
Abstract
Introduction
Myiasis is the infestation of living tissues by dipterous fly larvae and can affect both humans and animals. Ocular involvement is relatively uncommon and accounts for only a small proportion of all human myiasis cases. Depending on the depth of larval penetration, ophthalmomyiasis is classified as external, internal, or orbital, with external ophthalmomyiasis being the most common form. Among the various species implicated in ocular infestation, Oestrus ovis is recognised as the principal causative agent worldwide. The parasite normally completes its life cycle in sheep and goats; however, humans may become accidental hosts following the deposition of first-stage larvae onto the ocular surface. Although the condition has traditionally been associated with livestock breeding and rural environments, recent reports indicate that infestation may also occur in individuals without direct animal contact.1,3
The clinical manifestations of external ophthalmomyiasis are often nonspecific and may resemble common forms of conjunctivitis. Ocular redness, irritation, tearing, discharge, and foreign body sensation are the most frequently reported symptoms. Therefore, the diagnosis may be missed unless the conjunctival surfaces and fornices are carefully examined.1,4
Over the past two decades, numerous cases of O. ovis ophthalmomyiasis have been reported from various regions of Turkey, particularly in areas where sheep and goat farming is prevalent.3–5
Case reports
Case 1
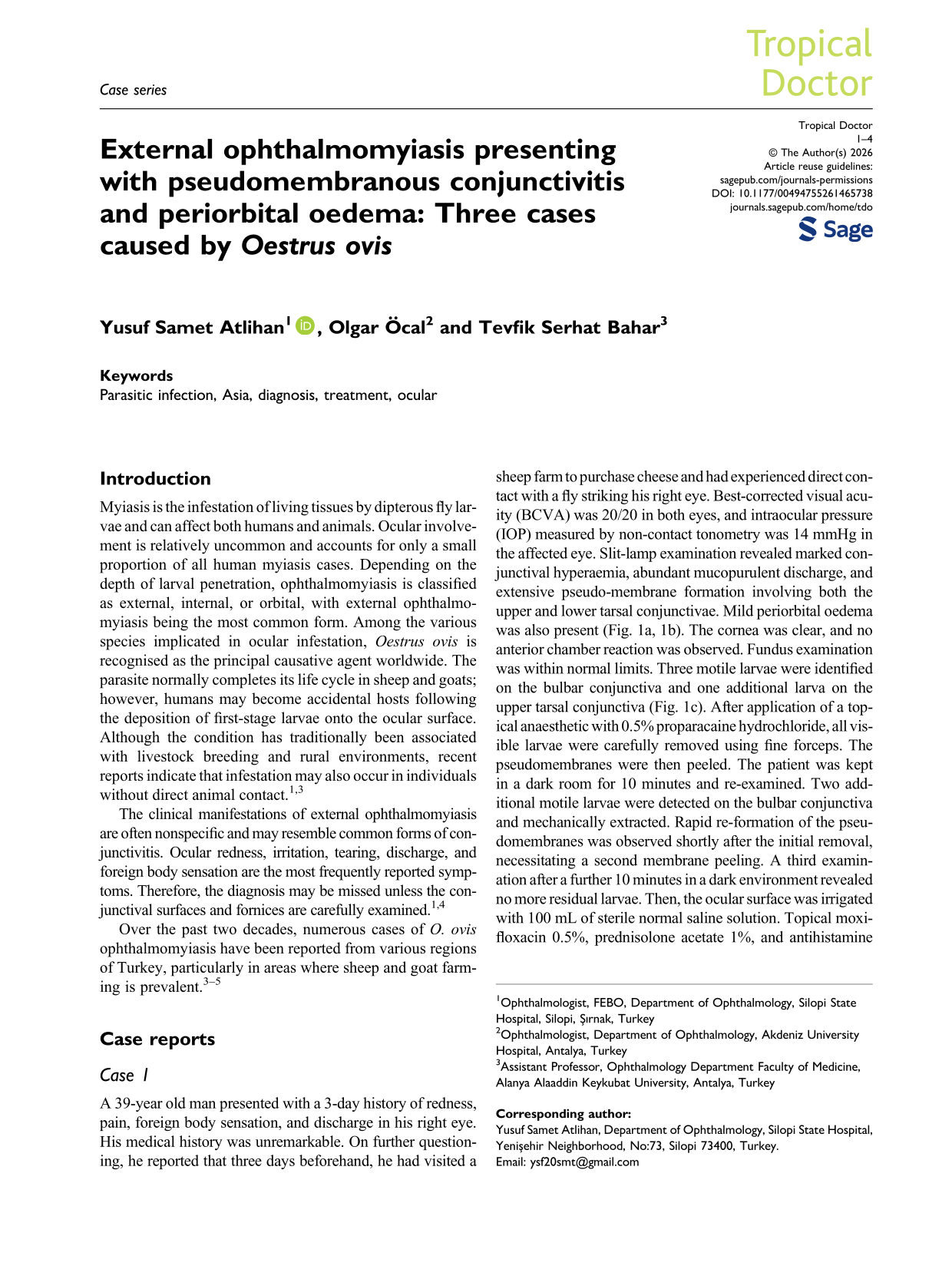
A 39-year old man presented with a 3-day history of redness, pain, foreign body sensation, and discharge in his right eye. His medical history was unremarkable. On further questioning, he reported that three days beforehand, he had visited a sheep farm to purchase cheese and had experienced direct contact with a fly striking his right eye. Best-corrected visual acuity (BCVA) was 20/20 in both eyes, and intraocular pressure (IOP) measured by non-contact tonometry was 14 mmHg in the affected eye. Slit-lamp examination revealed marked conjunctival hyperaemia, abundant mucopurulent discharge, and extensive pseudo-membrane formation involving both the upper and lower tarsal conjunctivae. Mild periorbital oedema was also present (Fig. 1a, 1b). The cornea was clear, and no anterior chamber reaction was observed. Fundus examination was within normal limits. Three motile larvae were identified on the bulbar conjunctiva and one additional larva on the upper tarsal conjunctiva (Fig. 1c). After application of a topical anaesthetic with 0.5% proparacaine hydrochloride, all visible larvae were carefully removed using fine forceps. The pseudomembranes were then peeled. The patient was kept in a dark room for 10 minutes and re-examined. Two additional motile larvae were detected on the bulbar conjunctiva and mechanically extracted. Rapid re-formation of the pseudomembranes was observed shortly after the initial removal, necessitating a second membrane peeling. A third examination after a further 10 minutes in a dark environment revealed no more residual larvae. Then, the ocular surface was irrigated with 100 mL of sterile normal saline solution. Topical moxifloxacin 0.5%, prednisolone acetate 1%, and antihistamine eye drops were prescribed. On the first-day follow-up, our patient reported marked symptomatic relief with substantial regression of conjunctival inflammation. One week later, conjunctival hyperaemia, discharge, and pseudomembrane formation had completely resolved, and no residual larvae were detected.

Clinical appearance of external ophthalmomyiasis due to Oestrus ovis. (a) Eyelid oedema and periocular erythema. (b) Diffuse conjunctival injection with mucopurulent secretion. (c) Slit-lamp image showing a first-stage Oestrus ovis larva attached to the bulbar conjunctiva (arrow).
Case 2
A 55-year old man presented with a one-day history of redness, pain, and foreign body sensation in his right eye. He had worked as a shepherd for many years and reported frequent occupational exposure to sheep and goats. He did not recall any direct contact with flies or ocular trauma before the onset of symptoms. BCVA was 20/20 in both eyes, and IOP measured by non-contact tonometry was 12 mmHg in the affected eye. Slit-lamp examination revealed conjunctival hyperaemia, mucopurulent discharge, and pseudomembrane formation involving both the upper and lower tarsal conjunctivae, although less extensive than in Case 1. Mild periorbital oedema was also noted (Fig. 2a). The cornea was clear, and there was no anterior chamber reaction. Fundus examination was unremarkable. Two motile larvae were identified on the bulbar conjunctiva and one additional larva on the upper tarsal conjunctiva (Fig. 2b). All visible larvae were carefully removed using fine forceps. The pseudomembranes were peeled, and the patient was re-examined after remaining in a dark room for ten minutes. No additional larvae were detected. After complete larval extraction, the ocular surface was irrigated with 100 mL of sterile normal saline solution. This patient was prescribed the same treatment regime as in Case 1. Follow-up examinations on the first day and first week demonstrated marked clinical improvement with complete resolution of symptoms and conjunctival findings. No residual larvae nor ocular complication was observed.

Clinical appearance of external ophthalmomyiasis due to Oestrus ovis. (a) Mild periorbital and eyelid oedema with conjunctival injection. (b) Slit-lamp image showing a first-stage Oestrus ovis larva attached to the bulbar conjunctiva (arrow).
Case 3
A 37-year old man presented with a two-day history of redness, pain, and foreign body sensation in his left eye. He lived in a rural village and reported that a fly had struck his eye while he was having a picnic the day before. He denied any history of livestock breeding or direct contact with sheep or goats. BCVA was 20/20 in both eyes, and IOP was 19 mmHg in the affected eye. Slit-lamp examination revealed conjunctival hyperaemia, mucopurulent discharge, and pseudomembrane formation involving both the upper and lower tarsal conjunctivae. Mild periorbital oedema was also observed. (Fig. 3a, 3b). The cornea was clear, and fundus examination was unremarkable. Three motile larvae were identified on the bulbar conjunctiva and were mechanically removed under topical anaesthesia (Fig. 3c). The pseudomembranes were peeled, and the ocular surface was irrigated with 100 mL of sterile normal saline solution. Re-examination after a 10-minute period in a dark room revealed no additional larvae. This patient was prescribed the same treatment regime as previous cases. Follow-up examinations demonstrated complete resolution of symptoms and conjunctival findings without complications.
Clinical appearance of external ophthalmomyiasis due to Oestrus ovis. (a) Mild periorbital oedema and diffuse conjunctival hyperaemia at presentation. (b) Eversion of the upper eyelid revealing pseudomembranous conjunctivitis of the tarsal conjunctiva (arrow). (c) Slit-lamp image showing a motile first-stage Oestrus ovis larva on the bulbar conjunctiva (arrow).
Laboratory evaluation
The extracted larvae were placed in physiological saline and sent for species identification. After routine laboratory preparation, including an alcohol series and xylene treatment, the specimens were examined under light microscopy. Morphological evaluation revealed translucent, spindle-shaped larvae measuring approximately 1–2 mm in length, with characteristic anterior oral hooks and segmental body spines. Based on these morphological features, the specimens were identified as first-instar O. ovis larvae (Fig. 4).

Light microscopy image of a first-instar Oestrus ovis larva. Characteristic anterior oral hooks and segmental body spines visible. Scale bar = 200 micrometer (μm).
Discussion
Ophthalmomyiasis externa is a rare ocular infestation caused primarily by first-stage larvae of O. ovis. As its clinical presentation often resembles acute conjunctivitis, diagnosis may be delayed unless a meticulous slit-lamp examination is performed. All three patients in our series presented with conjunctival hyperaemia, pain, foreign body sensation, mucopurulent discharge, pseudomembranous conjunctivitis, and periorbital oedema. Although conjunctival injection, tearing, and foreign body sensation are well-recognised manifestations of ophthalmomyiasis externa, the simultaneous occurrence of pseudomembranous conjunctivitis and periorbital oedema has received relatively little attention in the literature. While the former has occasionally been reported in association with O. ovis infestation, it is not generally emphasised as a characteristic clinical finding.3,6 The consistent presence of pseudomembranes in all three of our patients suggests that this manifestation may be underrecognised and may contribute to misdiagnosis as bacterial or viral conjunctivitis. Likewise, all patients in our series exhibited varying degrees of periorbital oedema. Previous reports have described eyelid swelling and inflammatory periocular reactions associated with ophthalmomyiasis externa.1,2 Particularly noteworthy is one case, in which external ophthalmomyiasis presented with marked eyelid oedema, chemosis, ocular motility restriction, and radiological findings mimicking orbital cellulitis despite the absence of intraocular or orbital invasion. 7 These findings were attributed to a severe local hypersensitivity reaction induced by O. ovis larvae. Similar inflammatory mechanisms may explain the periorbital oedema observed in our patients, although the severity was considerably milder.
Another notable observation was the rapid re-formation of pseudomembranes and the detection of additional larvae which became apparent when the patient remained in a dark room for several minutes. O. ovis larvae are highly photophobic and tend to migrate into the conjunctival fornices when exposed to light, hiding them from easy examination. Similar observations have been reported previously, emphasising the importance of eyelid eversion and careful inspection of the conjunctival fornices.3,8 Our findings further support the value of repeated slit-lamp examinations when clinical suspicion remains high despite apparently complete larval removal.
Complete removal of larvae is generally followed by rapid symptomatic improvement and excellent visual outcomes.3–5,9 Prominent pseudomembranous inflammation and periorbital oedema suggest a pronounced inflammatory response of the ocular surface and periocular tissues. Therefore, anti-inflammatory treatment may be particularly beneficial in such cases. with rapid symptomatic relief and regression of conjunctival inflammation following topical corticosteroid therapy. In addition, antihistamines may have a complementary role in patients with marked periocular oedema or suspected hypersensitivity reactions, as previously reported in severe inflammatory presentations of external ophthalmomyiasis.7,10 Although the combined use of topical corticosteroids, non-steroidal anti-inflammatory agents, and antihistamines may potentially accelerate recovery in selected patients with severe inflammatory responses, larger case series are required before firm therapeutic recommendations can be made.
Footnotes
Ethics statement
All procedures performed in this study were conducted in accordance with the ethical standards of the institutional and national research committees and with the principles of the Declaration of Helsinki and its subsequent amendments. Written informed consent was obtained from all patients for publication of their clinical data and accompanying images.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
None declared.