
Abstract
Neonatal candidaemia is a significant cause of morbidity and mortality in neonatal intensive care settings, particularly in low- and middle-income countries where diagnostic delays remain a challenge.
The diagnostic utility of a five-parameter sepsis screen and the comparison of matrix-assisted laser desorption ionisation-time of flight mass spectrometry (MALDI-TOF MS) with VITEK-2 for identification of Candida species in neonates were evaluated at a tertiary care institute in the sub-Himalayan region of India from November 2022 to March 2024. Non-albicans Candida species accounted for 75% of isolates. Significant discordance was observed between MALDI-TOF MS and VITEK-2, particularly for cryptic species. The sepsis screen demonstrated a sensitivity of 77.8% but lacked specificity because it included only culture-positive fungal cases. The mortality rate was 30%. Thus, we conclude that a sepsis screen serves as a useful early screening tool but is non-specific. MALDI-TOF MS provides more accurate and faster species identification than biochemical methods. A combined diagnostic approach may help reduce delays in targeted therapy in neonatal candidemia.
Introduction
Invasive candidiasis has emerged as a formidable threat to neonatal survival, accounting for significant morbidity and mortality. 1 This vulnerability is rooted in the vulnerable physiological immaturity of the neonatal immune system, often exacerbated by life-saving but invasive clinical interventions such as central venous catheterisation, mechanical ventilation, and total parenteral nutrition. 2 While Candida albicans historically dominated systemic fungal infections, non-albicans Candida species, many of which exhibit inherent or acquired resistance to common azoles, have emerged in abundance. 3
In the sub-Himalayan region of Northern India, the diagnostic landscape is further complicated by a persistent ‘Diagnostic Gap’. 4 Traditional biochemical identification systems, such as VITEK-2, often struggle to differentiate accurately between closely related or ‘cryptic’ species, such as the C. parapsilosis complex 5 or emerging pathogens such as Pichia occidentalis. Such misclassifications may delay the initiation of targeted antifungal therapy,6,7 which is critical given that neonates often present with non-specific clinical signs.8,9 Our study addresses this gap by evaluating the synergy between rapid haematological sepsis screening and high-resolution matrix-assisted laser desorption ionisation-time of flight mass spectrometry (MALDI-TOF MS) speciation, establishing a vital regional benchmark for fungal sepsis management.
Material and methods
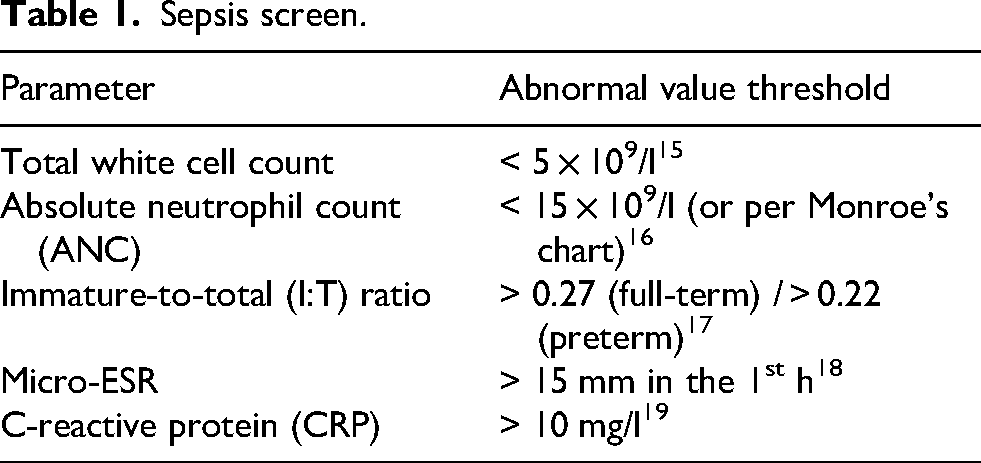
Our single-centre prospective cross-sectional study was conducted between November 2022 and March 2024 at a tertiary care Neonatal Intensive Care Unit in the sub-Himalayan region of Northern India. Only neonates with blood culture-proven candidaemia were included in the study. All Candida isolates were subjected to identification using the Bruker LT Microflex MALDI-TOF MS system. Results were compared with those obtained using the VITEK-2 Compact system. The former was used as the reference method, 10 given its greater discriminatory power for cryptic and emerging Candida species. 5 However, molecular sequencing was not performed. Primary phenotypic screening on Sabouraud's Dextrose Agar preceded a tiered identification protocol. 5 The Bruker LT Microflex MALDI-TOF MS system was used to process isolates using a formic acid/CHCA matrix extraction. 11 Scores were required for definitive species-level identification. 12 We compared results with the VITEK-2 compact system. 5 A standardised five-parameter sepsis screen was used to evaluate systemic inflammatory burden.13,14 Abnormal thresholds are given in Table 1.
Sepsis screen.
Results
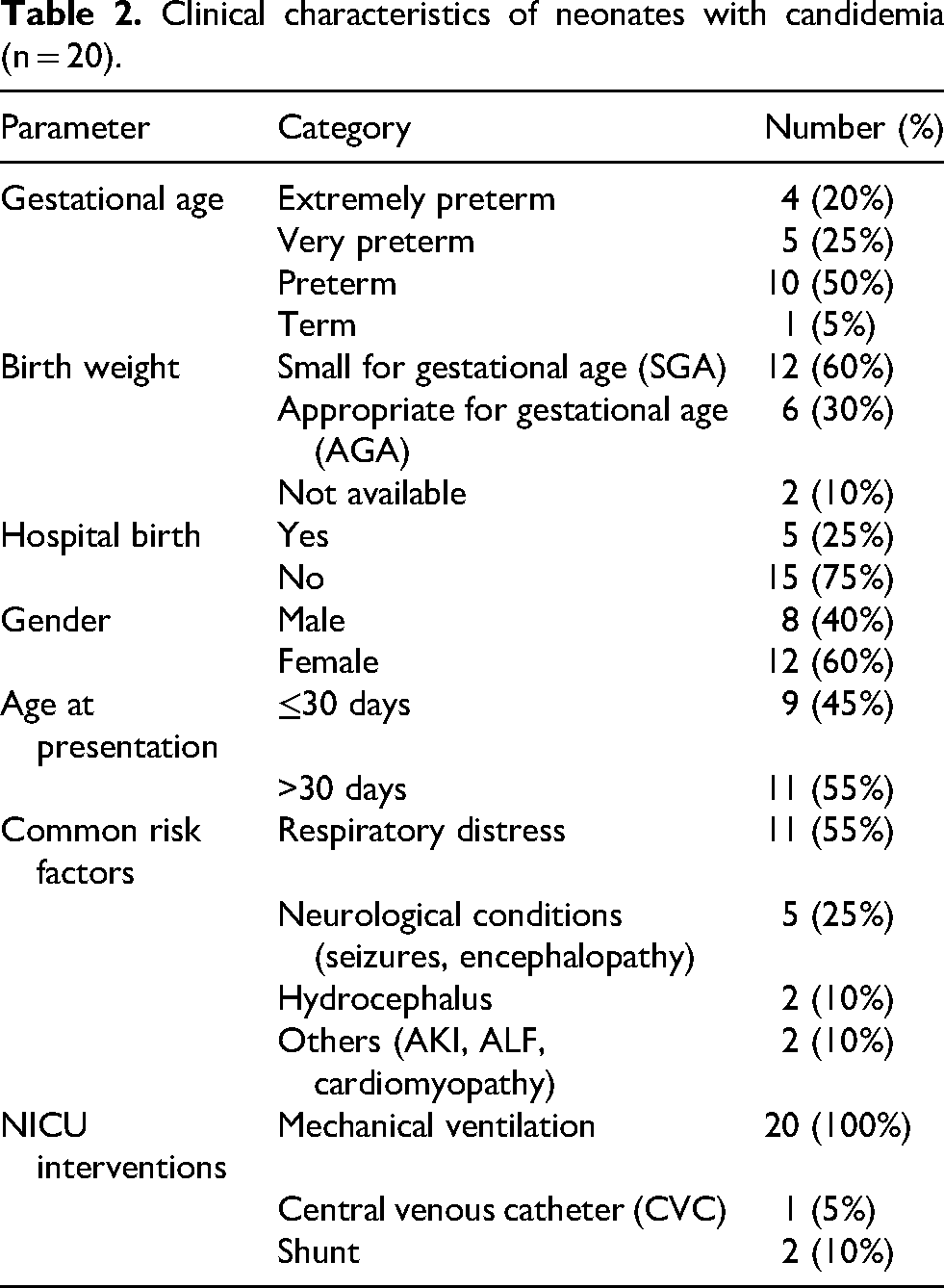
Neonatal candidaemia in this cohort predominantly affected a high-risk population, characterised by preterm birth (95%) and small for gestational age status (60%). Respiratory distress was the leading clinical presentation (55%). The majority of cases were born outside hospital (75%), and the universal requirement of mechanical ventilation highlights the severe clinical burden associated with these infections (Table 2).
Clinical characteristics of neonates with candidemia (n = 20).
A critical analysis of the 20 isolates revealed significant discordance between the proteomic and biochemical platforms. While common species such as C. tropicalis showed high concordance, biochemical methods consistently failed to identify cryptic pathogens. Clinically significant discordance (Tables 3 and 4).
Comparative analysis of neonatal Candida speciation (n = 20
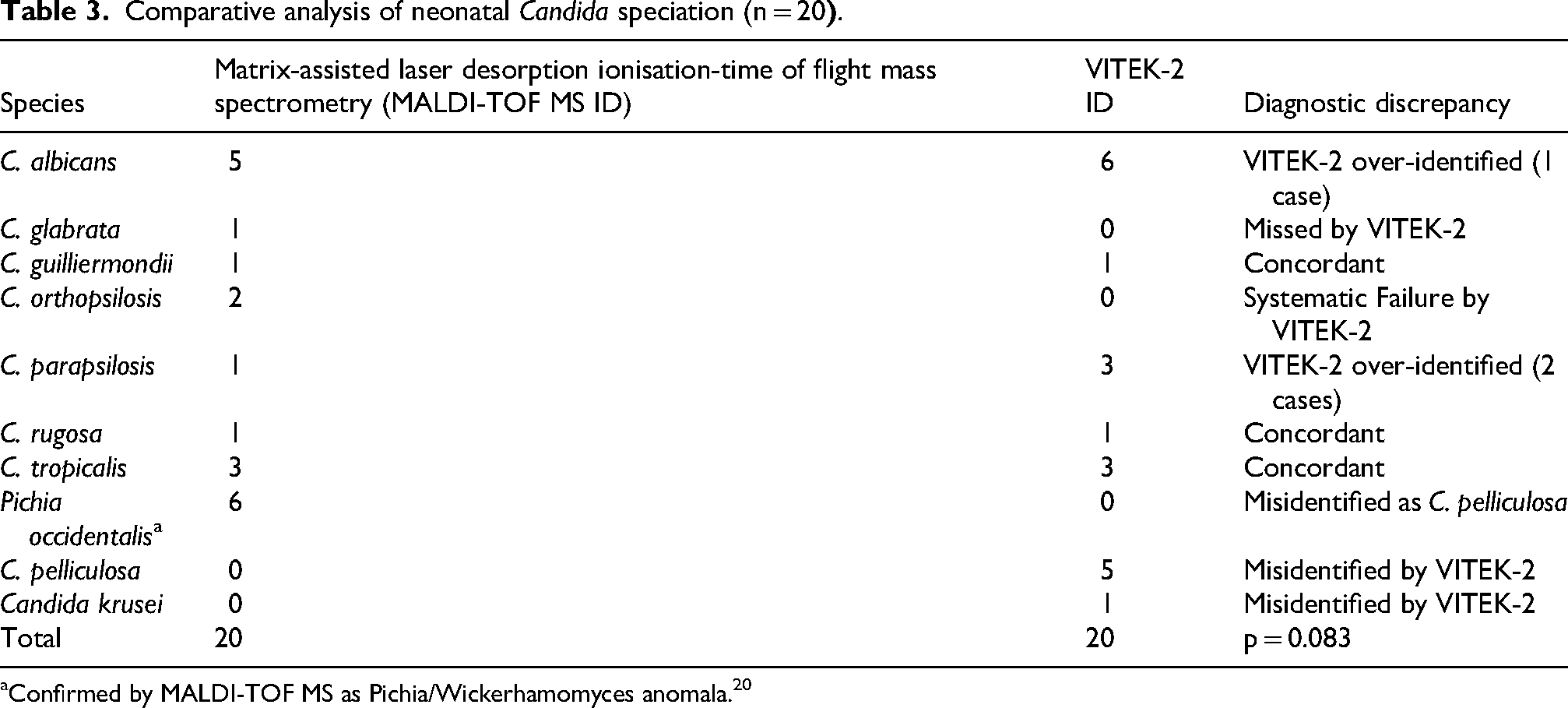
Confirmed by MALDI-TOF MS as Pichia/Wickerhamomyces anomala. 20
Diagnostic performance of the sepsis screen.
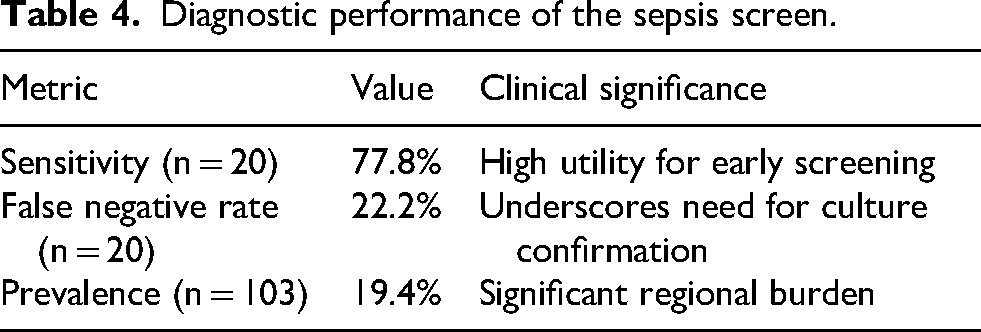
The ‘diagnostic gap’ was most evident in the misidentification of Pichia species as C. pelliculosa and the failure of VITEK-2 to distinguish C. orthopsilosis from the C. parapsilosis complex. MALDI-TOF MS scores provided definitive species-level identification where traditional phenotypic methods were insufficient (Table 4).
The sepsis screen demonstrated a sensitivity of 77.8% for detecting candidaemia. However, interpretation of diagnostic performance is limited by the study design, as only 20 culture-proven candidaemia cases were included. This underlines the need for simultaneous blood cultures and rapid MALDI-TOF MS speciation.
The term ‘prevalence’ in our study refers to the proportion of neonates with candidaemia among the 103 with suspected sepsis admitted to the NICU during the study period.
Specificity, positive predictive value (PPV) and negative predictive value (NPV) could not be calculated, as sepsis screen results in culture-negative and bacterial sepsis cases were not analysed. Our findings suggest that while the sepsis screen may serve as an early indicator, it cannot reliably distinguish fungal from bacterial sepsis.
Survival trajectories in the NICU showed significant variability (Table 5).
Neonatal clinical outcomes (n = 20).
The 30% in-hospital mortality rate, while severe, is lower than that of typical adult ICU cohorts, 21 possibly due to early intervention facilitated by the sepsis screen.
Discussion
Neonatal candidaemia remains a significant contributor to morbidity and mortality in NICU settings, particularly in low- and middle-income countries. 22 The 19.4% prevalence of candidaemia observed in this sub-Himalayan NICU underlines the substantial burden of fungal pathogens in Northern Indian tertiary care.23,24 The sepsis screen in our study showed a sensitivity of 77.8%, confirming its usefulness as an early screening tool. However, this finding must be interpreted cautiously. While sepsis screen parameters (such as CRP, ANC, and I: T ratio) are useful indicators of systemic inflammation, they are inherently non-specific and cannot distinguish between bacterial and fungal infections. 25 This limitation is particularly relevant in neonatal populations, where early-onset bacterial sepsis can present with similar haematological abnormalities. 8
In our setting, empirical antibacterial therapy remains the standard initial approach for suspected neonatal sepsis, but empirical antifungal therapy is considered selectively in high-risk neonates with persistent clinical deterioration or strong suspicion of fungal infection. In high-income settings, more restrictive antifungal use is guided by stringent clinical and microbiological criteria. 26
A high mortality rate of 30% in our study is comparable to reported rates. 27 Although neonates lack chronic comorbidity seen in adult populations, their immunological immaturity, coupled with exposure to invasive interventions, significantly increases their vulnerability. 27
A notable limitation of our study is that only culture-proven cases of candidaemia were included. As a result, the specificity, PPV, and NPV of the sepsis screen could not be determined. 28 Furthermore, molecular methods such as DNA 29 were not employed to validate species identification, which may have further strengthened the diagnostic conclusions.
However, overall, our findings reinforce the importance of integrating clinical assessment with rapid and accurate microbiological techniques.
Conclusion
Our study highlights that 75% of isolations of Non-Albicans Candida species in the sub-Himalayan neonatal population give a 30% mortality rate, 27 underlining the urgent need for a synergistic diagnostic approach. The 19.4% prevalence of candidaemia among suspected sepsis cases in our study underscores a high regional burden. While the rapid five-parameter sepsis screen is a useful early indicator with 77.8% sensitivity, its non-specific nature means it should not be the sole basis for initiating antifungal therapy. 13 Instead, it should trigger heightened clinical surveillance and a risk factor-based assessment. Empirical antifungal therapy should be reserved for high-risk neonates (e.g. those with persistent deterioration despite antibacterials) until MALDI-TOF MS provides definitive species identification. 30 This workflow is vital given the 35% discordance observed with biochemical systems such as VITEK-2, which frequently misidentify cryptic or emerging pathogens, such as Pichia occidentalis, potentially leading to suboptimal therapeutic outcomes. 31
Footnotes
Ethical clearance
The study was approved by the Institutional Ethics Committee
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.