
Abstract
Malignant bowel obstruction (MBO) is a known, devastating complication of advanced intra-abdominal malignancy. International management guidelines are derived from high-income settings and rely on resources: computed tomography, self-expanding metal stents, total parenteral nutrition, specialist palliative care, that are inconsistently available in low- and middle-income countries (LMICs). Clinicians in LMICs therefore manage MBO within a fundamentally different diagnostic and therapeutic landscape, usually without context-specific guidance. Surgery dominates management but carries high morbidity and mortality, particularly in patients with ECOG performance status ≥3, serum albumin <30 g/L, ascites and peritoneal carcinomatosis. Emerging LMIC-based data confirm these patterns: a prospective Kenyan series reported 30-day postoperative mortality of 10.8% for malignant obstruction, while a South African review of 510 obstructed colorectal cancer patients found stomas were used twice as frequently as stents, the reverse of high-income country practice. No prognostic tool has been validated in LMIC populations. MBO care in LMICs demands a recalibration of international evidence to local realities. Our proposed context-adapted decision framework offers a structured, evidence-informed approach to rational surgical decision-making that can be applied immediately, even in settings lacking advanced imaging or endoscopic services.
Keywords
Introduction
Malignant bowel obstruction (MBO) is a clinical syndrome defined by mechanical or functional impairment of bowel transit in a patient with intra-peritoneal malignancy or an extra-abdominal primary with peritoneal metastases. It complicates an estimated 3–15% of all cancers, but the incidence rises to 25–40% in colorectal cancer, 20–51% in epithelial ovarian cancer and 6–19% in gastric cancer.1–3 The prognosis is uniformly poor: median overall survival after onset ranges from one to three months, and in inoperable patients it is often fewer than four weeks.1,4 In an Australian tertiary cancer centre series, 40% of patients with MBO died within 90 days of index admission, and hypoalbuminaemia (OR 3.33 for albumin <30 g/L) together with peritoneal carcinomatosis (OR 5.80) were the strongest independent predictors of early death. 5
Current international management guidelines are built almost entirely on evidence generated in high-income countries (HICs).2,6,7 They assume routine availability of contrast-enhanced computed tomography (CT), self-expanding metal stents (SEMS), total parenteral nutrition (TPN), interventional radiology and multidisciplinary palliative care teams. Even in well-resourced environments, however, the evidence base is thin: a systematic review of 15 studies involving 882 patients with malignant small-bowel obstruction found no randomised controlled trials, and 30-day surgical mortality in operated patients ranged from 13% to 28%. 8
Low- and middle-income countries (LMICs) face a rapidly escalating cancer burden super-imposed on persistent late-stage presentation. An estimated 70–80% of cancers in LMICs are incurable at diagnosis, owing to limited screening, low health literacy and inadequate referral pathways. 9 A systematic review of delays in cancer care across LMICs identified that the costs of diagnostic and treatment services, geographical inaccessibility and poor health literacy were the dominant drivers of late presentation, with median patient-associated delays ranging 2- 24 months across tumour types. 10 Cervical cancer, with an age-standardised incidence of approximately 40 per 100,000 women, remains the leading cause of female cancer death in 21 of 48 LMICs, more than ten times the WHO elimination target of 4 per 100,000. 11 In contrast to HICs, where bowel obstruction from cervical cancer is rare, this cancer in LMICs frequently causes rectosigmoid obstruction through extrinsic compression, a mechanism for which SEMS is technically ineffective even when available. 12 Ovarian cancer-related MBO in LMICs typically occurs in the absence of any prior cytoreductive surgery or systemic chemotherapy, and with profound nutritional depletion. Colorectal cancer, which is increasing in incidence across the region, presents as a surgical emergency in nearly 33% of cases and is associated with 30-day postoperative mortality rates that consistently exceed 20%. 13 A recent scoping review of emergency colorectal cancer presentation across Africa documented rates varying from 8.3-64.9%, with the highest figures reported from Nigerian and Sudanese cohorts, and confirmed that surgery remains the mainstay of treatment while endoscopic stenting was only available as a treatment option in parts of South Africa. 14
The diagnostic and therapeutic infrastructure gap is structural. A survey of ten Nigerian secondary hospitals found that seven had no CT scanner, and the single existing machine was inoperable. 15 SEMS, TPN and specialist palliative care services are similarly scarce or absent. Consequently, LMICs clinicians must navigate the management of MBO by a combination of extrapolation from HIC evidence, institutional habit and clinical improvisation, without the staging precision, prognostic scores or therapeutic optionality that their HIC counterparts command. Palliative surgery in resource-constrained African settings has been described as a largely undocumented activity, carried out without protocols or outcome data. 16
In response to this evidence-practice chasm, our review aims to (i) synthesise the available global evidence on MBO epidemiology, diagnosis, prognostic assessment and management; (ii) critically appraise the applicability of this evidence, integrating published Africa-specific data from surgical, oncological and palliative care settings across the continent; and (iii) propose a structured, resource-stratified clinical decision algorithm that is practical and applicable at the bedside with only serum albumin as a laboratory investigation.
Methods
Ours is a structured narrative review. To minimise selection bias, systematic search principles were embedded, and the selection process is documented according to PRISMA principles in a flow diagram (Fig. 1).
A structured literature search was performed across PubMed/MEDLINE, EMBASE, African Journals Online and the Cochrane Library for studies published in English between January 2000 and January 2026, using: “malignant bowel obstruction,” “malignant intestinal obstruction,” “bowel obstruction” AND “cancer” or “malignancy,” and “intestinal obstruction” AND “neoplasm,” and adding: “sub-Saharan Africa,” specific country names, “low-income,” and “resource-limited,” “palliative surgery,” “colostomy,” “bowel diversion,” “self-expanding metal stent,” “octreotide,” “palliative care,” “peritoneal carcinomatosis.” Reference lists of included systematic reviews, meta-analyses and clinical guidelines were hand-searched. GLOBOCAN 2022 and the IARC Cancer Atlas were accessed for regional epidemiology.
Studies were included if they were primary research articles (observational cohorts, case series, randomised trials), systematic reviews, meta-analyses or clinical guidelines reporting on the epidemiology, diagnosis, management or outcomes of MBO in adult patients (≥18 years) with intra-abdominal or pelvic malignancy or peritoneal metastases. Publications that focused exclusively on benign bowel obstruction, paediatric populations or in a language other than English were excluded. Conference abstracts and grey literature from African surgical and oncological meetings were also considered where they provided extractable MBO-relevant data.
Results
Our search identified 68 titles and abstracts, of which 53 full-text articles were assessed for eligibility, with 37 satisfying all inclusion criteria (fig. 1). Three grey literature sources were included for contextual relevance but were not weighted the same as peer-reviewed studies in the synthesis.
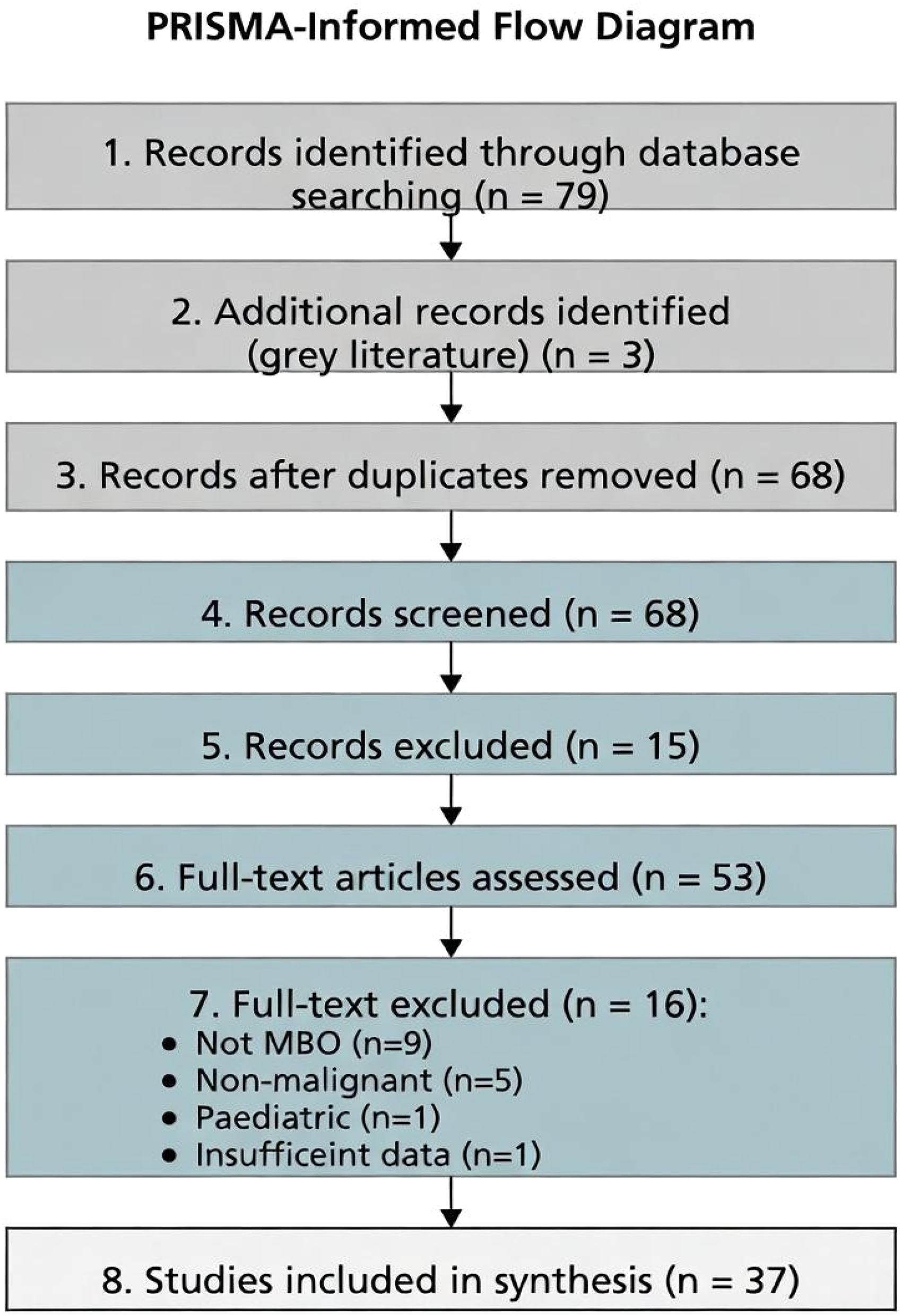
PRISMA-informed flow diagram.
Data were extracted into a standardised form and synthesised thematically across the following domains: epidemiology & aetiology, pathophysiology, clinical presentation & diagnosis, prognostic assessment & patient selection, non-surgical management and surgical management. For each domain, global evidence was reviewed first, followed by an explicit discussion of its applicability and limitations in the LMIC setting. Where LMICs-specific data existed, these were used to frame the contextual discussion; where none was available, the evidence gap was explicitly acknowledged. Because of marked heterogeneity in study design, populations and outcome definitions, no statistical pooling was performed. The resource-stratified clinical algorithm was developed inductively from the synthesised evidence.
Table 1 presents the causative malignancy in MBO with global incidence data and LMIC-specific contextual notes. Highlights are: (1) cervical cancer as a major cause of MBO in LMICs; (2) ovarian cancer-related MBO in the absence of prior cytoreductive surgery or systemic chemotherapy, with profound nutritional depletion5,17; and (3) unknown primary cancer. 18 A younger age at presentation for colorectal cancer in LMICs is seen (peak c.44 years)19,20 with (25–31%) presenting as surgical emergencies.13,14
Causative malignancies in MBO, global incidence data with sub-Saharan African contextual notes.
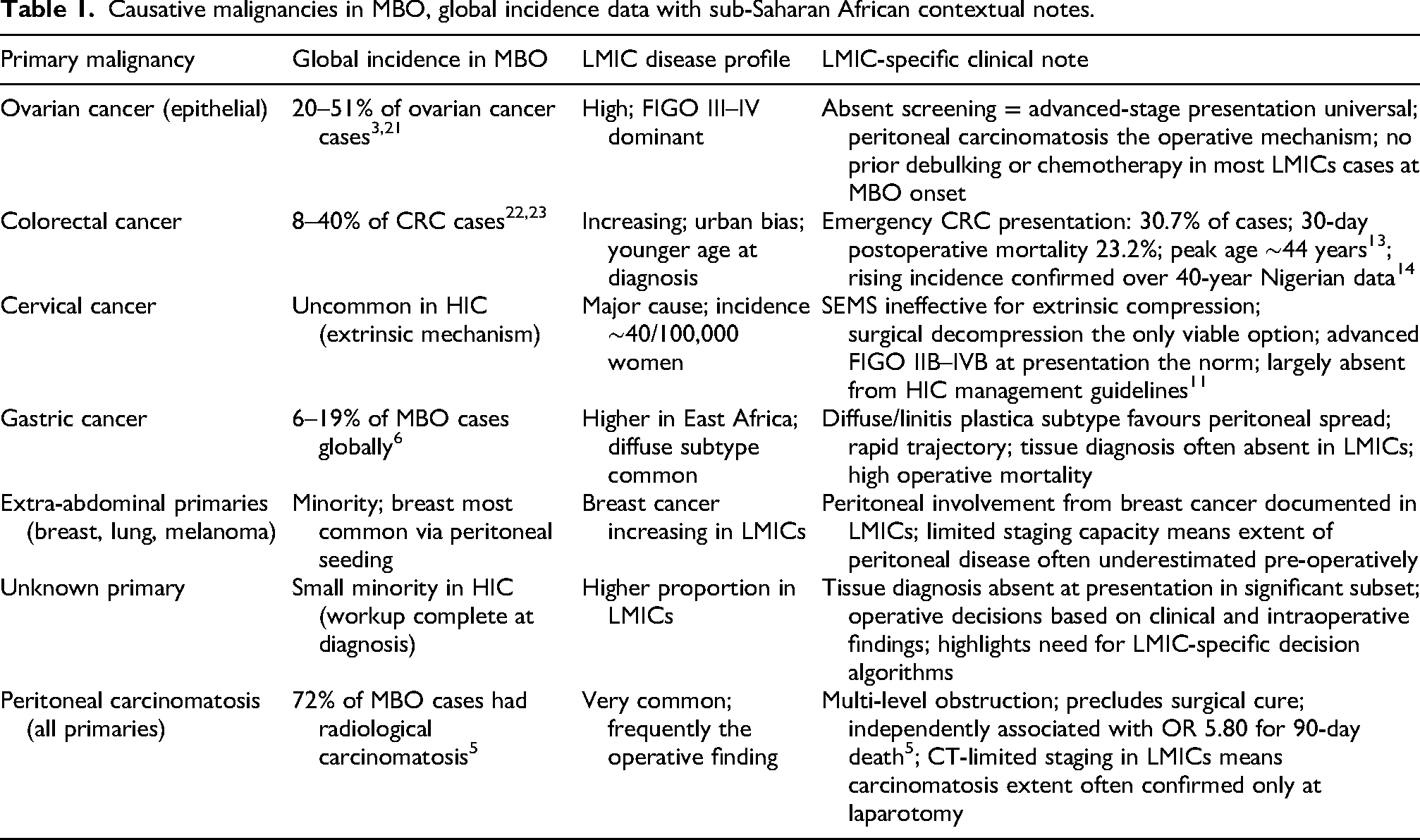
Table 2 presents diagnostic modalities for MBO, comparing performance characteristics, LMIC availability and clinical roles. Plain abdominal X-ray (sensitivity 50–80%) remains the most widely available first-line screening tool. Abdominal ultrasound, available in most LMIC secondary hospitals, reliably demonstrates ascites, hepatic metastases, pelvic masses and gross bowel dilatation but cannot stage peritoneal carcinomatosis with surgical precision. 24 The table supports a pragmatic, resource-stratified diagnostic approach prioritising clinical assessment, including mandatory bedside ECOG performance status grading, physical examination for ascites and cachexia and serum albumin measurement.
Diagnostic modalities for MBO, performance characteristics, LMIC availability and clinical role.
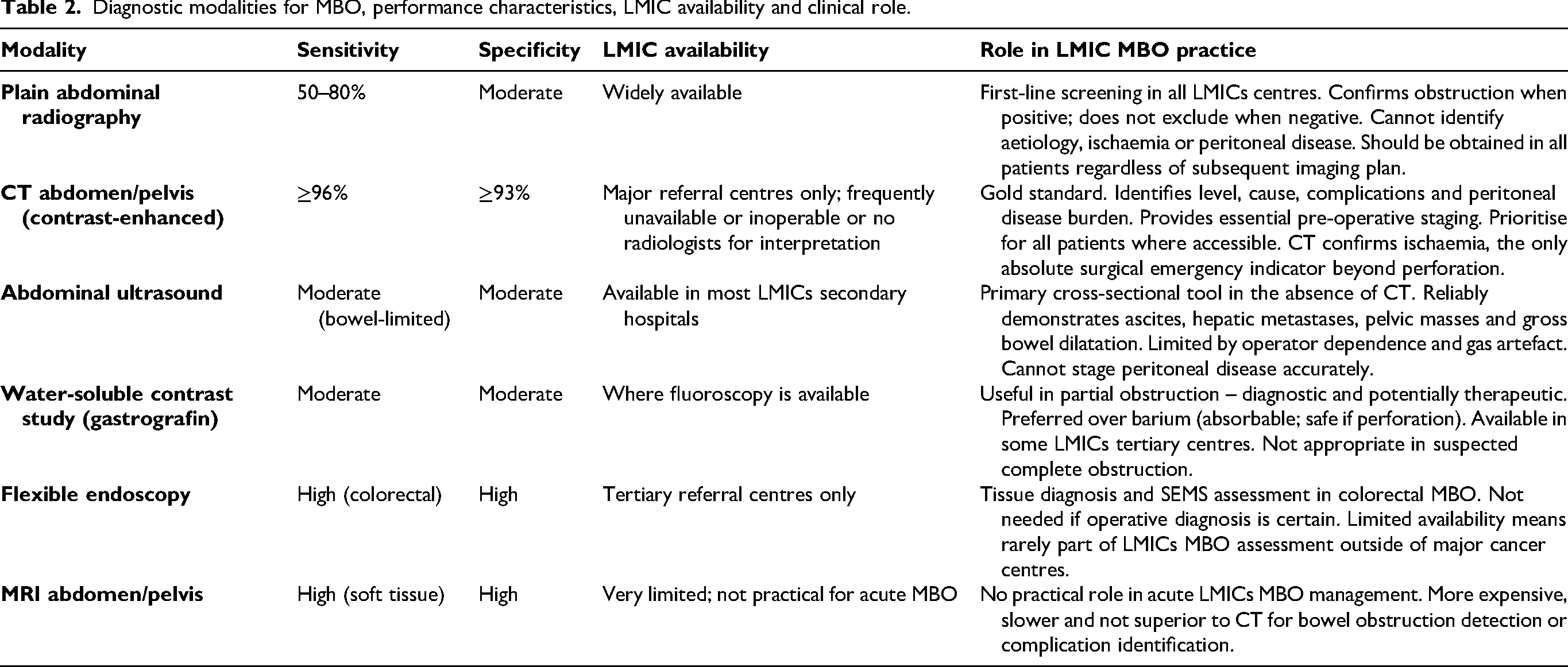
Table 3 synthesises evidence-based predictors of poor surgical outcome in MBO with their applicability in LMICs, where no prognostic scoring system has been validated. The strongest, most consistently replicated predictors include ECOG performance status ≥3 (median survival 27 days), 4 serum albumin <30 g/L (odds ratio 3.33 for 90-day death),5,25 peritoneal carcinomatosis (odds ratio 5.80), 5 gross ascites,2,26 multi-level obstruction12,27 and multiple malnutrition markers. 28 The Kenyan prospective series, 29 the only prospective LMIC study specifically examining surgical outcomes of malignant intestinal obstruction, reported 30-day postoperative mortality of 10.8% in a cohort where 62.7% of tumours were T4 and 57.6% had metastatic disease at presentation.
Evidence-based predictors of poor outcome in MBO surgery – clinical applicability in LMICs.
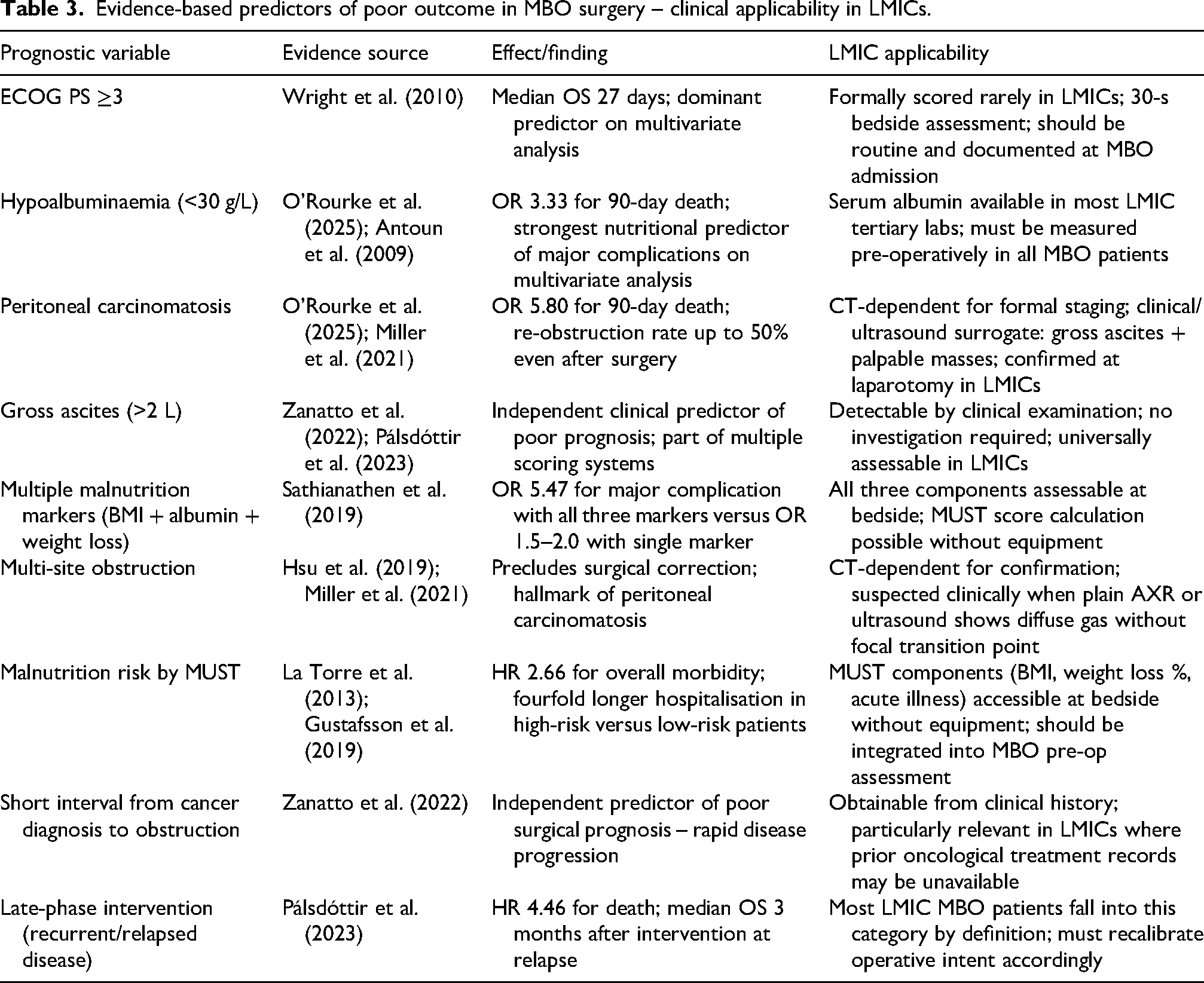
Table 4 details pharmacological agents for non-surgical MBO management with mechanisms, dosing, evidence levels and LMIC applicability. Hyoscine butylbromide (40–120 mg/day IV or SC) is the first-line antisecretory agent in LMICs, being low-cost, widely available and on essential medicines lists.2,6 Dexamethasone (8–16 mg/day IV) provides dual anti-oedema and antiemetic effects. 27 Haloperidol (0.5–2 mg qds IV/SC) is the preferred antiemetic in complete obstruction as it lacks prokinetic activity.6,7 Total parenteral nutrition has no evidence-supported role in routine MBO management, being far too costly for the benefit obtained.
Pharmacological agents for non-surgical MBO management – evidence base, dosing and LMIC applicability.
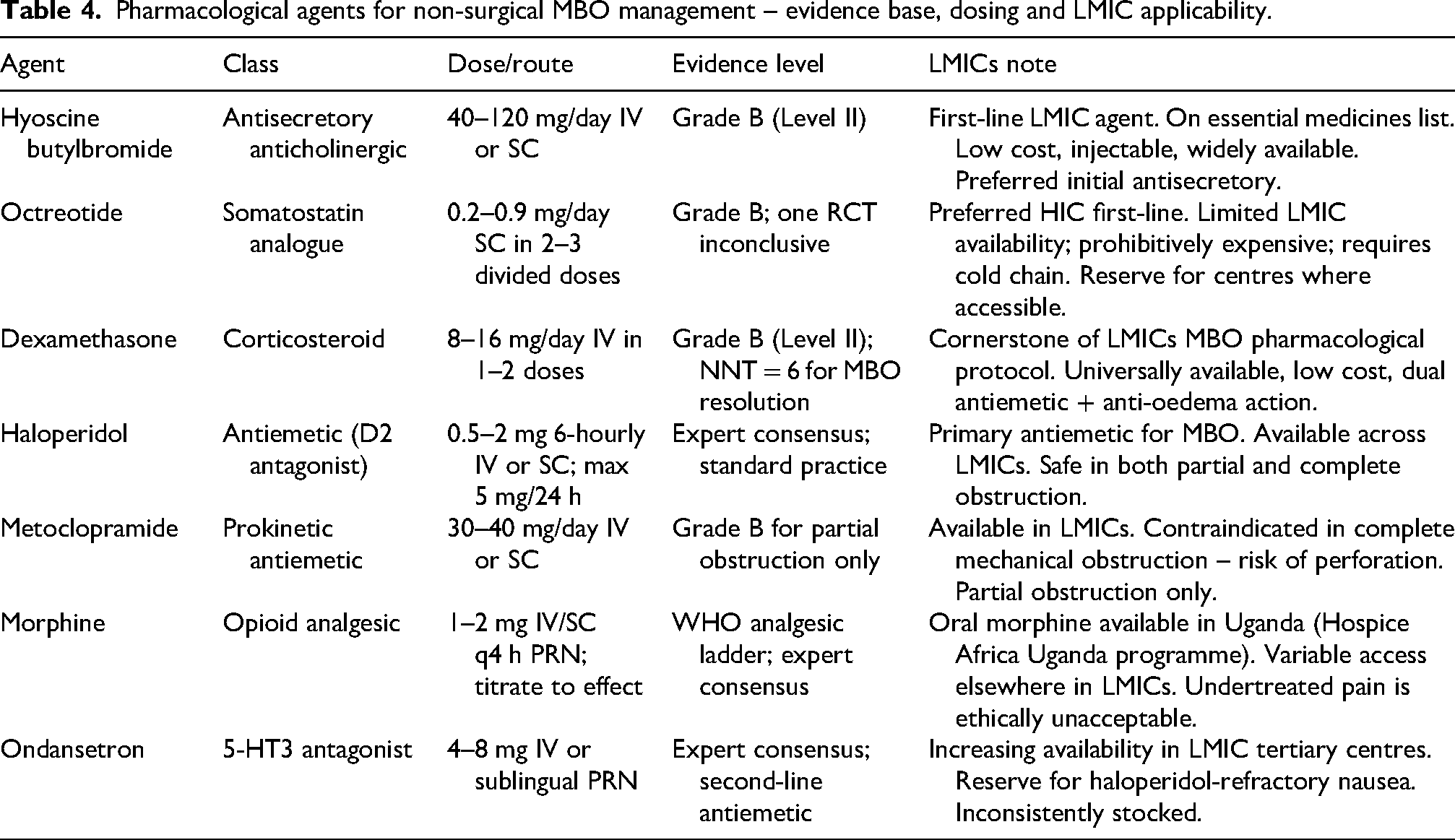
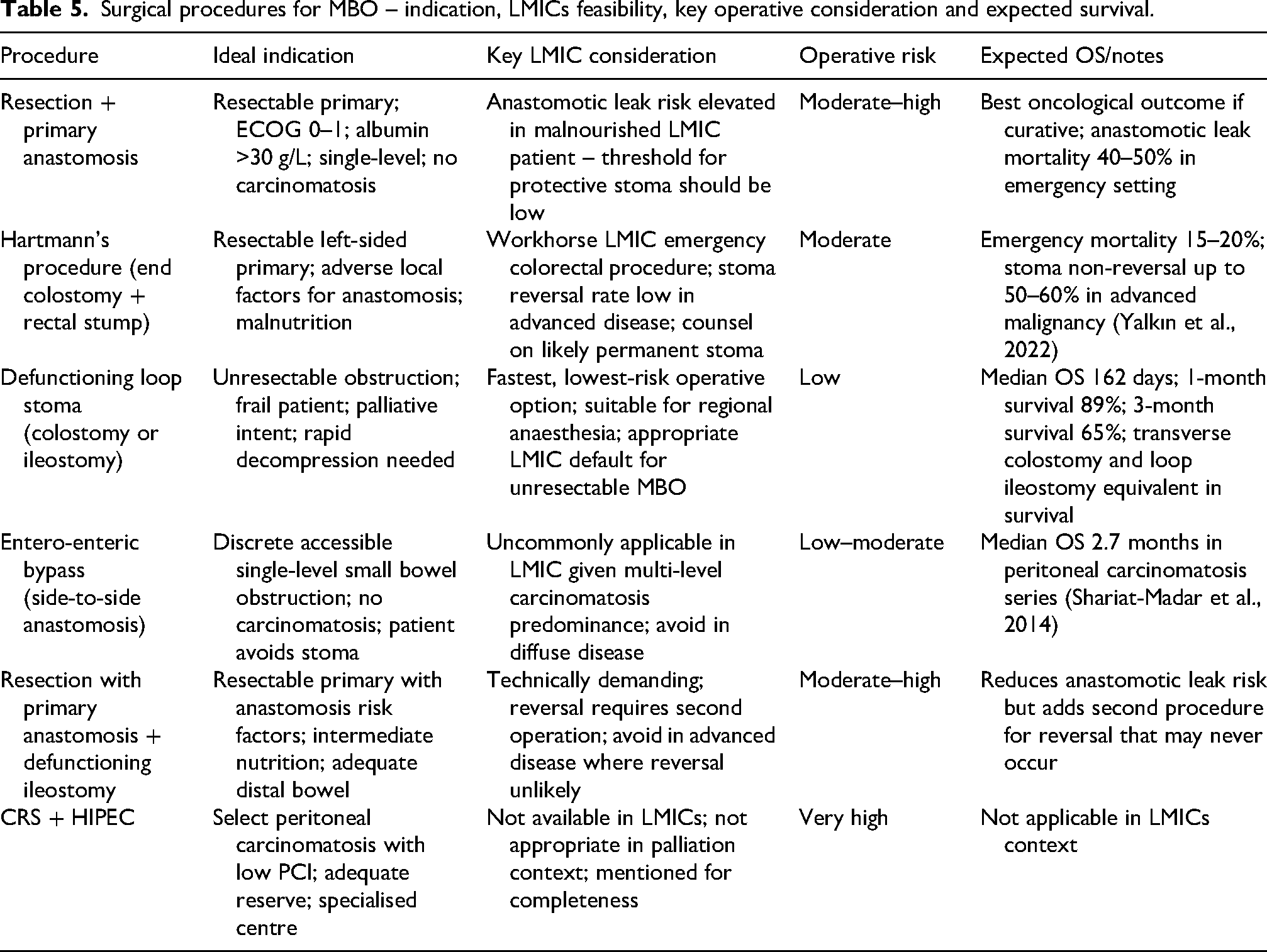
Table 5 summarises surgical procedures for MBO with indications, LMIC feasibility, operative risk and expected outcomes. Hartmann's procedure is the workhorse emergency colorectal procedure for left-sided MBO in LMICs.29,30 Defunctioning loop stoma (loop ileostomy or transverse colostomy) is the fastest, lowest-risk operative option for unresectable obstruction or very frail patients, feasible under regional anaesthesia in 20–40 min. 31 The Burkina Faso series 32 of 639 palliative digestive cancer surgeries demonstrated 76% very satisfactory symptom improvement. MBO recurs in up to 49% of patients within 90 days of surgery. 5 Stenting is well-nigh impossible.
Surgical procedures for MBO – indication, LMICs feasibility, key operative consideration and expected survival.
We propose a resource-stratified clinical algorithm (fig. 2) which accepts diagnostic uncertainty as a constitutive feature of the LMIC clinical encounter and provides a framework for navigating that uncertainty in a structured, evidence-informed manner.

Clinical algorithm for the diagnostic evaluation and multidisciplinary management of malignant bowel obstruction in advanced malignancy.
Proceed to laparotomy with intent for resection and primary anastomosis where anatomy and nutrition permit, or a diversion stoma where they do not. Median survival 222 days; appropriately selected surgical candidates have a 60–80% chance of achieving durable symptom control.2,4
Initiate a 48-72 h trial of aggressive conservative management with serial reassessment. If obstruction resolves, transition to pharmacological palliation and diet modification. If no resolution, consider limited surgical intervention, defunctioning loop stoma or bypass, rather than definitive resection.
Palliate pharmacologically. Median survival for ECOG 3–4 is 27 days regardless of intervention; peritoneal carcinomatosis itself carries an OR of 5.80 for 90-day death.4,5
Discussion
First, the epidemiology and aetiology of MBO in LMICs differ substantially from HICs. Second, the diagnostic and therapeutic infrastructure gap constitutes a structurally transformative constraint. Third, no prognostic assessment tool has been validated in LMICs populations.
The strength of this review lies in its explicit focus on clinical applicability and its integration of a broad range of Africa-specific primary evidence.
The limitation is the narrative methodology, which, while appropriate, precludes quantitative meta-analysis and is susceptible to selection bias. The LMIC-specific primary literature on MBO remains sparse; much of the contextual analysis is therefore inferential, and many of the studies cited report on mixed-aetiology intestinal obstruction rather than isolated MBO. The proposed algorithm has not been prospectively validated, and there is wide heterogeneity of existing LMIC health systems.
Prospective multicentre MBO cohort studies in LMICs are needed to document tumour types, stage distribution, nutritional and performance status at presentation, management pathways and 30- and 90-day outcomes. An LMIC-specific MBO prognostic score, derived from and validated against surgical outcomes using universally bedside-assessable variables, is urgently required. Pragmatic pharmacological trials should evaluate the efficacy, feasibility and cost-effectiveness of locally available MBO regimes. Implementation research is needed to determine the best approaches to integrate palliative care into surgical MBO pathways in settings where such specialist services are scarce or non-existent.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.