
Abstract
Burnout, as a work-related phenomenon, has negative consequences on employee functioning and is well documented. What is deserving of further investigation is how effort-recovery processes may be affected, in this instance, sleep. The purpose of this study was to investigate whether significant sleep difficulties are reported when employees report experienced burnout, while also controlling for age, gender, exercise, smoking habits, and treatment for depression. A cross-sectional survey design was used in data collection. The sample consisted of 734 participants with white collar positions in the financial industry of South Africa. Structural equation modelling methods were implemented in order to investigate the hypotheses. The results of the structural model indicated that burnout was significantly related to sleep difficulties, even in the presence of reported treatment for depression, and the other control variables. The correlations between burnout, treatment for depression, as well as sleep difficulties were all positive and practically significant. The results, recommendations, limitations, and practical implications of the study are discussed.
The average white collar employee (e.g., technical, professional, managerial, and sales occupations; Maume & Houston, 2001), spends an average of 8 hours hr a day working during a normal working week (Ramutloa, 2008). The only activity that would demand a similar amount of time from the day would be time spent sleeping. The combination of these two activities makes up the majority of any employee’s workday. Interestingly, research has not yet agreed on the essential purpose of sleep; but theories indicate that sleep, inter alia, restores homeostasis in the central nervous system and may allow the processing of affective information (cf. Everly & Lating, 2013), and thus is an important effort-recovering factor in combatting the development of burnout-related symptoms.
Job stress and effort-recovery
Work calls for a significant investment of self, in the form of job demands, in the average employee working day. These job demands induce stress, which in turn initiates mind–body arousal. If these demands are perceived as threatening, the employee reacts with anxiety, which activates the autonomic nervous system (Spielberger, Vagg, & Wasala, 2003). Moreover, employees who experience stress are inclined to utilise more alcohol and cigarettes, but also sleep and exercise less (Maslach & Jackson, 1982). The Effort-Recovery Model (Meijman & Mulder, 1998) posits that work requires an employee to expend effort during the day and that this leads to certain load reactions in the employee (behavioural, physiological, and subjective); the load from the aforementioned reactions can be reversed if the employee returns to his or her normal psychobiological state, that is, is no longer confronted with demands, and then recovers to his or her pre-demand levels (cf. Meijman & Mulder, 1998; Sonnentag, 2001). It is therefore important to research the effects that work, especially work stress and its pinnacle outcome, burnout, may have on sleep, as sleep plays an important role in the effort-recovery of employees. Indeed, research has found that insufficient effort-recovery from work stress leads to burnout and eventual health impairment of employees (Geurts & Sonnentag, 2006).
Job burnout and the health impairment process
Job burnout has been extensively researched (cf. Bakker, Demerouti, & Sanz-Vergel, 2014; Schaufeli & Buunk, 2003; Schaufeli, Leiter, & Maslach, 2009; Shirom, 2003) and has been defined as ‘a persistent, negative, work-related state of mind in normal individuals that is primarily characterized by exhaustion, which is accompanied by distress, a sense of reduced effectiveness, decreased motivation, and the development of dysfunctional attitudes and behaviours at work’ (Schaufeli & Enzmann, 1998, p. 36). Furthermore, job burnout has classically been operationalised as comprising three components (exhaustion, cynicism, and lowered professional efficacy; Maslach & Jackson, 1981; Maslach & Leiter, 1997), but in more recent times, also as consisting of two core components (exhaustion and cynicism; Schaufeli & Taris, 2005). The current study subscribes to the two core component operationalisation of job burnout. Moreover, recent research has also suggested that investigation of burnout as a global construct might be necessitated as opposed to its individual components (Mészáros, Ádám, Szabó, Szigeti, & Urbán, 2013). The latter study also showed professional efficacy to be separate from the global burnout construct. The job demands–resources (JD-R) model provides a theoretical context to explain burnout’s development in the work environment. In the JD-R model’s health impairment process, distress in the form of chronic job demands leads to a deterioration of energy levels into exhaustion, cynicism, and the eventual state of burnout (Bakker & Demerouti, 2007; De Beer, Rothmann, & Pienaar, 2012). Burnout then leads to various negative outcomes for the employee and the organisation: that is, psychological ill-health, eventual physical ill-health, and a reduced sense of commitment to the organisation (Bakker & Demerouti, 2007; De Beer et al., 2012; Schaufeli & Bakker, 2004).
Stress, burnout, and sleep difficulty
It is known that stress can lead to problems with sleep (Jansson & Linton, 2006). One could then extrapolate to say that burnout, as the extreme outcome of prolonged work stress, may elicit a similar if not a more severe reaction. Some research concerning burnout and sleep exists and has included a focus on sleep impairment among females (cf. Grossi, Perski, Evengard, Blomkvist, & Orth-Gomer, 2003), and establishing that stress and burnout can also evoke somatic responses and may affect metabolic (both anabolic and catabolic) processes in individuals (cf. Ekstedt, 2005; Melamed et al., 1999). The researchers who first coined the term burnout, Herbert Freudenberger along with Gail North, suggested that burnout followed a 12-step process and that these steps are not necessarily followed sequentially – one of the former steps included the employee ‘neglecting needs’, which leads employees to increasingly regard family, friends, eating, and sleep as unnecessary aspects of their lives (cf. Kraft, 2006). Here, it is important to note that the latter mentioned neglect of sleep seems to be a wilful action by the employee due to time constraints of the normal day and is instrumental in the development of burnout. It is therefore not necessarily a sleep difficulty or disturbance that is induced due to an affliction of burnout. It has also been suggested that impaired sleep may play a role in exhaustion and burnout development (Ekstedt et al., 2006), indicating a possible reciprocal relationship.
Frequent sleep difficulties’ clinical diagnosis is insomnia, which carries the following symptoms: ‘difficulty initiating sleep, maintaining sleep, or having non-restorative sleep that is also accompanied by daytime dysfunction (DSM-IV-TR) despite adequate opportunity to sleep’ (Drake, Eklov, & Roth, 2013, p. 193). Armon, Shirom, Shapira, and Melamed (2008) investigated the effects of burnout on insomnia in a longitudinal study in Israel and indicated that burnout and insomnia influence each other in a reciprocal relationship over time. They indicate that burnout can lead to insomnia, but that insomnia could also play an important role in the development of burnout. An interesting cross-sectional study by Söderström, Ekstedt, Åkerstedt, Nilsson, and Axelsson (2004) of young individuals (24–43 years old) in the information technology (IT) industry found that if those employees were at a high burnout level, they would show more arousals from sleep and also more sleepiness on days off from work. In other research, among primary care physicians, it has been found that there is a clear relationship between burnout and insomnia symptoms, and also reduced sleep quality (Vela-Bueno et al., 2008). Furthermore, research has found that impaired sleep quality will negatively affect the recovery process of clinically burned-out individuals (Sonnenschein, Sorbi, van Doornen, Schaufeli, & Maas, 2007). A review of research by Kucharczyk, Morgan, and Hall (2012), which explored the occupational impact of sleep quality and insomnia symptoms from 30 studies, found that insomnia symptoms are associated with excess absenteeism, accident risks, reduced perception of workplace productivity, inhibited career progression, and reduced job satisfaction.
Burnout, depression, and antidepressants
Burnout and depression have been shown to be two independent and separable constructs, even though they do share some similar symptoms such as fatigue and concentration problems (Glass & McKnight, 1996; Schaufeli & Enzmann, 1998). This is important to consider, as depression has also been shown to affect the sleep of its sufferers. Some depressed individuals may sleep less (Benca & Peterson, 2008), while other depressed individuals may sleep more (Posternak & Zimmerman, 2001). According to Carver, Scheier, and Wientraub (1989), a coping strategy that can be used by some individuals includes mental disengagement in the form of day dreaming or excessive sleeping in order for the individual to escape from the stressors experienced in life. Antidepressant medications have been linked to sleep difficulties, especially when using selective serotonin reuptake inhibitors (SSRIs). Indeed, most medications that affect the central nervous system can induce insomnia in some individuals (cf. Pagel & Parnes, 2001).
Confounding variables of sleep difficulty
Other variables that have also been shown to affect sleep include age, gender, exercise, and smoking. Sleep quality, quantity, and also sleep architecture (the basic structural organisation of sleep, for example, deep sleep; Colten & Altevogt, 2006) are all affected due to changes in the normal ageing process of individuals; this is especially measurable in the elderly who have trouble initiating and maintaining sleep (Espiritu, 2008; Monjan, 2013). Moreover, gender differences also exist for insomnia, in that females have shown a greater predisposition (Zhang & Wing, 2006). Exercise has long been thought to be conducive to sleep quality, especially in epidemiologic research, but experimental research results have been less persuasive (Kline & Youngstedt, 2013). Furthermore, smokers have been shown to experience a number of insomnia-type impairments and should therefore be controlled for in research analyses concerning sleep (Jaehne et al., 2012). These control path variables were included as research has shown there is a need to recognise the potential confounding influence of these variables on occupational performance and sleep (Kucharczyk et al., 2012).
Self-report and single-item measure validity
Traditionally single-item self-report measures for constructs are frowned upon due to the widely held stance that one item may not be sufficient to measure the construct accurately. However, more recent research has found that single-item measures can be used, reliably and validly, when measuring constructs with similar accuracy compared to longer surveys measuring said construct (cf. Bergkvist & Rossiter, 2007; Cappelleri et al., 2009; Dolbier et al., 2005; Littman et al., 2006; Milton, Bull, & Bauman, 2011; Yohannes et al., 2011). These single-item measure implementations are usually used for practical reasons as opposed to purely theoretical grounds, due to attempts to minimise cost and improve uptake of potential respondents, that is, shorter surveys (less paper, completion time). This study will measure burnout with multiple items and the other variables with single categorically scaled item measures in its investigation.
The central hypothesis for this study is therefore that job burnout, measured as a work-related phenomenon, will be significantly associated with sleep difficulties even in the presence of other confounders of sleep difficulty, measured by single items, that is, reported treatment for depression, age, gender, exercise, and smoking.
Method
Participants
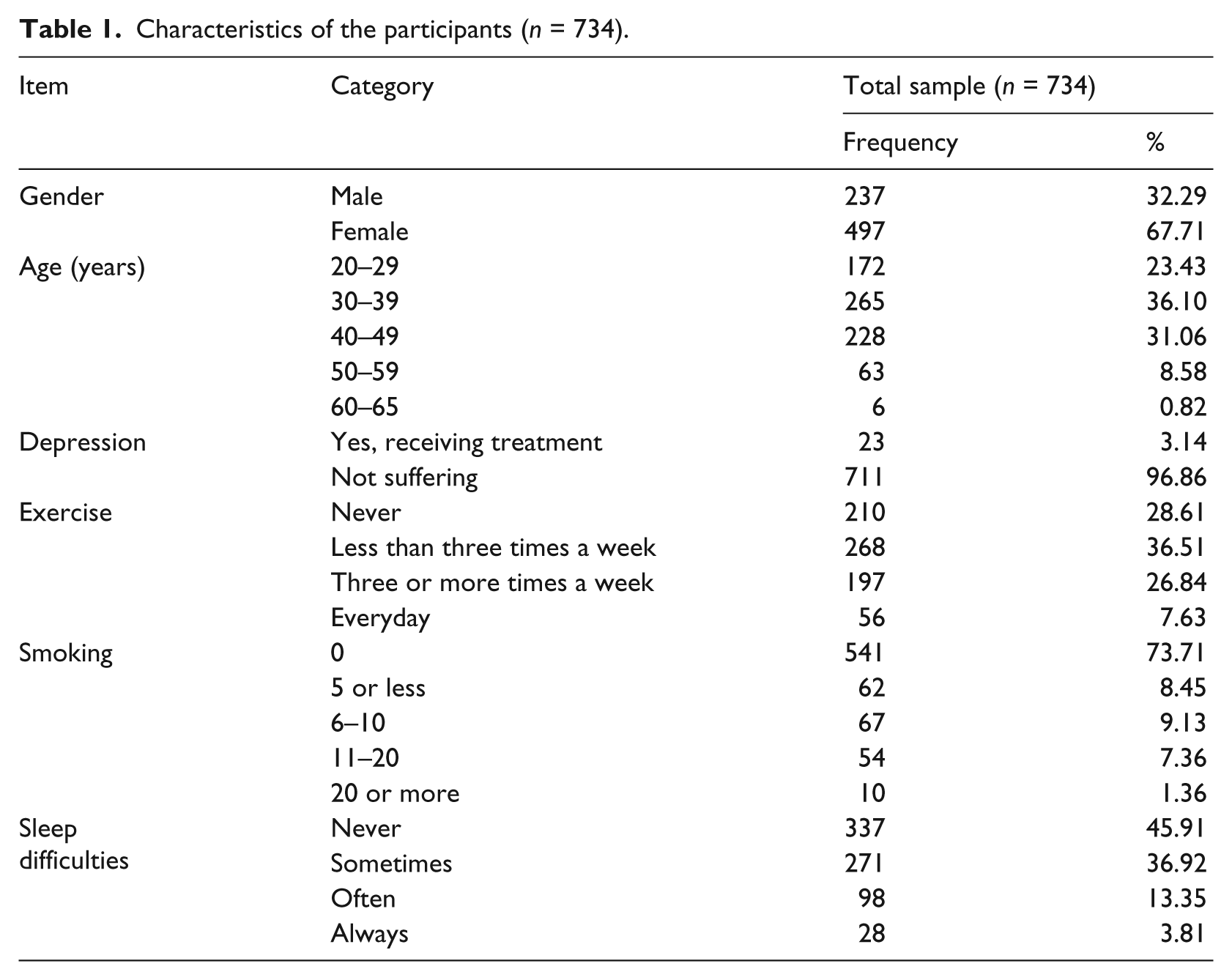
A sample of individuals (n = 734) was collected at random (Table 1). The majority of the sample consisted of female participants, 497 (67.7%), while 237 (32.3%) were male. The number of participants from the 30- to 39-years age group was the majority (265; 36.1%). The most prevalent home languages were English, with 328 (44.7%), and Afrikaans (n = 293; 39.9%). It is likely that participants who report receiving treatment for depression have been clinically diagnosed by a clinical psychologist and/or psychiatrist and have been prescribed some form of antidepressant medication (refer to discussion of ‘Measures’). The employees who explicitly stated that they are receiving treatment for depression in the available sample numbered 23 (3.14%). The majority of employees engage in insufficient exercise per week (less than three times a week; 65.12%), and most (73.7%) employees indicated that they do not smoke. Employees who experience sleep difficulty at least Often to Always numbered a combined 126 (17.2%).
Characteristics of the participants (n = 734).
Instruments
The South African Employee Health and Wellness Survey (SAEHWS; Rothmann & Rothmann, 2007) was used to measure all the constructs for this study. The internal consistency of all the subscales of the SAEHWS is satisfactory compared to generally accepted guidelines for both alpha and omega coefficient reliability indicators (i.e., α ≥ .70; ω ≥ .70). The following subscales from the SAEHWS were used for this study:
Job burnout (α = .81; ω = .82) was constructed by a second-order latent variable of its two core components, namely, Exhaustion and Cynicism (Schaufeli & Taris, 2005). This was done to more accurately estimate a latent variable for burnout, as a change in the one component leads to a change in the overall global construct (Shirom & Melamed, 2006). The following subscales were measured by Likert scales: Exhaustion (α = .83) based on 4 items, for example, ‘I feel drained from my work’; Cynicism (α = .76) based on 4 items, for example, ‘I am uncertain whether my work is important’.
Depression (Treatment) was measured by the following item: ‘Are you currently receiving treatment for Depression’, with a yes or no scale (own emphasis) (Yes, I am receiving treatment for this condition; No, I am not suffering from this condition). The framing of the question is important as a participant who felt ‘unsure’ whether he or she suffers from depression would still have to indicate ‘no’ if he or she is not currently receiving treatment. Conversely, if a participant is currently receiving treatment, it is likely due to clinical diagnosis, coupled with medication or other prescribed treatment.
Sleep difficulties were measured on a 4-point intensity scale (Never, Sometimes, Often, Always) with the following item, ‘Over the last 3 months, how often have you experienced sleep difficulties?’ The terminology ‘sleep difficulties’ is used because all participants might not be familiar with the term ‘insomnia’ or perhaps even ‘hypersomnia’, in this way. Therefore, the question is deemed appropriate as participants who experience difficulties with sleep would more accurately self-report general problems with sleep. This is also deemed more appropriate, as a clinical tool for diagnosis of insomnia (or its specific symptoms) could not be used.
Exercise frequency was measured on a 4-point intensity scale (Never, Less than three times per week, Three times or more a week, Everyday) with the following item: ‘Over the last 3 months, how often have you exercised for 20 min or more per day?’
Smoking was measured on a 5-point intensity scale (Never, 5 or less per day, 6–10 per day, 11–20 per day, 20 or more per day) with the following item: ‘How often do you use tobacco products per day?’
Age and Gender were captured by a biographical questionnaire in the first section of the survey, which also included race and language.
Procedure
A survey design was used to achieve the research objective (Shaughnessy, Zechmeister, & Zechmeister, 2003). Individual cross-sectional surveys were conducted at random throughout an organisation from the financial sector. The company specialised in insurance services. The survey was in electronic web-based format, and each participant received a secured link via email with detailed instructions.
Ethical considerations
The research was approved as part of a project by a panel of the North-West University’s faculty for Economic and Management Science’s Research Committee. All ethical guidelines for research with human subjects were adhered to during this study. Anonymity and confidentiality of the participants were assured; transmission of data was encrypted with the American Encryption Standard (AES). Furthermore, no identifying information was shared with any parties during or after the study.
Data analysis
Latent variable modelling via structural equation modelling (SEM) methods was implemented with Mplus 7.11 (Muthén & Muthén, 2013). Mplus possesses the capability to work with a combination of continuous and categorical indicators in the same model. SEM is a powerful statistical technique that allows researchers to specify all the applicable research variables in one model – the input type is the covariance matrix of the data, and therefore, SEM considers the influence (covariance) of all the variables (on one another) at the same time in addressing research questions. The mean and variance-adjusted unweighted least squares method, or abbreviated ULSMV, estimator (Muthén & Muthén, 2013), was chosen for analysis as it has been shown to provide more accurate estimates when compared to the weighted least squares (WLS) in analysing observed categorical data for latent variable purposes when a model converges (Rhemtulla, Brosseau-Liard, & Savalei, 2012). The aforementioned estimators estimate thresholds as opposed to the intercepts that the maximum-likelihood (ML) generates – this is deemed an advantage as it is highly debatable whether the ‘distance’ between a Never and Sometimes, or Sometimes and Often, or Often and Always; options on a categorical scale are equal intervals as is the supposition in ML analysis with continuous indicators.
A polychoric correlation matrix is applied to ordinal data that aims to estimate the correlation between latent variables; Spearman’s rank correlation coefficient has ‘some undesirable properties and the empirical polychoric correlation coefficient is better suited for statistical inference’ (Ekström, 2010, p. 1). Mplus generates a polychoric correlation matrix in the presence of categorical variables and the implementation of the ULSMV estimator. Polychoric correlations have been shown to produce the most accurate results with categorical data, compared to other methods (cf. Holgado-Tello, Chacón-Moscoso, Barbero-García, & Vila-Abad, 2010). Practical significance for correlation coefficients were set at r ≥ .30 (medium effect) and r ≥ .50 (large effect) (Cohen, 1988). Concerning model fit, the following indices were considered: Comparative Fit Index (CFI; acceptable values between .90 and .99), Tucker–Lewis Index (TLI; acceptable values between .90 and .99), and the root mean square error of approximation (RMSEA; acceptable values below .10). (cf. Hu & Bentler, 1998; Muthén, 2009; Muthén & Muthén, 2013; Van de Schoot, Lugtig, & Hox, 2012).
The variables specified as categorical were the observed indicators for burnout (i.e., the exhaustion and cynicism items), gender, sleep difficulty, exercise frequency, smoking, and treatment for depression – leaving age as the only continuous observed variable included in the model. A traditional limitation in working with categorical variables is that independent variables cannot be specified as categorical. Therefore, in order to specify these as exogenous variables, several dummy latent variables were created by constraining the means, variances, and loadings of each of the observed variables. The dummy variables were then validly used as independent indicators in the analysis in order to investigate the structural model’s regression paths.
Results
Results of the SEM analyses showed that the CFI (.984) and TLI (.977) surpassed the rule of thumb of .90 (Hoyle, 1995) and also the more recent suggestion of .95 (cf. Hooper, Coughlan, & Mullen, 2008) for an indication of good model fit. Additionally, the RMSEA value of .023 is below the guideline of .05 and also .10, which confirms good model fit (Browne & Cudeck, 1993).
Table 2 shows the polychoric correlation statistics of the variables from the analysis.
Correlation matrix for the latent variables.
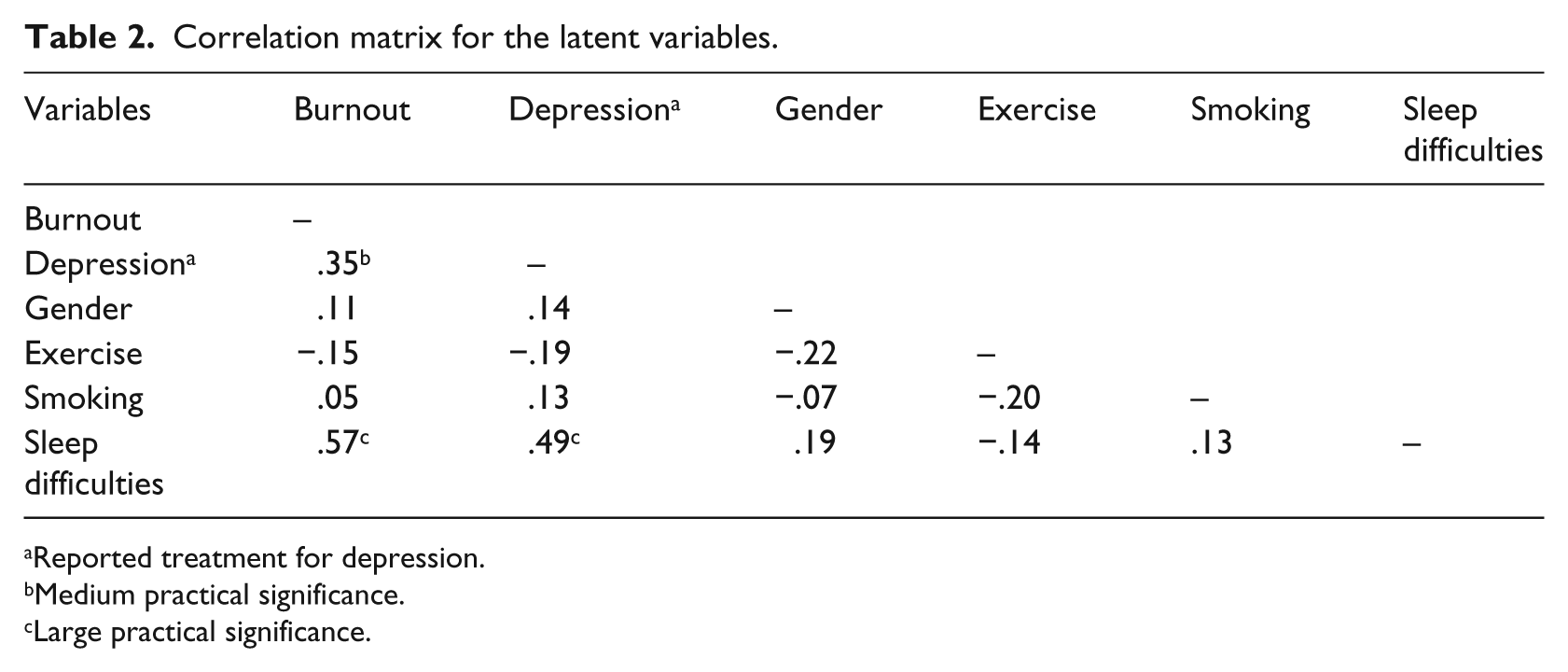
Reported treatment for depression.
Medium practical significance.
Large practical significance.
The polychoric correlation table shows that burnout is correlated with a medium practical significance with treatment for depression. Importantly, burnout also showed a large practically significant correlation with sleep difficulties. Treatment for depression was practically significantly correlated with sleep difficulties with a medium effect (bordering on a large effect).
Figure 1 presents the standardised coefficients of the research model (see Table 3 for detailed output). The squares on the left (depression, gender, exercise, and smoking) represent the observed independent variables and their corresponding counterparts in circles the latent dummy variables constructed as categorical independent variables for the analysis.
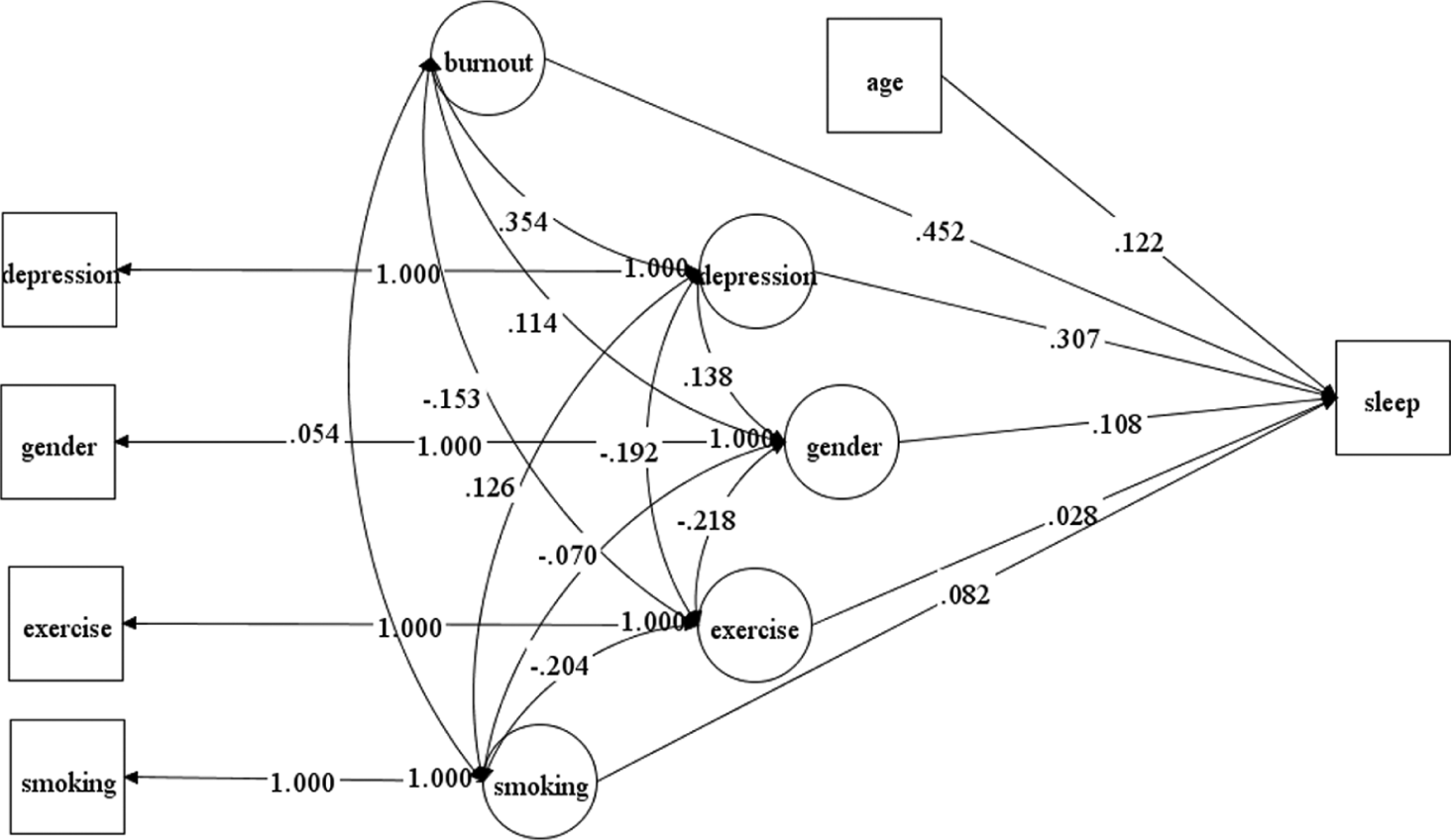
Structural model of the current study with standardised path coefficients.
Standardised estimates for the structural paths.
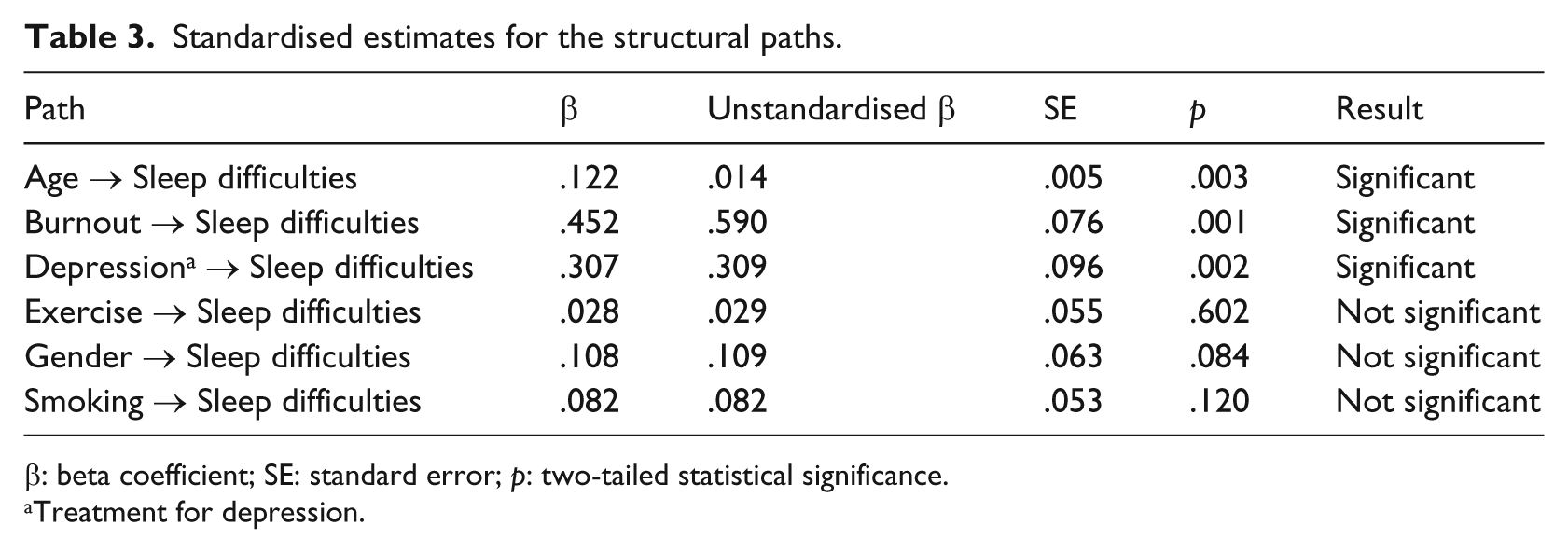
β: beta coefficient; SE: standard error; p: two-tailed statistical significance.
Treatment for depression.
Table 3 presents the results of the structural model with the standardised and non-standardised path coefficients with the statistical significance of each relationship.
Burnout was significantly related to sleep difficulties (β = .452; p < .001), confirming the central hypothesis of this study. Concerning the presence of the other control paths specified for this study, there were only two that were significant: age (β = .122; p < .003) and treatment for depression (β = .307; p < .002). Gender, exercise, and smoking therefore had no significant relationships with sleep difficulties in this sample (p > .05).
Discussion
The aim of this study was to investigate job burnout as a subjective, self-identified occupational phenomenon’s relationship with self-reported sleep difficulties, while controlling for treatment for depression, age, gender, exercise, and smoking behaviour. The central hypothesis was confirmed: burnout had a significant relationship with reporting sleep difficulties even in the presence of all the other variables. This appears to be the first study within the South African context to address job burnout and sleep difficulties and presents a unique approach with the combination of variables. This finding is important as it shows that job burnout is significantly associated with employees reporting sleep difficulties, even when controlling for a combination of factors that have shown to be able to affect sleep. Previous results, albeit in different contexts, are in line with the findings of this study: Ekstedt (2005) suggests that sleep impairment occurs due to an inability to unwind or relax mentally from tension; Armon et al. (2008) found that burnout was associated with insomnia; and Söderström et al. (2004) found that individuals with higher levels of burnout show more arousal from sleep compared to those scoring low on burnout. Therefore, employees who are experiencing increasing sleep difficulties could have a tell-tale sign of the health impairment process at work in them. Research has also found that impaired sleep may also hinder recovery from burnout (Sonnenschein et al., 2007), and that burnout and impaired sleep may adversely affect one another over time (Armon, 2009). Therefore, it is evident that reversed or reciprocal relationships are possible, which implies that impaired sleep may also be a risk factor for burnout, and vice versa – this warrants further investigation, specifically also in the South African context.
Age and treatment for depression were the only other variables, besides burnout, that had a significant positive relational path to sleep difficulty. In practical terms, this indicates that as age increases, so does employee self-reporting of sleep difficulties. Similar results have also been found in previous studies linking age and insomnia-type symptoms (Espiritu, 2008). With regard to treatment for depression, the practical implication of the result is that if an employee indicated that he or she suffers from depression, in the form of receiving treatment for the condition, that reporting sleep difficulties will increase. This is an interesting result as some antidepressant medications have shown a sedative effect but others do not, and that in individuals with insomnia and concomitant depression, sedative/hypnotic medications are often prescribed in conjunction with the antidepressant (Pagel & Parnes, 2001). However, the possibility remains that the employee experienced the sleeping difficulties even before starting the medication; the type of depression medication is also not known, and the possibility of other medications that may complicate the scenario was not investigated. However, what is important within the context of this study is that the influence of treatment for depression has been accounted for in its structural path and that it does not quell the largely significant path of burnout on sleep difficulties. The same applies to gender, exercise, and smoking habits that revealed no significant path relationships to reporting sleeping difficulties in this sample and, for the purposes of this study, should be interpreted as implying that regardless of depression treatment, gender, exercise, and smoking, employees will still report sleep difficulties when experiencing burnout.
This study is not without limitations: A cross-sectional survey design was used and therefore the possibility of common method bias does exist, and causality cannot be confirmed. Furthermore, the number of participants who indicated they were receiving treatment for depression was quite low, and those who indicated that they do not smoke were relatively high. Moreover, no clinical diagnoses were available; it would have been ideal if each participant could have been evaluated and if their medical histories were available. Future studies should seek to address these limitations.
Conclusion
This study provided evidence for the association between job burnout and sleep difficulties in the presence of various control variables. Therefore, it is important that effort-recovery from work be promoted, which should include sufficient and quality sleep, as recovery from burnout has also shown improved sleep continuity (Ekstedt, Söderström, & Åkerstedt, 2009). Relevant practitioners in organisations should also consider and investigate the prevalence of sleep difficulty among employees. This will allow them to focus on informing employees of the importance of quality sleep and how it may affect their work performance and personal stress reaction.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.