
Abstract
Leptospirosis exhibits a broad spectrum of clinical symptoms, ranging from mild fever to severe multiorgan failure. Hepatic dysfunction is common in leptospirosis and typically occurs after the prodromal phase of the disease. Jaundice in leptospirosis is due to impaired hepatocellular bilirubin excretion and bile flow disruption. However, bile duct injury leading to secondary sclerosing cholangitis (SSC) in leptospirosis is rare.
Case report
A 29-year old woman with no comorbidity presented with progressive jaundice for 45 days, intermittent fever, and 30 days of pruritus. These symptoms were not associated with pale stools nor significant weight loss. Examination revealed pallor and icterus, but systemic examination was unremarkable. Laboratory evaluation showed anaemia (Hb 96 g/L) with total bilirubin 165 µmol/L (direct bilirubin 121 µmol/L) and AST, ALT, and ALP 886/1271/72 IU/, respectively. Serological tests for viral hepatitis were negative. Workup for tropical infections, including typhoid, scrub typhus, and malaria, was also negative; however, IgM antibodies to leptospira were positive. Abdominal ultrasonography revealed mild hepatomegaly.
Intravenous ceftriaxone and oral doxycycline were administered for ten days. Initial serum bilirubin levels increased to 333 µmol/L (direct bilirubin 213µmol/L) and ALP increased to 280 IU/L, while transaminase levels normalised. Given the persistent cholestatic jaundice, further evaluation was mandated. An MRI scan revealed parenchymal fibrosis with multi-segmental narrowing of the intrahepatic bile duct radicles (Fig. 1A). A liver biopsy then showed confluent hepatocellular necrosis, portal-based inflammation, and bile duct injury (Fig. 1B). Based on the clinical course, imaging, and histopathological findings, secondary sclerosing cholangitis (SSC) secondary to leptospiral infection was diagnosed. With conservative management, gradual resolution of jaundice over three months occurred.
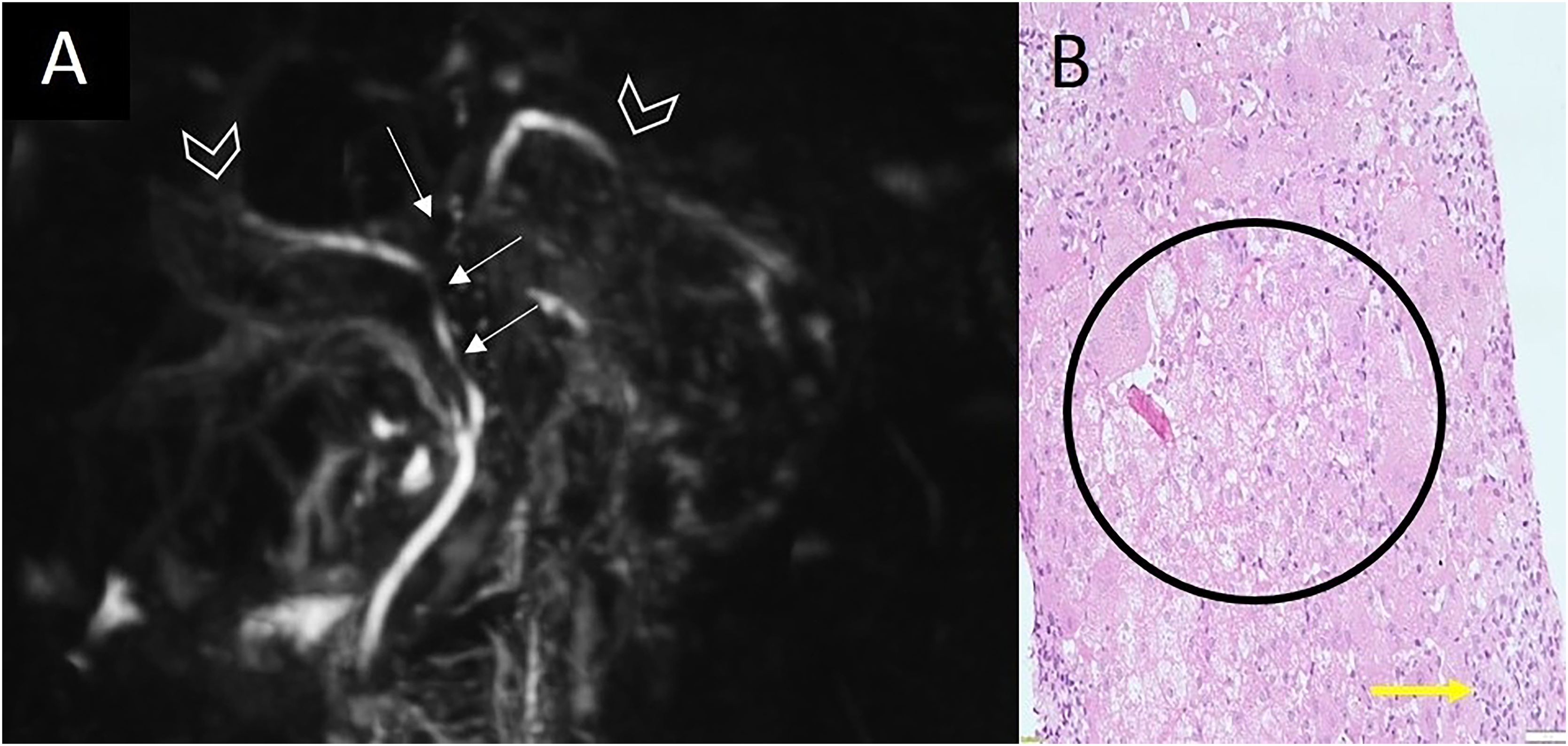
(A): Magnetic resonance cholangio-pancreatography image shows irregular narrowing at the confluence, left hepatic duct and common hepatic duct (arrows) with pruning of distal branch ducts (arrowheads), which are not visualised, suggestive of secondary sclerosing cholangitis. (B): Histopathological examination of the liver shows multiple foci of confluent necrosis (black circle) and loss of hepatic parenchyma, replaced by extensive ductular proliferation and a chronic inflammatory infiltrate (Yellow arrow).
Discussion
Leptospirosis is a global zoonosis with varied clinical signs ranging from mild fever to severe multi-organ failure. Hepatic dysfunction is common and usually presents with disproportionate hyperbilirubinaemia and modest increases in transaminase levels. It most frequently occurs approximately a week after the onset of prodromal symptoms. Unlike in viral hepatitis, jaundice in leptospirosis primarily reflects cholestasis due to impaired hepatocellular bilirubin excretion and dysfunction of intrahepatic bile flow, rather than extensive hepatocellular necrosis. The mechanisms involved include hepatocellular dysfunction, Kupffer cell activation, and disruption of bile canalicular transporters triggered by inflammatory mediators. 1
SSC is a progressive cholangiopathy caused by acquired damage to the biliary epithelium, resulting in inflammation, fibrosis, and multifocal stricture of the bile ducts. It is most commonly associated with critical illnesses, ischaemic cholangiopathy, recurrent pyogenic cholangitis, severe infections, and toxic insults. Infectious triggers include bacterial sepsis, opportunistic infections, and, rarely, parasitic or viral pathogens. SSC secondary to leptospirosis remains extremely rare, with only isolated case reports documented in the literature to date. Its pathogenesis is likely to be multifactorial. Proposed mechanisms include direct endothelial injury, small-vessel vasculitis, and ischaemic injury to cholangiocytes, which are vulnerable to hypoxia and inflammation. Immune-mediated bile duct injury during convalescence may contribute to progressive cholestasis despite microbiological clearance. 2 These mechanisms resemble those in SSC following severe infections, critical illness, or ischaemic cholangiopathy.3,4 The natural history of SSC is variable. It typically progresses to biliary cirrhosis and liver failure, particularly when associated with critical illness. However, it is reversible if the trigger is temporary and promptly managed, as demonstrated in our case.
This case highlights several clinically important issues. First, leptospirosis should remain a differential diagnosis for jaundice, particularly in endemic regions. Second, worsening cholestasis after initial treatment necessitates re-evaluation of the diagnosis and additional imaging. Third, bile duct injury and SSC, although rare, are possible complications of leptospiral infections. This should be considered in cases presenting with cholestatic jaundice when initial investigations are inconclusive. Early detection can prevent unnecessary invasive procedures and facilitate appropriate patient monitoring.
Footnotes
Authors’ contributions
LCK, KK, and VV were responsible for patient management and care; VV and LK contributed to original manuscript writing and conceptualisation; SG and SS contributed to supervision and review of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Statement and declarations
Informed written consent was obtained from the patient for the publication of this report.