedge-shaped peripheral consolidation consistent with septic pulmonary emboli, and left-sided hydropneumothorax with passive lung collapse.
The acute presentation, peripheral embolic distribution on imaging, and concomitant isolation of Staphylococcus aureus from blood and sputum strongly supported SPE secondary to catheter-related bloodstream infection. 1
The catheter was thus removed and intravenous vancomycin was initiated as targeted therapy whilst continued renal replacement therapy was continued, though immuno-suppressive therapy was temporarily withheld, with good effect.
Discussion
Catheter-related bloodstream infection is a major cause of morbidity among haemodialysis patients. 4 Staphylococcus aureus remains the predominant pathogen and is strongly associated with metastatic infectious complications.1,5
SPE is not an infrequent complication, but hydropneumothorax is uncommon, arising from rupture of necrotising cavitating lesions into the pleural space. 3 Recognition of this complication is important because its delayed diagnosis may result in respiratory deterioration and increased mortality.
In tropical countries, cavitary lung lesions are frequently attributed to tuberculosis, but the clinical situation must be taken into consideration, and blood and sputum cultures rigourously pursued. However, the presence of intravascular devices, bacteraemia and peripheral embolic distribution of lesions should prompt consideration of SPE. Early imaging, prompt catheter removal and targeted antimicrobial therapy are critical for favourable outcomes, particularly among immuno-compromised patients.
Footnotes
Ethics approval
Not applicable.
Consent for publication
Written informed consent for publication of this case report and accompanying images was obtained from the patient.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Availability of data and materials
Not applicable.