
Abstract
Partial molar pregnancy co-existing with a live fetus is a rare obstetric condition posing diagnostic and management challenges.
Case report
A 20-year old primigravida with partial molar pregnancy of 22 weeks’ gestation (POG) was referred for medical termination of pregnancy. She had on-and-off spotting for the previous month. There was no genetic nor obstetric abnormality in her family. Clinical examination showed a 24–26 weeks sized uterus. An ultrasound scan revealed no congenital fetal abnormalities, a normal Doppler study and cystic placenta changes of snowstorm appearance (Figure 1) at some suggestive of placental mesenchymal dysplasia (PMD) or molar gestation with co-existing with a fetus.
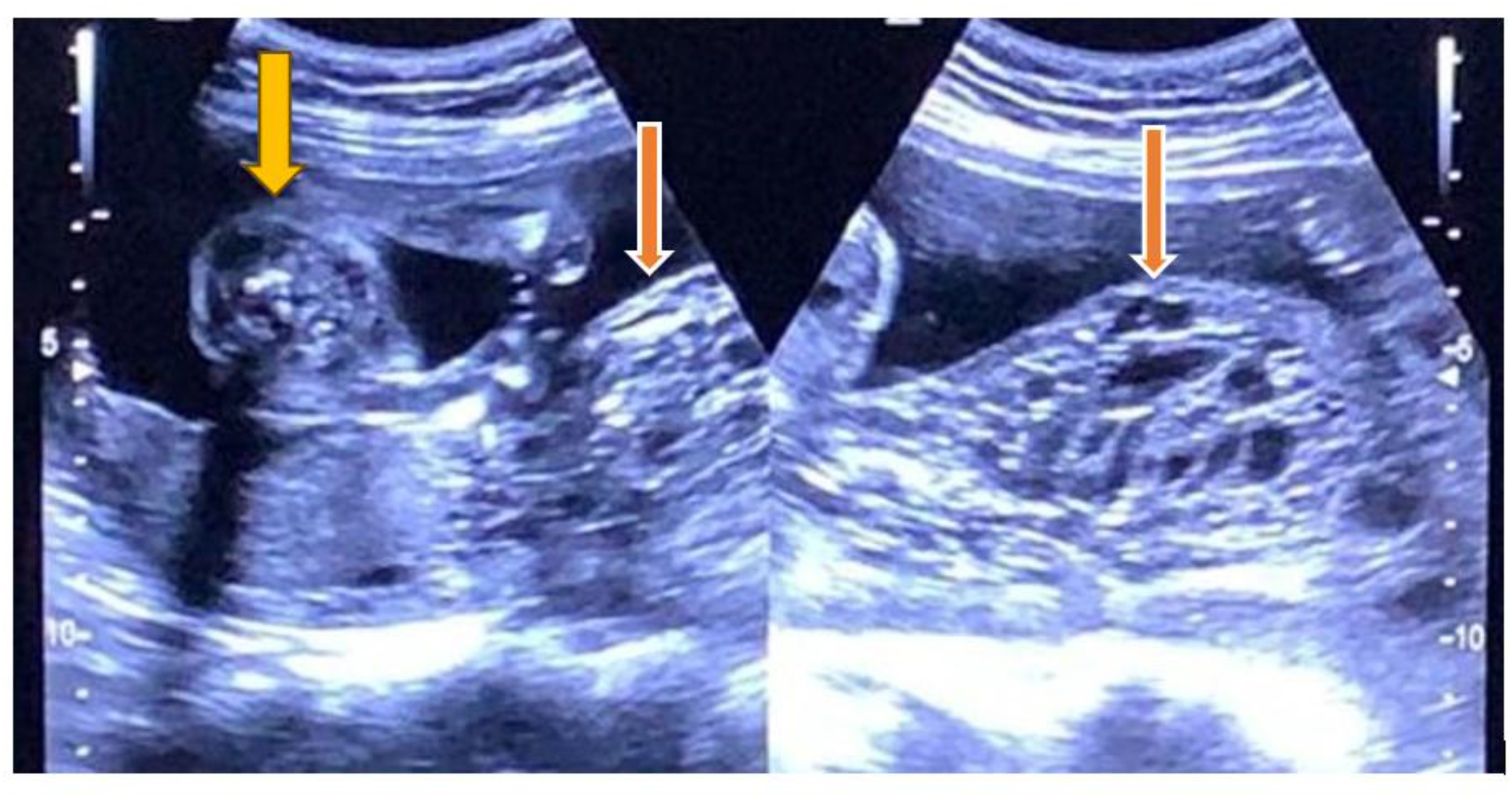
Cystic placenta changes of snowstorm appearance at some suggestive of placentaL mesenchymal dysplasia (PMD) or molar gestation with co-existing with a fetus.
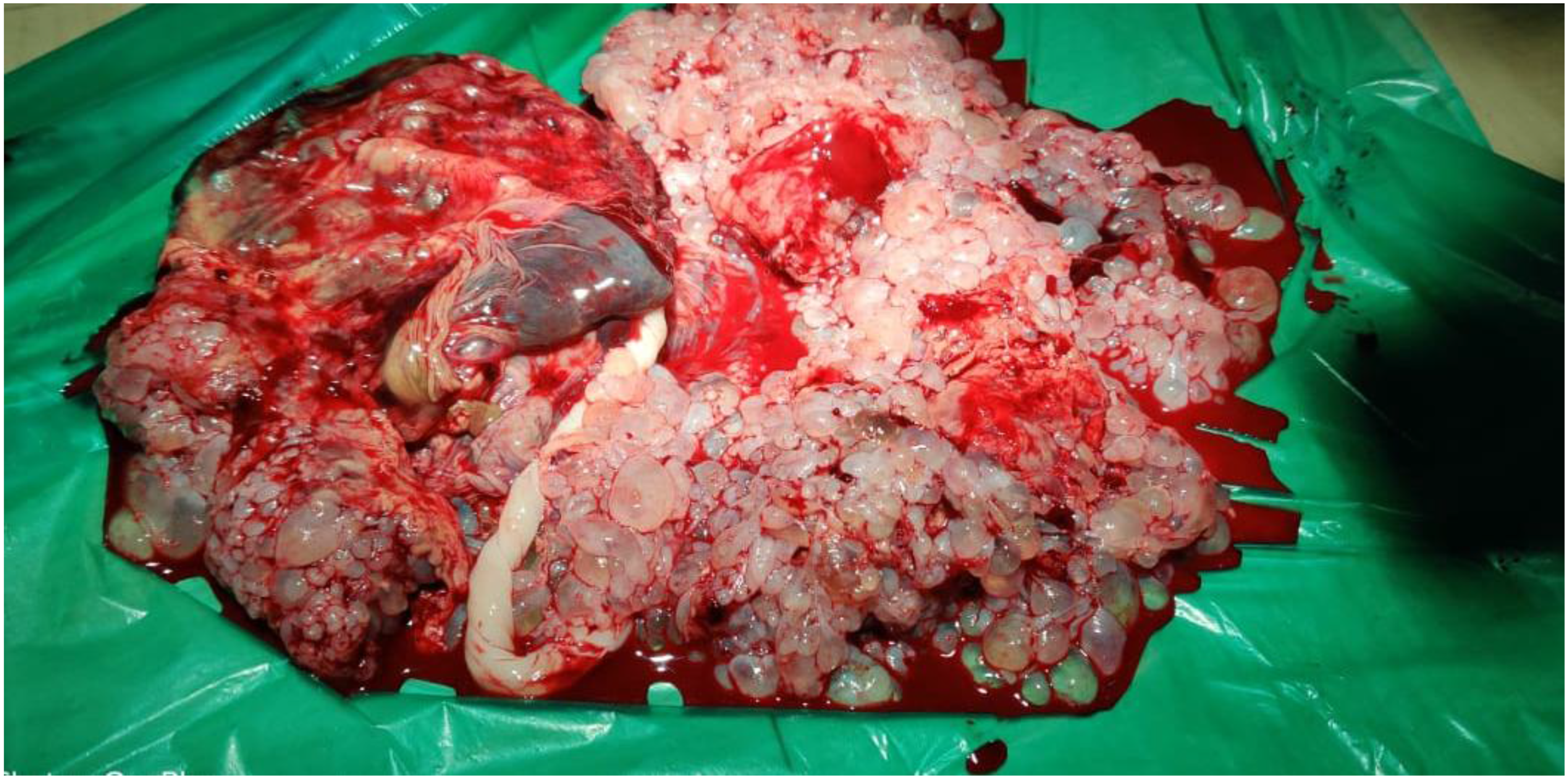
Placenta with many groups of grape-like vesicular cystic structures.
β-hCG values were found to be elevated (255 IU/ml), the chest radiograph normal and thyroid function test within normal limits.
Close antenatal surveillance was carried out at regular 2-weekly intervals, with ultrasound scan and other investigations. Mild pre-eclampsia occurred at 30 weeks’ gestation prompting treatment Labetalol 100 mg bd. No placental insufficiency or oligohydrominos developed at 34 weeks spontaneous labour resulted in the delivery of a male baby of 1.7 kg and a placenta with many groups of grape-like vesicular cystic structures (Figure 2). The postpartum was uneventful. Histopathological examination of the placenta showed scalloped villi, trophoblastic proliferation, and hydropic degeneration consistent with a partial mole. The β-hCG was serially monitored weekly for 7 weeks till normalisation levels (<2 mIU/ml) two times.
The baby was normal karyotypic (46XY) and healthy at the last follow-up at 1 year.
Discussion
Molar pregnancy, otherwise known as hydatidiform mole (HM), is a gestational trophoblastic disease (GTD), characterised by abnormal fertilisation, resulting in villous hydrops and trophoblastic hyperplasia with or without embryonic development. 1 It is classified into complete and partial HM. In complete moles, the fetus is absent while in partial molar pregnancy, a fetus may coexist. 2
Ultrasound scan is the diagnostic modality of choice and shows a honeycomb-like echo or a snowstorm appearance in the placenta. 3 HM is mostly reported with significantly higher β-hCG level. 4 Distinguishing between PMD, complete mole with coexisting fetus, and partial molar pregnancy antenatally can be difficult because of overlapping imaging characteristics. In our case, the markedly elevated β-hCG level supported the diagnosis of GTD, while definitive confirmation was obtained only after histopathological examination of the placenta.
Early diagnosis improves the prognosis as complications such as haemorrhage, pre-eclampsia, hyperthyroidism, and risk of persistent gestational trophoblastic neoplasia can be closely monitored. 5
Successful continuation of pregnancy is associated with favourable prognostic factors such as a structurally and chromosomally normal fetus, preserved fetal growth, normal Doppler findings, and absence of severe maternal complications. 6 In our case, these factors supported expectant management despite markedly elevated β-hCG levels. The stable maternal condition, confirmed fetal viability, close multidisciplinary surveillance, comprehensive counselling, and shared decision-making contributed to the delivery of a healthy infant and uncomplicated maternal recovery.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.