
Abstract
Iatrogenic oesophageal perforation (IOP) is a rare but potentially fatal complication of orogastric (OG) or nasogastric tube insertion in preterm neonates, with mortality rates up to 30%. We describe the case of a female neonate born at 31 + 5 weeks of gestation (birth weight 1.8 kg) who required extensive resuscitation and OG tube insertion after admission to the neonatal intensive care unit. Admission chest radiograph showed right-sided pneumothorax with OG tube aberrantly positioned in the right hemithorax which was missed initially. Following intercostal drain insertion and commencement of enteral feeds, milky pleural drainage was observed. Normal pleural triglyceride levels excluded chylothorax, prompting radiographic re-evaluation and paediatric surgical review, leading to diagnosis of IOP. Despite conservative management, the infant developed septic shock with sclerema and died on the 4th day of life. This case emphasises careful radiographic confirmation of tube placement in preterm neonates and the diagnostic significance of milky pleural drainage following feeds
Introduction
Iatrogenic oesophageal perforation (IOP) in neonates, though rare, carries significant morbidity and mortality, particularly in preterm and very low birthweight infants whose oesophageal wall is thin and susceptible to injury from routine intensive care procedures.1,2 The most common cause is gastric tube insertion, followed by endotracheal intubation and pharyngeal suctioning.1,3 Perforation typically occurs at the pharyngo-oesophageal junction or right piriform sinus, and radiographic tube malposition within the right hemithorax is the pivotal diagnostic clue. 4 Despite this, diagnosis is frequently delayed because pneumothorax, a common neonatal complication, tends to dominate the clinical picture, relegating tube position to secondary consideration. 5 Non-operative management has emerged as the preferred initial strategy for oesophageal perforation, with comparable outcomes to surgical repair in stable neonates.3,6 We report a case of suspected IOP in which delayed recognition of tube malposition, followed by the appearance of milky pleural drainage, prompted the diagnosis.
Case report
A female neonate, delivered at 31 weeks’ and 5 days’ gestation with a birth weight of 1.8 kg, required extensive resuscitation including endotracheal intubation. She was admitted to the neonatal intensive care unit and had an orogastric (OG) tube inserted following initial stabilisation. A subsequent chest radiograph demonstrated a right-sided pneumothorax with the OG tube visible in the right hemithorax (Figure 1). However, this malposition was at first not recognised, the clinical focus being on treatment of the pneumothorax. An intercostal drain (ICD) was inserted, but as the infant was then haemodynamically stable, no further intervention was deemed necessary.
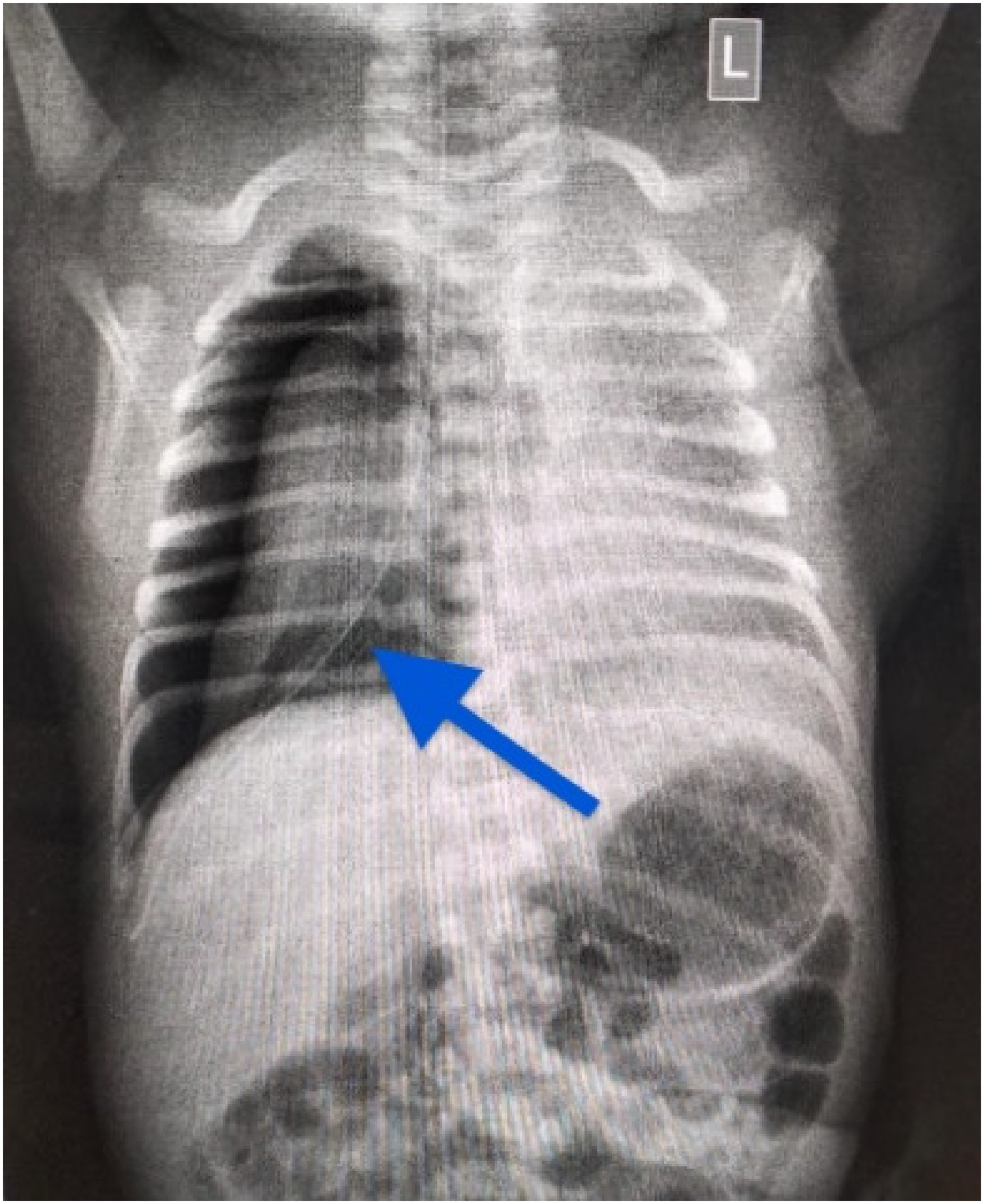
Chest radiograph showing right-sided pneumothorax with a malpositioned orogastric tube entering the right hemithorax (arrow).
Subsequently, however, milky fluid was observed draining from the ICD after starting feeds (Figure 2). A chylothorax was excluded by pleural fluid analysis showing normal triglyceride levels. Thus the chest radiograph was re-examined, which demonstrated the OG tube was not located within the stomach.
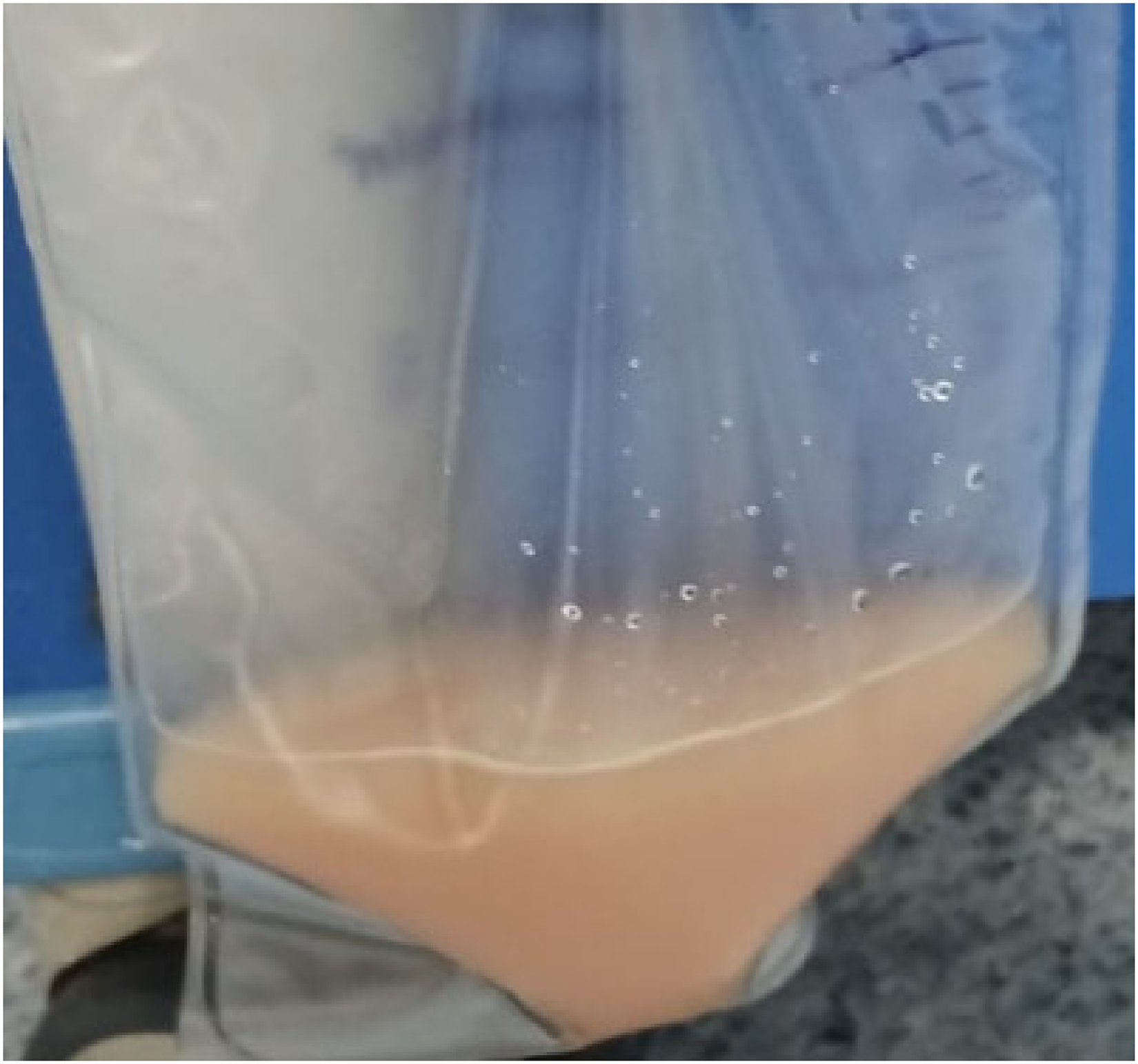
Milky pleural fluid in ICD bag. ICD: intercostal drain.
Conservative management for an evident oesophageal perforation was instituted, restricting oral intake, and treatment with a barrage of intravenous broad-spectrum antibiotics (piperacillin-tazobactam, amikacin, meropenem, vancomycin, colistin and teicoplanin). Despite this, the neonate developed septic shock with generalised sclerema and died on her fourth day of life.
Discussion
This case illustrates the two cardinal diagnostic features of IOP in preterm neonates: radiographic tube malposition and milky pleural drainage following enteral feeds. IOP most commonly arises at the pharyngo-oesophageal junction.1,4 It may be misdiagnosed as oesophageal atresia or an unrelated pneumothorax, and careful radiographic review of tube position is obligatory. 1
Barotrauma could have been a plausible alternative cause of pneumothorax. However, the combination of radiographic OG tube malposition in the right hemithorax and subsequent enteral feed-associated pleural drainage proved otherwise. Confirmatory investigations such as water-soluble contrast oesophagography, CT with contrast, flexible endoscopy, or postmortem histology were not performed. In resource-limited settings, clinicians often need to rely on clinical probability rather than formal confirmatory investigations. 7
A chylothorax has an elevated pleural triglyceride concentration (typically >1.1 g/L).5,8
Non-operative management is now the established first-line approach in stable neonates.3,4,9,10 In our case, delayed recognition allowed soiling of the right pleural cavity, which, though no microbiological evidence nor postmortem confirmation could be produced, is a major predictor of adverse outcomes. 6
In conclusion, first, every post-OG insertion neonatal radiograph must include a systematic checklist review before clinical action is taken. Second, the combination of an OG tube in the right hemithorax with ipsilateral pneumothorax should be treated as an IOP until proven otherwise. Third, in resource-limited settings where contrast oesophagography is not immediately feasible, the combination of tube malposition, ipsilateral pneumothorax and feed-associated pleural drainage should declare an oesophageal perforation unless proved otherwise and prompt surgical intervention unless deemed unsurvivable. Fourth, the decision to operate should be guided by clinical trajectory rather than fixed anatomical criteria. 11 Accepted indications for surgery in neonatal IOP include: (i) failure of the pleural effusion or pneumothorax to resolve or worsening on serial radiographs despite bowel rest and antibiotic therapy; (ii) ongoing or increasing ICD output without clinical improvement; (iii) development of empyema mediastinitis; (iv) progression to septic shock, haemodynamic instability, or multi-organ dysfunction refractory to medical management; and (v) failure to demonstrate clinical improvement despite appropriate conservative management. 7 Thus, close monitoring is essential to identify these signs. Operative options include primary repair of the oesophageal defect, debridement, drainage of contaminated pleural or mediastinal collections, and in complex cases, oesophageal exclusion with staged reconstruction. These are all formidable procedures: thus, best avoided in the first place by immediate correction if OG tube placing is in some way unsatisfactory.
Footnotes
Acknowledgements
The authors we would acknowledge the contribution of the nursing staff and residents of the neonatal unit for their assistance in patient care and data retrieval.
Ethics approval and consent to participate
All necessary consent and approval were obtained by the authors. Further, this case report has been prepared in accordance with the CARE (CAse REport) guidelines. All necessary consent and approval were obtained by the authors. Further, this case report has been prepared in accordance with the CARE (CAse REport) guidelines.
Consent for publication
All necessary consent for publication was obtained by the authors.
Author contributions
All authors contributed significantly to this manuscript. All authors contributed significantly to this manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All data generated and analysed are included within this research article. All data generated and analysed are included within this research article.