
Abstract
A 43-year old man presented with fever and cough and was initially treated for community-acquired pneumonia. Within 24 h, he deteriorated and was admitted with type 1 respiratory failure. A recent history of exposure to waterlogged fields, along with progressive decline in haemoglobin, platelet counts and deranged liver function tests, raised suspicion for leptospirosis, later confirmed by positive IgM serology. With progressive clinical and radiological worsening, severe pulmonary haemorrhagic syndrome was considered. He was managed with oxygen, noninvasive ventilation (NIV), ceftriaxone, doxycycline, cotrimoxazole, and pulse methylprednisolone. He showed significant improvement and was successfully weaned off NIV and oxygen. This case highlights the importance of early recognition and timely initiation of steroid therapy in severe leptospiral pulmonary involvement.
Keywords
Case presentation
A 43-year old man presented with a 3-day history of cough and fever. At initial outpatient evaluation, a chest radiograph revealed left lower zone consolidation (Fig. 1A), and the CURB 65 score was 1. He was treated with amoxicillin–clavulanic acid and paracetamol. Baseline investigations showed mild anaemia (Hb 11.2 g/L), total leucocyte count 11.2 × 109/L, and platelet count 96.2 × 109/ L.
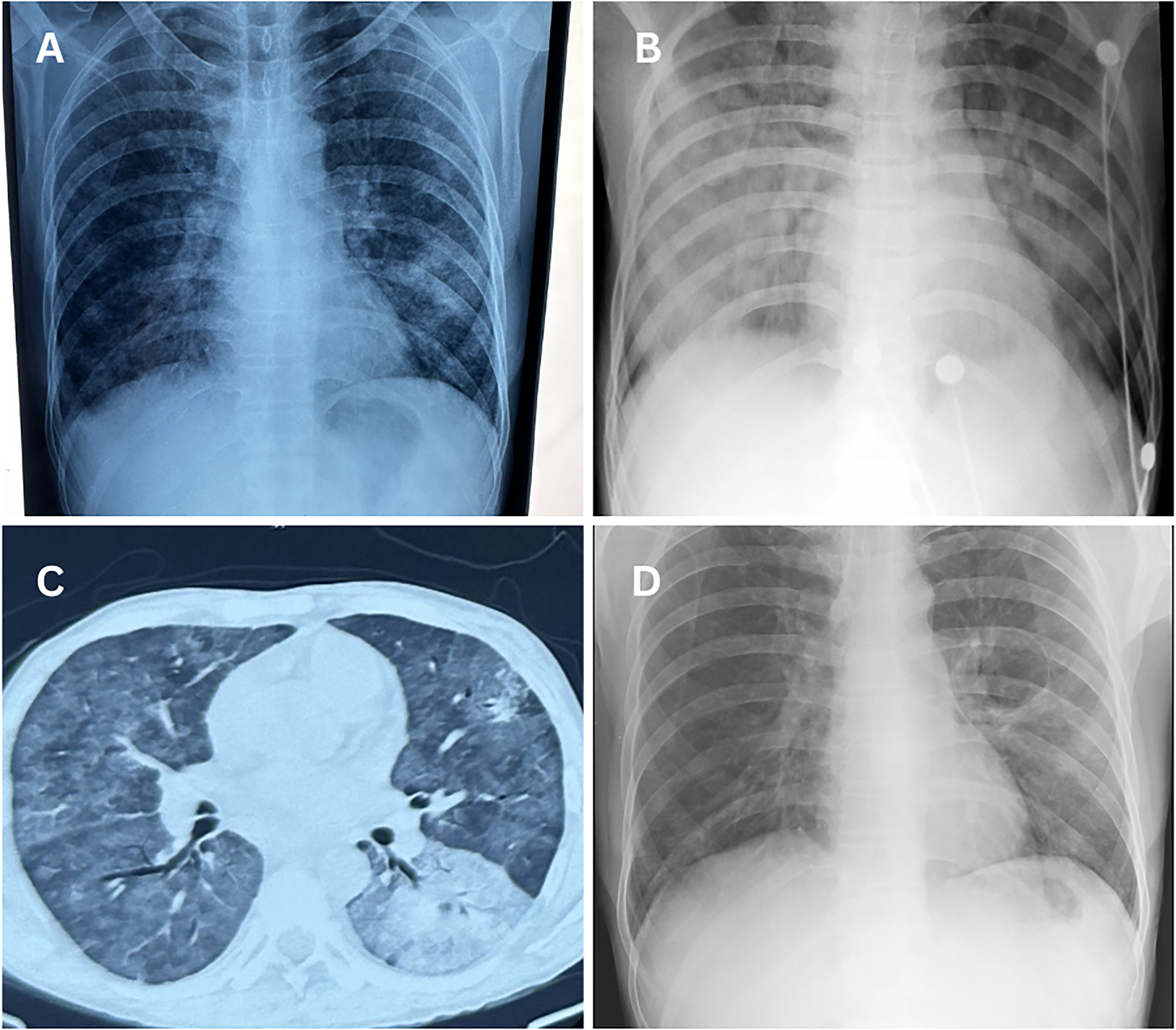
Radiological evolution of leptospirosis-associated pulmonary haemorrhage (A) initial chest radiograph showing left lower zone consolidation. (B) Chest radiograph obtained 24 h later demonstrating rapid progression to diffuse bilateral alveolar opacities. (C) CT chest showing bilateral ground-glass opacities with patchy consolidations consistent with diffuse alveolar haemorrhage. (D) Follow-up chest radiograph demonstrating marked resolution of pulmonary infiltrates after treatment.
One day later, he presented as an emergency with high-grade fever (temperature 39.5°C) and acute-onset breathlessness. He was tachycardic (HR 140/min), tachypnoeic (RR 48/min) using his accessory muscles, hypoxic (SpO₂ 40% on room air), and hypotensive (BP 98/60 mmHg). Arterial blood gas analysis showed severe metabolic acidosis with hypoxaemia (pH 7.27, pCO₂ 27 mmHg, pO₂ 22 mmHg, HCO₃− 12.4 mmol/L on FiO₂ 21%; PF ratio 104).
He was admitted to the intensive care, where repeat laboratory investigations revealed a haemoglobin of 8.9 g/L, total leukocyte count 6.89 × 109 /L, platelet count 64 × 109/L, total bilirubin level of 61.6 µmol/L, AST 160 U/L, ALT 380 U/L, urea 19.5 mmol/L, and creatinine 97.2 µmol/L. A repeat chest radiograph now showed bilateral homogeneous opacities (Fig. 1B). Contrast-enhanced CT scan demonstrated bilateral consolidation with interlobular septal thickening and thin-walled cystic changes (Fig. 1C).
At deeper questioning, our patient reported recent exposure to waterlogged wheat fields following heavy rainfall. In view of this exposure and clinical deterioration, he was started empirically on intravenous piperacillin–tazobactam, doxycycline, and trimethoprim–sulfamethoxazole, with noninvasive ventilation (NIV) (BiPAP) at an inspiratory positive airway pressure of 16 cm H₂O, expiratory positive airway pressure of 6 cm H₂O, and FiO₂ of 100%.
Subsequently, Leptospira IgM antibodies returned positive. Other investigations, including HIV, dengue NS1 antigen, dengue serology, malarial antigen test, ANA, PR3, MPO, anti-GBM antibodies, and urine routine microscopy and sputum CBNAAT, were negative.
In view of progressive anaemia, thrombocytopenia, and clinical radiological features, a severe pulmonary haemorrhage secondary to leptospirosis was established. Treatment with methylprednisolone (1 g od), ceftriaxone, and cotrimoxazole demonstrated significant clinical improvement within 48 h, with a gradual reduction in oxygen requirement which thus enabled weaning from NIV support. After completion of pulse therapy, he was transitioned to a tapering dose of oral prednisolone.
By day 5 of steroid initiation, our patient was completely weaned off from ventilator support. A follow-up chest radiograph at discharge showed marked radiological improvement (Fig. 1D). Oral doxycycline, cotrimoxazole, and tapering doses of prednisolone were continued.
Discussion
Severe pulmonary haemorrhage is an uncommon yet life-threatening complication of leptospirosis, occurring in approximately 5–10% of cases, but increasing to 20–70% in severe disease.1,2 It typically develops during the immune phase, usually 4–7 days after symptom onset, and carries a high mortality rate of 50–70%.1,3
It results from immune-mediated pulmonary capillary inflammation, leading to increased alveolar-capillary permeability and diffuse alveolar haemorrhage, rather than direct bacterial invasion.2,3 Clinically, patients present with rapidly progressive dyspnoea, bilateral infiltrates, and declining haemoglobin and platelet counts.
In endemic areas, leptospirosis should be considered early, especially when there is a history of exposure to contaminated water. The diagnosis relies on serological confirmation along with exclusion of mimickers such as tuberculosis, dengue, malaria, and pulmonary vasculitis.1,4
Early treatment with antibiotics such as ceftriaxone or doxycycline, along with adjunctive pulse methylprednisolone, may significantly reduce immune-mediated lung injury and improve clinical outcomes,3,4 demonstrated by our case of favourable recovery without requiring invasive mechanical ventilation
Footnotes
Acknowledgement
We thank the patient and his family for their trust and consent to share her clinical details. We also appreciate the support of our ICU staff for their valuable role in management.
Ethics approval
Ethical approval was not required for this case report in accordance with institutional policy.
Written consent for publication
Written informed consent was obtained from the patient and can be provided to the journal on request.
Author contributions
KS and PKD conceptualised the case report, data collection and supervised patient management. VV, KP, and BK contributed to literature review, manuscript drafting, manuscript writing, critical revision, and final approval of the version to be published.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of data and materials
No additional datasets are available beyond those described in the manuscript.