
Abstract
Keywords
Introduction
Antineutrophil cytoplasmic antibody (ANCA)-associated vasculitis is a potentially life-threatening small-vessel vasculitis characterised by necrotising inflammation involving multiple organ systems, particularly the kidneys and respiratory tract.1,2 Early manifestations are often non-specific and may include constitutional symptoms, anaemia, and subtle urinary abnormalities before the development of overt organ-threatening disease. Persistent microscopic haematuria may represent the earliest clue to glomerular inflammation and may precede deterioration in renal function by several weeks. 3 Failure to recognise these early findings may delay diagnosis and curative immuno-suppressive therapy, allowing progression to rapidly progressive glomerulonephritis and diffuse alveolar haemorrhage.
Case report
A 45-year old woman with no previous history of diabetes mellitus, hypertension, chronic kidney disease, nor auto-immune disease initially presented with progressive generalised weakness, easy fatiguability, and bilateral pedal oedema. At multiple consultations over the preceding months, she was evaluated for symptomatic anaemia and received packed red blood cell transfusions. Her illness was attributed to iron deficiency and vitamin B12 deficiency anaemia.
Retrospective review of her previous investigations showed persistent microscopic haematuria despite preserved renal function with normal serum creatinine levels. No nephrological or auto-immune evaluation was pursued at that stage.
Over the following weeks, she developed progressive oliguria that developed into complete anuria for 6 days prior to admission to us. On presentation, her blood pressure was 140/90 mmHg, with extensive palpable purpuric and violaceous lesions involving both lower limbs with areas of necrotic discolouration, suggestive of active cutaneous vasculitis (Fig. 1). Laboratory tests demonstrated severe acute kidney injury with a serum creatinine of 1.06 mmol/L.

Extensive palpable purpuric and violaceous vasculitic lesions with areas of necrotic discolouration involving both lower limbs, consistent with active small-vessel vasculitis.
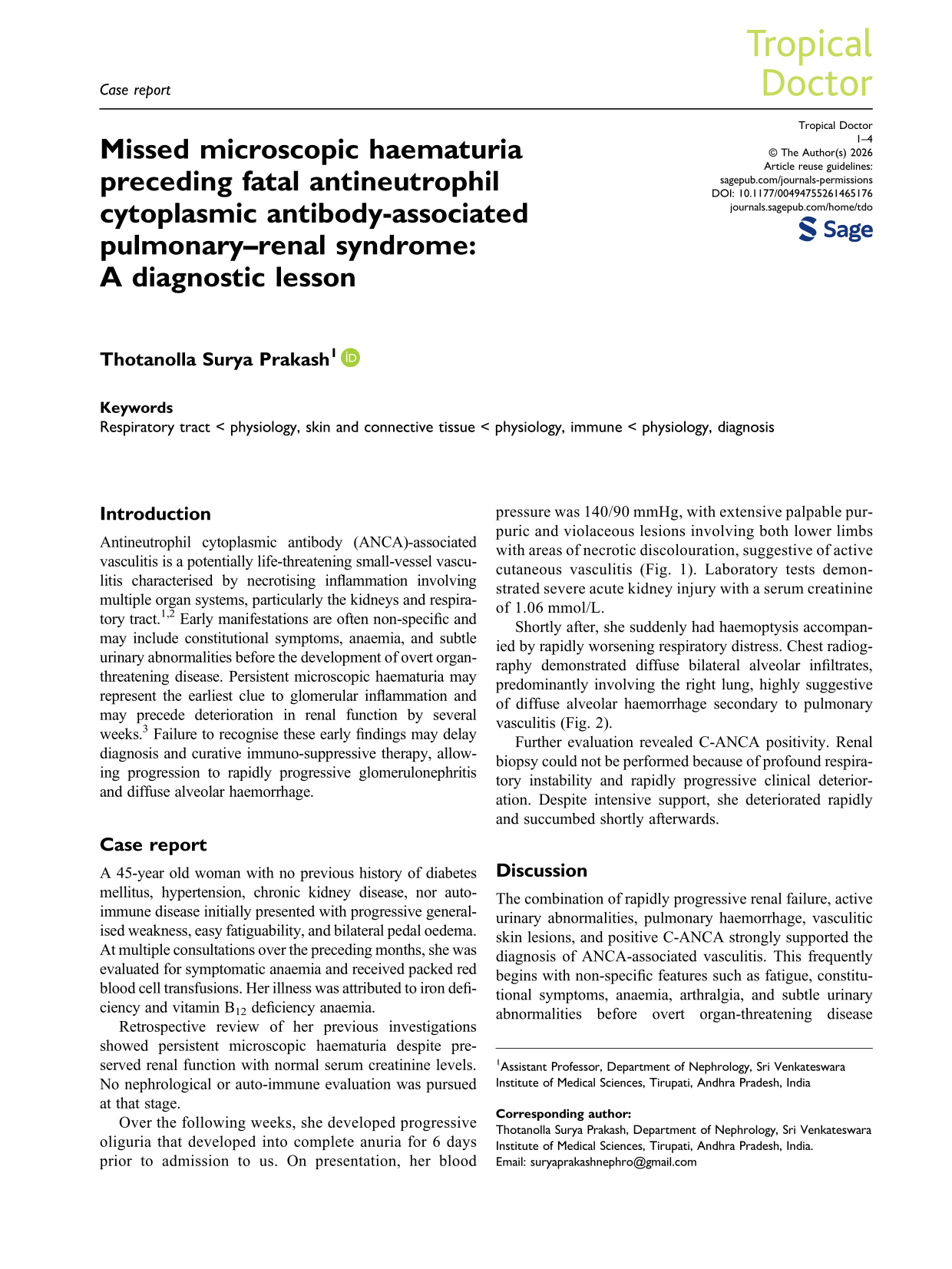
Shortly after, she suddenly had haemoptysis accompanied by rapidly worsening respiratory distress. Chest radiography demonstrated diffuse bilateral alveolar infiltrates, predominantly involving the right lung, highly suggestive of diffuse alveolar haemorrhage secondary to pulmonary vasculitis (Fig. 2).
Chest radiograph demonstrating diffuse bilateral alveolar infiltrates suggestive of diffuse alveolar haemorrhage secondary to pulmonary capillaritis.
Further evaluation revealed C-ANCA positivity. Renal biopsy could not be performed because of profound respiratory instability and rapidly progressive clinical deterioration. Despite intensive support, she deteriorated rapidly and succumbed shortly afterwards.
Discussion
The combination of rapidly progressive renal failure, active urinary abnormalities, pulmonary haemorrhage, vasculitic skin lesions, and positive C-ANCA strongly supported the diagnosis of ANCA-associated vasculitis. This frequently begins with non-specific features such as fatigue, constitutional symptoms, anaemia, arthralgia, and subtle urinary abnormalities before overt organ-threatening disease develops.1,2 Renal involvement commonly manifests initially as microscopic haematuria and may precede significant deterioration in renal function. 3 Consequently, urinalysis may provide one of the earliest objective clues to evolving glomerular inflammation, before fulminating pulmonary and renal collapse.
Our case illustrates a missed diagnostic opportunity. Persistent microscopic haematuria, constitutional symptoms, oedema, and anaemia were all present for several weeks before the development of catastrophe. A normal serum creatinine during the early phase of illness probably contributed to failure to recognise active glomerular disease. As a result, our patient was allowed to progress from a potentially treatable inflammatory condition to rapidly progressive renal failure and fatal diffuse alveolar haemorrhage.
This latter is among the most severe complications of ANCA-associated vasculitis and is associated with substantial mortality. 4 Pulmonary capillary inflammation results in diffuse disruption of the alveolar microvasculature, leading to haemoptysis, hypoxaemia, and respiratory failure. The co-existence of diffuse alveolar haemorrhage and rapidly progressive glomerulonephritis is described as pulmonary–renal syndrome, a medical emergency requiring urgent diagnosis and prompt immuno-suppressive therapy.
The principal educational message of this case is the importance of recognising persistent microscopic haematuria as a marker of possible systemic vasculitis, even when renal function remains normal. In many resource-constrained settings, access to advanced serological testing may be limited; however, urinalysis remains inexpensive, widely available, and easily performed. Careful interpretation of persistent urinary abnormalities may facilitate earlier referral, auto-immune evaluation, and treatment before irreversible organ damage develops.
Footnotes
Acknowledgements
The authors would like to thank the patient and her family for consenting to the publication of this case and the accompanying clinical images
Ethics approval
Ethics approval was not required for this case report in accordance with institutional policy.
Consent for publication
Written informed consent for publication of this case report and the accompanying clinical images was obtained from the patient and is available for review by the Editor upon request.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
Not applicable.