
Abstract
Per-anal minimally invasive surgery (traditionally known as TAMIS) is an effective technique for local excision of selected rectal lesions. However, widespread adoption in low-resource countries remains constrained by the high cost of dedicated TAMIS access platforms, which cost c. US$700. This cost barrier is particularly relevant in publicly funded hospitals serving economically disadvantaged populations. We report the development and successful clinical use of an indigenous low-cost TAMIS port fabricated from commonly available materials at a total cost of only US$5.
Case report
An 80-year old woman presented with a broad-based polypoidal lesion located on the right lateral wall of the lower rectum, c. 3 cm above the dentate line. Biopsy showed an adenomatous polyp with dysplasia. Magnetic Resonance imaging showed a lesion confined to the mucosa without evidence of sub-mucosal invasion. Radical resection was considered undesirable because of the patient's advanced age, associated operative risk, and her refusal to accept a temporary stoma.
To facilitate local excision, an indigenous TAMIS port was designed by surgical residents (authors KH & UG). Approval was obtained from our institutional ethics committee (IEC/2026/5846). The device was constructed using a stainless steel ‘tiffin box’ (diameter 10 cm, cost US$ 1.50). Three instrument ports, one 10-mm optical port and two 5-mm working ports, were created on the base. An additional side-wall port was made for suction. Standard laparoscopic rubber washers (cost US 50c) were used as seals to minimise gas leakage. A truncated conical stainless steel glass (base 5 cm, top 3.5 cm, length 8 cm) was welded to the lid. Its outer surface was covered with rubber derived from a bicycle inner tube (cost = US 80c) to improve grip and reduce mucosal trauma (Figure 1), (total fabrication cost coming to US$ 2). Sterilisation was achieved with ethylene oxide. Written informed consent was obtained from our patient.
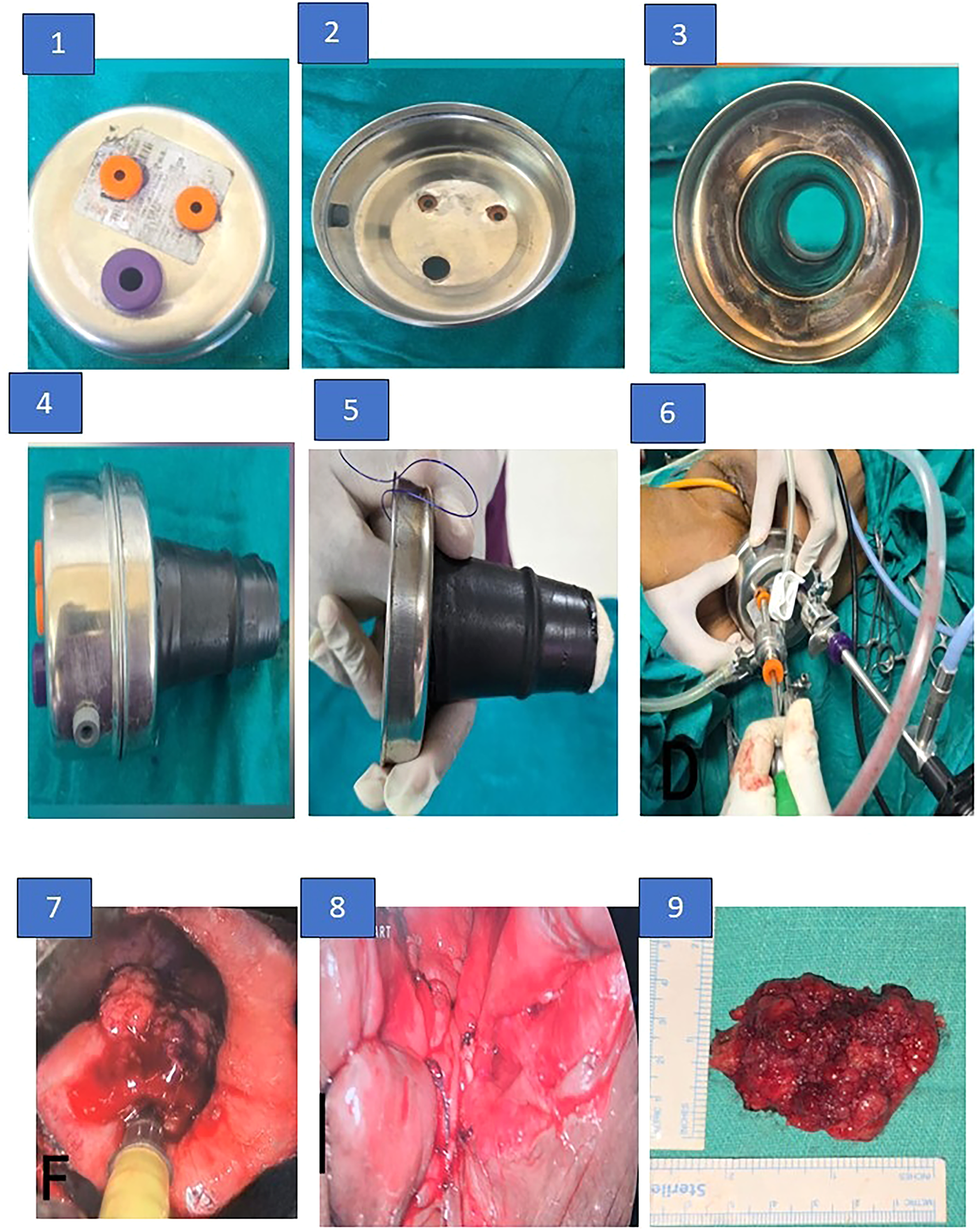
Indigenous per-anal minimally invasive surgery (TAMIS). 1. Base of tiffin box with one 10 mm and two 5 mm ports. 2. Inner view of tiffin box. 3. Lid of tiffin box with conical stainless steel glass welded over it. 4. Side port for suction. 5. Obturator made of lignocaine jelly soaked gauze. 6. Complete assembled device with telescope and operating instruments. 7. Lesion endoscopically visualised. 8. Tumour bed after closing the defect. 9. Excised specimen.
Under general anaesthesia, she was placed in the lithotomy position with Trendelenburg tilt. A lubricated gauze with long stay sutures (kept outside the anus for later retrieval) was used as an obturator while introducing the glass part of the port per-anally. This was then pushed proximally to prevent colonic faecal matter from contaminating the operative field and to ensure a stable pneumo-rectum, which was then established using standard carbon dioxide insufflation. Conventional laparoscopic instruments were used.
After circumferential marking with monopolar electrocautery, full-thickness excision was performed using a harmonic scalpel with a 5-mm surgical margin until mesorectal fat was visible. The rectal defect was subsequently closed with interrupted 3–0 polyglactin sutures (Figure 1).
The procedure was completed successfully without any complications. Visualisation, instrument triangulation, and maintenance of pneumo-rectum were satisfactory throughout the operation. The postoperative course was uneventful, and our patient was discharged without any adverse events. Final histopathology confirmed a tubular adenoma with high-grade dysplasia with clear resection margins.
Discussion
Innovation in surgery is often viewed through the lens of advanced technology. However, in resource-constrained environments, innovation needs to be driven by necessity; the greatest gains arise from using simple materials and adapting these for functional surgical solutions. Our device reduced procedural access costs by >99% compared with commercially available systems, while still allowing the use of standard laparoscopic instruments already available. Another advantage is that our product is re-usable while commercially available ports are manufactured for single use; furthermore, its outer box acts as a reservoir for any rectal effluent which can readily be removed from the suction port at its side-wall.
Our proof-of-concept experience demonstrates the feasibility of a safe, effective and extremely low-cost alternative to commercial TAMIS platforms. Obviously, further evaluation in larger series is warranted, but it goes without saying that frugal innovations such as ours will achieve accessibility of TAMIS in settings where otherwise cost would be a prohibitive barrier to care.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Declaration of Artificial Intelligence (AI) in scientific writing
During the preparation of this manuscript, the authors used artificial intelligence tools for language refinement, grammar correction, and improvement of readability. The authors carefully reviewed and edited the output and take full responsibility for the content of the manuscript.