
Abstract
The World Health Organization 20-item Self-Reporting Questionnaire is a quick, low-cost screening instrument for measuring common mental disorders and has been applied in community-based health surveys in developing countries. It was originally designed as a general single factor tool for assessing mental distress associated with several common mental disorders. However, studies have also examined alternate multi-factor solutions for the Self-Reporting Questionnaire–20 across diverse study populations. A cross-sectional household survey was conducted in August and September 2009 among adults living in five urban communities in Johannesburg, South Africa (n = 360). The Self-Reporting Questionnaire–20 was used to assess common mental disorders in the past month. Confirmatory factor analysis was applied to compare three competing models (one-, two-, and three-factor models). All three models fit the data well. Gender invariance was tested on the one-factor model based on its extensive application in clinical and research settings. Our findings did not support gender invariance. The differences in factor loadings between male and female subgroups suggest that the application of the Self-Reporting Questionnaire–20 may be more suited to women and therefore should be used cautiously for the assessment of common mental disorders in South Africa urban populations.
Keywords
Introduction
Mental health problems are a major public health concern contributing towards 7.4% of all disability adjusted life years (DALYs) worldwide (Whiteford et al., 2013). In South Africa, neuropsychiatric disorder is the eighth leading cause of healthy lives lost in DALY estimates of 2000 (Norman, Bradshaw, Schneider, Pieterse, & Groenewald, 2006). Common mental disorders are defined as a group of distressed states manifesting with anxiety, depressive, and unexplained somatic symptoms typically encountered in communities and primary health-care settings (Goldberg & Huxley, 1992). In South Africa, a national household survey reported that 30% of adults experienced a Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) disorder in their lifetime, of which 16% and 10% respectively experienced an anxiety and mood disorder (Herman et al., 2009; Stein et al., 2008).
Mental illness has been associated with socioeconomic determinants such as income, employment, and social position (World Health Organization [WHO], 2002). Gender has also been shown to be a critical determinant of mental illness. Depression and anxiety are common comorbid disorders where significant gender differences exist (Linzer et al., 1996). Studies have shown that women have a higher 12-month and lifetime prevalence of depression and anxiety than men in the United States (Kessler et al., 1994) and South Africa (Herman et al., 2009; Stein et al., 2008). The higher prevalence observed in women may be as a result of behavioural differences causing increased diagnoses. For example, women are more likely to report physical and psychological symptoms, such as fatigue and disturbances of appetite and sleep (Kroenke & Spitzer, 1998). Women are also more likely to seek medical help (Spinhoven & Kooiman, 1997). In addition, women are more likely to be exposed to poverty, discrimination, and socioeconomic disadvantage and are therefore more vulnerable to common mental disorders than men (Afifi, 2007). Men, on the other hand, are more likely to develop alternative disorders in response to stress such as antisocial behaviour and alcohol abuse (WHO, 2002).
The Self-Reporting Questionnaire (SRQ-20) was designed by the WHO to assess mental distress associated with several common mental disorders in developing countries (Harding et al., 1980; WHO, 1994). It is a 20-item scale that has been successfully applied in primary health-care and community-based settings and can be self-administered or interviewer-administered. Furthermore, the SRQ-20 is considered to be a relatively cost-effective tool for the evaluation of mental health in adults, especially in developing countries (Harpham et al., 2003; Sartorius & Janca, 1996).
Past studies that explored the internal structure of the SRQ-20 have proposed a number of different factor structures that differ from the original one-factor structure (Chen et al., 2009; Cherian, Peltzer, & Cherian, 1998; Harding et al., 1980; Iacoponi & Mari, 1989; Scholte, Verduin, van Lammeren, Rutayisire, & Kamperman, 2011; Sen, 1987; Ventevogel et al., 2007). Authors have proposed factor structures ranging from two to seven depending on country settings and cultural understanding of the mental health questions included in the SRQ-20. Studies that have demonstrated three or more factor solutions, have consistently described factor structures relating to depressive, anxiety, and/or somatoform symptoms (Chen et al., 2009; Cherian et al., 1998; Iacoponi & Mari, 1989).
To date and to the best of our knowledge, three studies have investigated the internal structure of SRQ-20 by gender (Ghubash, Daradkeh, El-Rufaie, & Abou-Saleh, 2001; Stratton et al., 2013; Ventevogel et al., 2007). Ghubash et al. (2001) applied Receiver Operating Characteristic (ROC) analysis to determine validity indices for the Arabic General Health Questionnaire (AGHQ) as well as the Arabic version of the SRQ-20 in a community survey of United Arab Emirates nationals residing in Al Ain city (Ghubash et al., 2001). The sensitivity, specificity, and area under the curve (AUC) of the AGHQ were 86%, 85%, and 93%, respectively, compared with 83%, 83%, and 90%, respectively for the SRQ-20. The AGHQ had considerably better discrimination between ‘cases’ and ‘non-cases’ than the SRQ-20. The authors reported significant gender differences between the discriminatory ability of both questionnaires.
Ventevogel et al. (2007) similarly compared the Hopkins Symptom Checklist–25 (HSCL-25) with the SRQ-20 in a primary care setting in Afghanistan also using ROC analysis. The SRQ-20 performed moderately in both males and females, with the AUC measuring 74% for men and 73% for women. The authors reported higher cut-off points for the SRQ-20 in women than men (17 for women and 10 for men).
Recently, Stratton et al. (2013) reported on the psychometric properties of the SRQ-20 in a large Vietnamese survey using a latent variable modelling approach. When analysing the effect of gender on the SRQ-20 by measurement invariance tests, the authors reported gender differences on factor loadings and thresholds of a single factor construct (Stratton et al., 2013).
Gender invariance is a statistical property of measurement that demonstrates if the same construct is being measured across men and women and in turn tests whether different groups ascribe the same meanings to scale items (Milfont & Fischer, 2010). Accordingly, without testing the assumption of measurement invariance it remains unclear whether gender differences in common mental disorders are a reflection of true differences, or the product of a different understanding of the mental ill health between men and women in the study population. In addition, the reported discrepancies in the structure of the SRQ-20 warrant further examination of the psychometric properties of the SRQ-20 as it is commonly used in South African settings.
The aim of this study was to investigate the internal validity of the SRQ-20 as a measure of common mental disorders in males and females in Johannesburg, South Africa.
Methods
Participants
This study was conducted in Johannesburg, South Africa, as part of an urban health panel study across five communities, selected based on their different housing characteristics. The Health, Environment and Development (HEAD) study aimed to determine socioeconomic and environmental factors associated with the physical and mental health of adults (older than 18 years) living in different housing types in Johannesburg. The study areas included the following: an inner-city suburb of high-rise blocks of flats characterised by younger and more transient residents; second, a degrading inner-city residential suburb characterised by older and more established residents; third, an Apartheid government housing project characterised by older residents; fourth, an informal settlement characterised by a relatively mobile population; and finally, a post-apartheid government housing project characterised by a relatively established older population. Households were randomly selected from town planning maps for each of study areas. In total, 805 households were identified across five study areas.
The overall response rate in 2009 was low (47%). Interviews were available for 375 individuals; 159 individuals refused to participate and 271 households were non-contactable, that is, either addresses could not be located, or buildings were abandoned, or there were no individuals older than 18 years in the household to be interviewed. A total of 15 (4%) participants were excluded owing to large amounts of missing data.
There were 360 adult participants included in the study across the five study areas; 58% of the participants were female (see Table 1). The mean age of participants was 37.4 (standard deviation [SD]: 14.1) years. Zulu (22%), Afrikaans (20%), and Setswana (14%) were among the most common home languages spoken, with only 8% (29) reportedly having English as their home language. A total of 46% of respondents did not go to school at all or had only completed primary school and 54% were unemployed. A large proportion (81%) of respondents reportedly lived in formal housing. Households with no income or a monthly household income of less than R1000 constituted 39% of respondents.
Socio-demographic characteristics of the study sample.
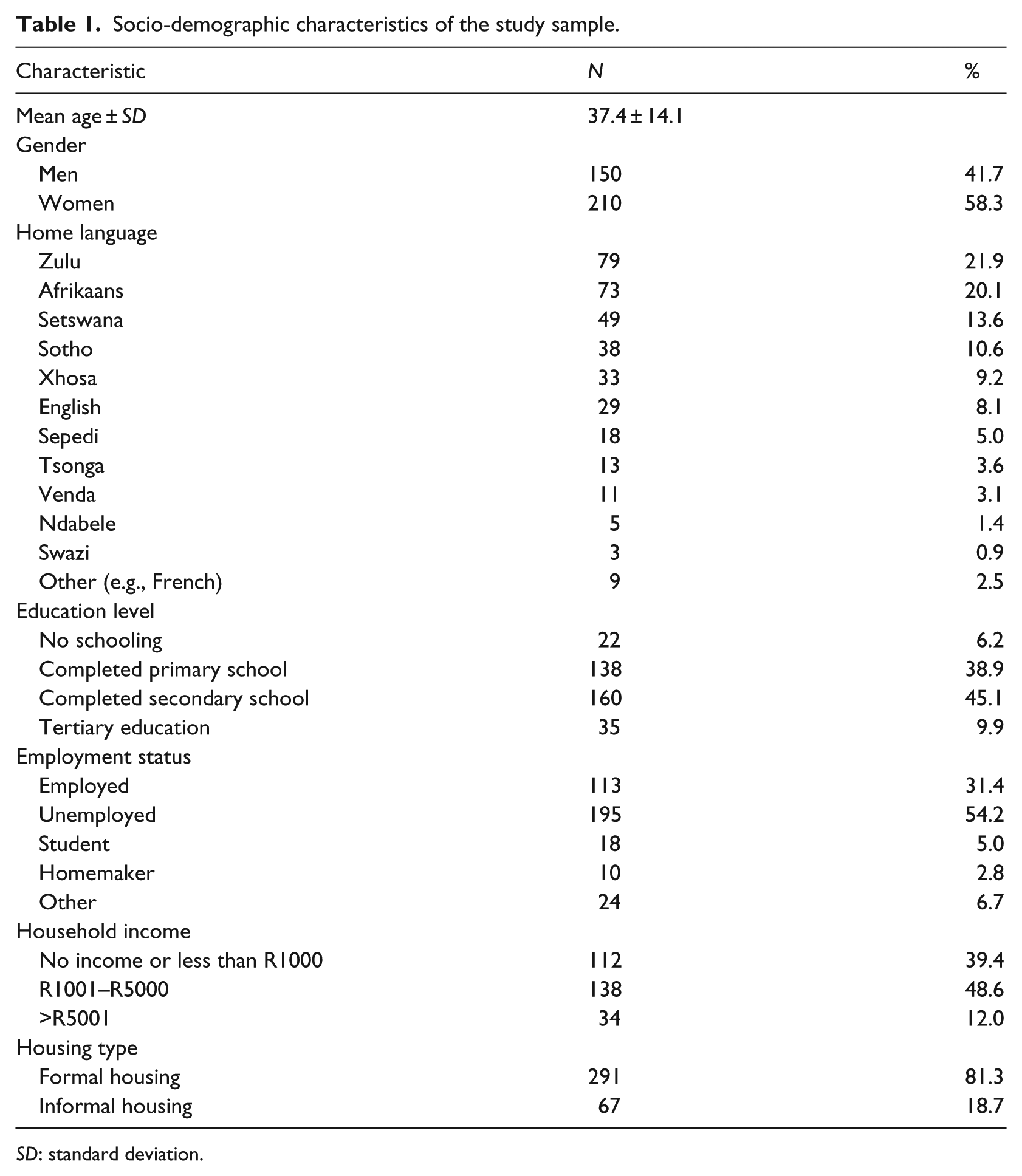
SD: standard deviation.
Instruments
Common mental disorders were assessed using the interviewer-administered WHO 20-item Self-Reporting Questionnaire (WHO, 1994). It consists of 20 yes/no questions, scored 1 or 0, relating to mental health symptoms experienced in the month prior to the interview. Participants scoring 8 or more on the SRQ-20 were classified as a ‘case’ for common mental disorders (Harpham et al., 2003). The SRQ-20 has been translated and validated into at least 20 languages and has been assessed in adolescent and adult populations (Harpham, Huttly, De Silva, & Abramsky, 2005; Harpham et al., 2003; WHO, 1994).
In South Africa, the SRQ-20 has been applied in community-based surveys as a screening tool for common mental disorders (Bhagwanjee, Parekh, Paruk, Petersen, & Subedar, 1998; Rumble, Swartz, Parry, & Zwarenstein, 1996). Internally consistent estimates of the SRQ-20 have been reported across international and African studies, with Cronbach’s alpha values ranging from .81 to .91 (Al-Subaie, Mohammed, & Al-Malik, 1998; Chen et al., 2009; Scholte et al., 2011).
Procedure
Field work took place between August and September 2009. An adult in each household was randomly selected to be interviewed, on the condition that he or she was older than 18 years of age. Interviews were conducted by environmental health students from the University of Johannesburg. The structured questionnaire was interviewer-administered, and questions were orally translated for participants who did not speak English. Prior to the interviews, field workers underwent intensive training, led by a registered psychologist, on questionnaire administration and translation. Households who were not immediately available (owing to circumstances such as work or hospitalisation) were contacted the following month over a weekend.
Ethical considerations
Each participant gave written informed consent prior to commencement of the study. Ethical approval for this study was granted by the Ethics Committee of the University of Witwatersrand, South Africa (Protocol number M10471).
Data analysis
Secondary analysis of data collected in September 2009 was undertaken using STATA Release 12 statistical software (StataCorp, Texas, USA, 2007). Categorical variables were presented as frequencies and percentages. Univariate and multivariate normality was assessed using the Shapiro–Wilk test and Mardia’s (1970) multivariate skewness and Mardia’s multivariate kurtosis respectively. Measure of sampling adequacy was determined using the Kaiser–Meyer–Olkin (KMO) index and Bartlett’s test of sphericity to assess the suitability of a factor solution. The KMO index ranges from 0 to 1, with 1 representing when each variable is perfectly predicted without error by other variables (Kaiser, 1970). A KMO index of greater than .5 and a significant Bartlett’s test of sphericity, that is, p < .05, are necessary to ensure a satisfactory factor analysis (Bartlett, 1954; Kaiser, 1970).
Principal axis extraction method was applied. Oblique rotation was used to facilitate the interpretation of the two- and three-factor models. Factor selection criteria were based on the latent root criterion and the scree test criterion. For each variable, factor loadings of more than .30 were considered significant based on sample size criteria (Hair, Black, Babin, & Anderson, 2010).
Univariate analysis of individual items showed significant non-normality regarding skewness and kurtosis (Shapiro–Wilk test, p < .001) of all items except Item 1. Multivariate non-normality was confirmed by Mardia’s multivariate skewness (β1,p = 191.3, χ2 = 11,582.8, p < .001) and Mardia’s multivariate kurtosis (β2,p = 775.2, χ2 = 11,489.4, p < .001). Diagonally weighted least squares (DWLS) was applied in order to account for the (non-normal) binary distribution of the data (Brown, 2006).
Goodness of fit was assessed using the following five common criteria: (1) low Satorra–Bentler chi-square (SB χ2) with an insignificant p-value (Hair et al., 2010), (2) normed χ2 (the ratio of the chi-square to its degrees of freedom [χ2/df]) of less than 3 (Bollen, 1989), (3) root mean square error of approximation (RMSEA) ⩽ .08 and ⩽ .05 as acceptable and close fit (Kline, 2005), (4) a comparative fit index (CFI), and (5) Tucker–Lewis index (TLI) ⩾ .90 as acceptable fit (Hair et al., 2010).
When comparing models across groups, the hierarchical nested model approach was applied. This approach compared each model to a more restricted version of the same model, that is, configural, weak, strong, and strict factorial invariance (Meredith, 1993). Configural factorial invariance determined whether the factor structure and the items associated with the latent factors were similar across gender and established a baseline against which further constraints could be tested. Weak factorial invariance assessed whether factor loadings were equal across genders, in addition to the configural invariance constraints. Strong factorial invariance tested if the factor loadings and indicator means were equivalent across gender. Strict factorial invariance tested whether factor loadings, indicator means, and error variances were equivalent across gender.
The relative goodness of fit between nested models was tested using the Satorra–Bentler scaled chi-square difference test (ΔSB χ2) where a non-significant ΔSB χ2 test indicated that the models were equivalent across groups. As the ΔSB χ2 test is dependent on sample size and may be susceptible to model complexity (Chueng & Rensvold, 2002), additional criteria of comparative model fit are suggested. These include CFI difference (ΔCFI) between nested models of ⩽.01 and a change in RMSEA of less than .015 which indicated that the more restrictive model is supported (Chen, 2007; Chueng & Rensvold, 2002).
Internal consistency of the SRQ-20 was measured using Cronbach’s alpha coefficient (α), a measure which ranges from 0 (no internal consistency) to 1 (perfect internal consistency) (Hair et al., 2010). High reliability was indicated by Cronbach’s α ⩾ .80 (Hair et al., 2010; Nunnally, 1978).
Results
The proportion of total participants who scored 8+ on the SRQ-20 was 10.4% (see section ‘Instruments’). Women (M = 3.66, SD = 3.73, 95% confidence interval [CI] = [3.15, 4.17]) reported higher mean SRQ-20 scores than men (M = 2.15, SD = 2.76, 95% CI = [1.70, 2.59]) (Table 2). The mean difference in SRQ-20 scores was 1.52 (between 0.81 and 2.22 higher score).
Description of the SRQ-20 by gender.
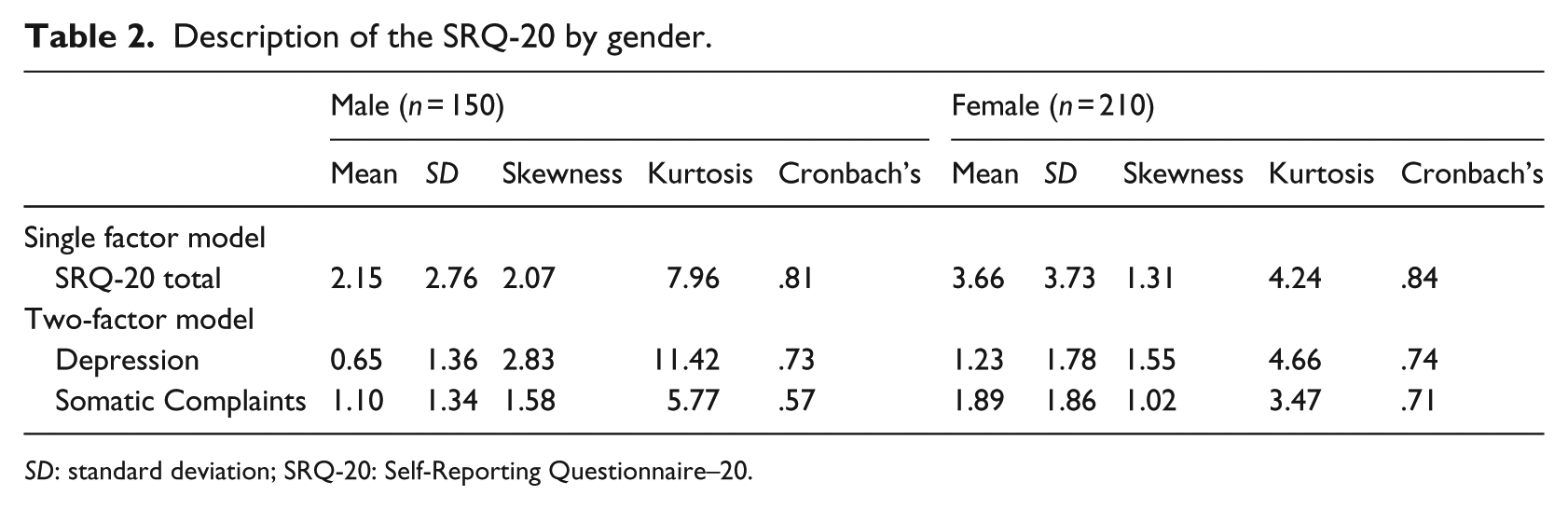
SD: standard deviation; SRQ-20: Self-Reporting Questionnaire–20.
Factor structure of the SRQ-20
The KMO index was .85, indicating that the present data were suitable for factor analysis. The Bartlett test of sphericity was significant (χ2 = 1651.3, p < .001), an additional indication of adequate correlation between variables to continue factor analysis. When applying the latent root criterion, that is, retaining the factors that have an eigenvalue greater than 1.0, one-factor was suggested to best represent the data (eigenvalue of 4.51). Examination of the scree plot suggested a two- and three-factor solution (Figure 1). The subject to item ratio was 18:1. In light of previous analysis of the psychometric properties of the SRQ-20 supporting various multi-dimensional models, three confirmatory factor analysis (CFA) models (the original one-factor, two-factor, and three-factor models) were fit to the data (see Table 3). The first model consisted of a general single factor solution consisting of 20 items with high reliability (Cronbach’s α = .84). Common factoring with principal axis extraction resulted in 74% of variance explained by a single factor.
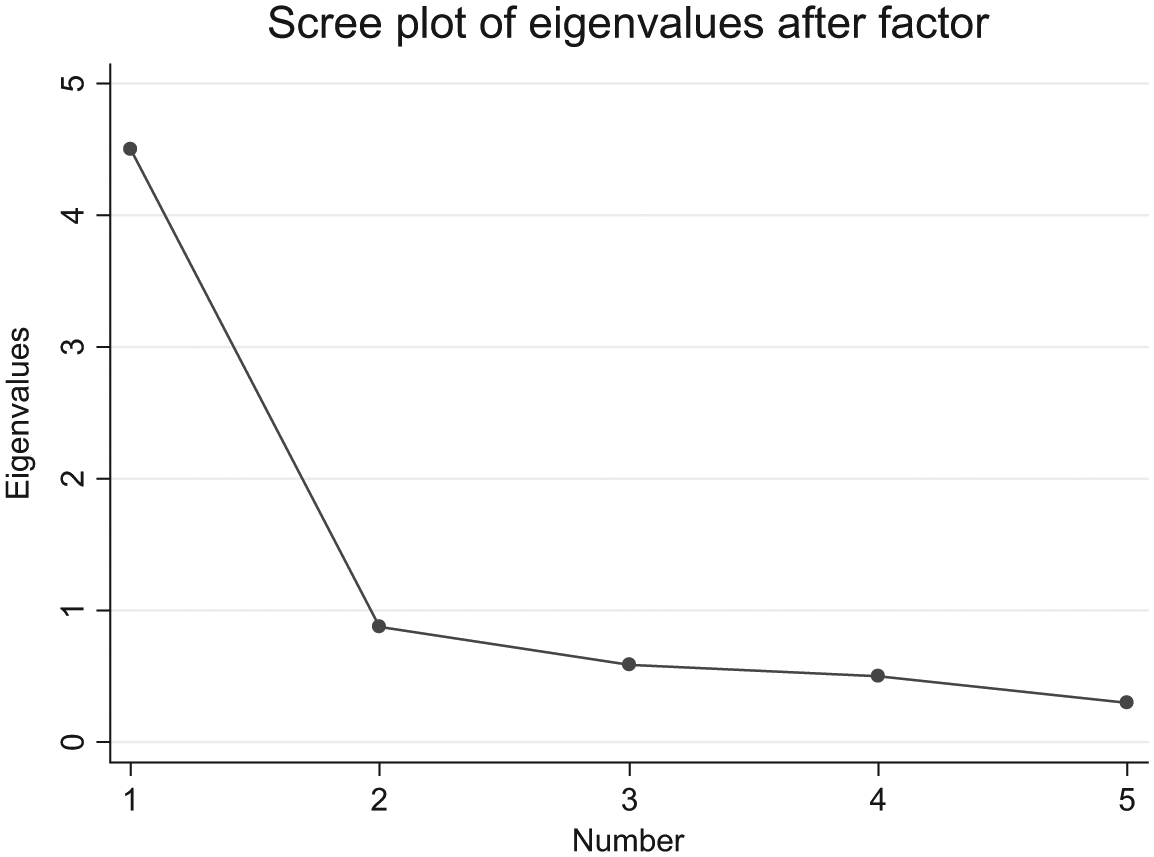
Scree plot of eigenvalues from the SRQ-20 questionnaire.
Factor loadings of the single factor model and the oblique-rotated two-factor model.
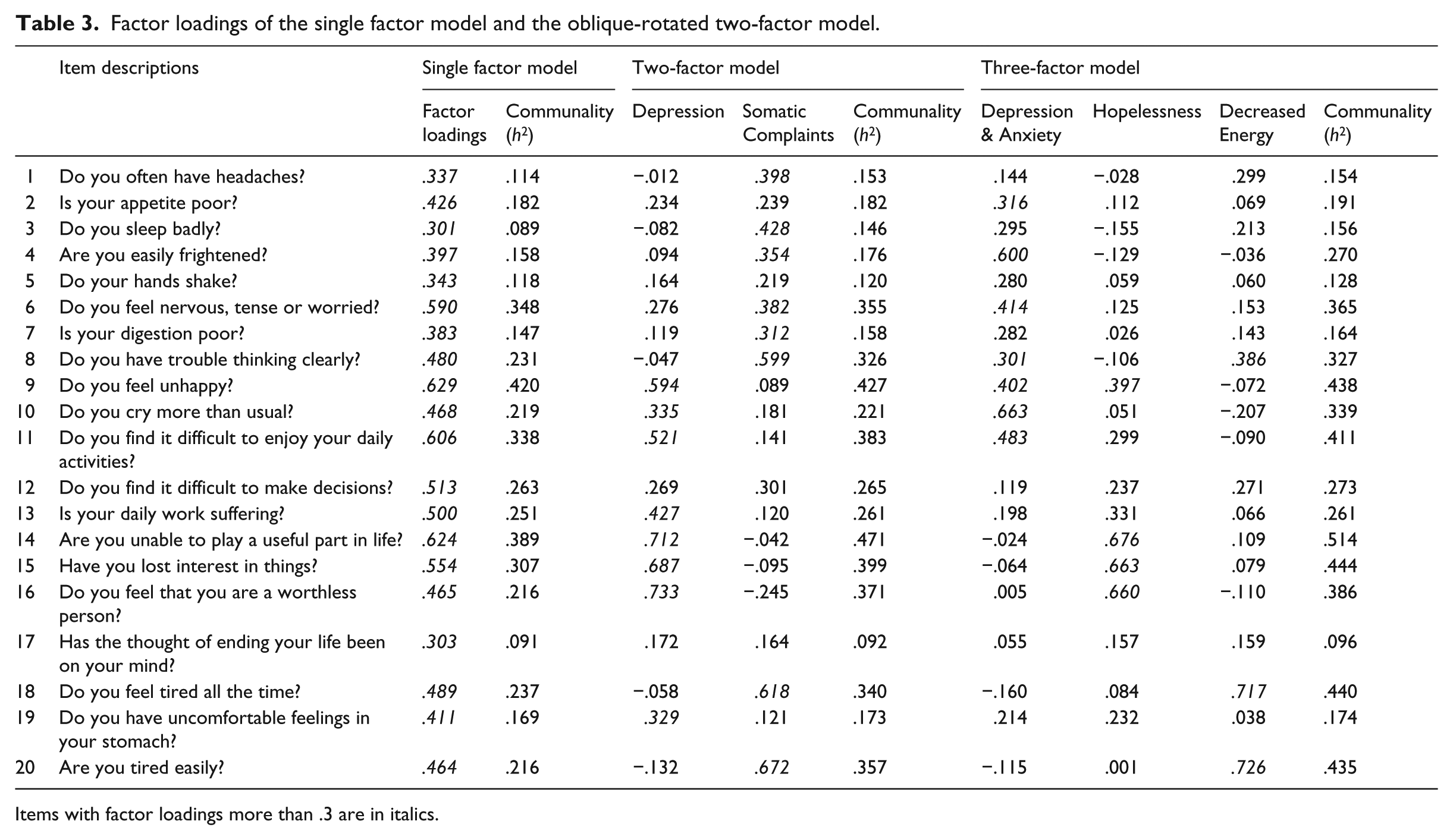
Items with factor loadings more than .3 are in italics.
The second structure was a correlated two-factor solution with interpretable factors: ‘Depression’ and ‘Somatic Complaints’ (see Table 3). The Depression factor was characterised by items assessing unhappiness, crying more than usual, and loss of pleasure in daily activities. The Somatic Complaints factor was represented by items that mostly addressed physical symptoms, that is, headaches, sleeping badly, feeling tired, and poor digestion. There was a moderate correlation between Depression and Somatic Complaints (r = .55). The reliability of the Depression and Somatic Complaints factors was moderate (Cronbach’s α = .73) and low (Cronbach’s α = .57), respectively.
The third structure was a correlated three-factor solution with the following interpretable factors: ‘Depression & Anxiety’, ‘Hopelessness’, and ‘Decreased Energy’. The Depression & Anxiety factor was represented by items assessing feelings of anxiety, unhappiness, and physical symptoms. The Hopelessness factor was characterised by items assessing feelings of worthlessness and loss of interest in things. The Decreased Energy factor consisted of two items relating to tiredness. The three factors were correlated as follows: Depression & Anxiety and Hopelessness, r = .51; Hopelessness and Decreased Energy, r = .37; and Depression & Anxiety with Decreased Energy, r = .34. The reliability of the Depression & Anxiety factor, Hopelessness, and Decreased Energy factor was .64, .71, and .71, respectively.
The validity of the three models was tested using CFA (see Table 4). The three-factor model had an acceptable fit (CFI = .913, TLI = .904, RMSEA = .066 [CI = [.056, .069]]). However, the two-factor model (CFI = .981, TLI = .978, RMSEA = .036 [CI = [.023, .041]]) and the modified single factor model (CFI = .982, TLI = .980, RMSEA = .032 [CI = [.021, .042]]) demonstrated a close fit suggesting that the factors present could be meaningfully interpreted. Given that all three models fit the data reasonably well and are plausible solutions, for the gender invariance testing a single factor solution was chosen based on the SRQ-20’s widespread use as a single 20-item scale both in clinical and research settings.
Confirmatory factor analysis: baseline model fit and comparative fit indices.
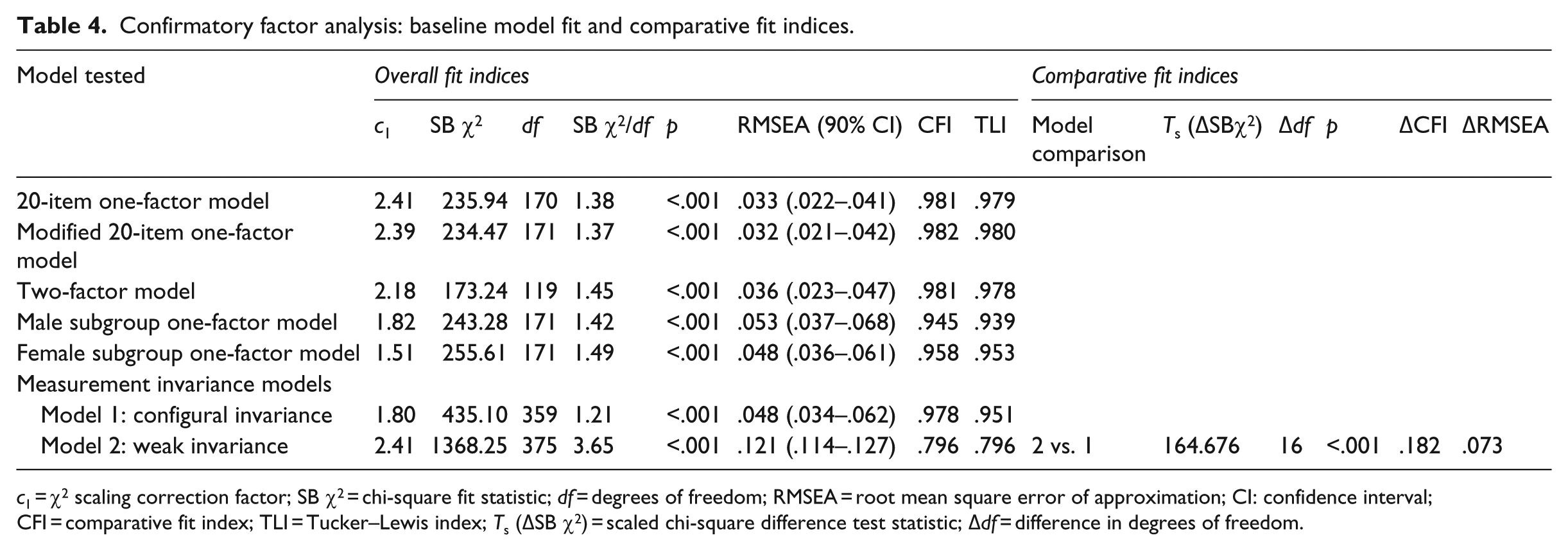
c1 = χ2 scaling correction factor; SB χ2 = chi-square fit statistic; df = degrees of freedom; RMSEA = root mean square error of approximation; CI: confidence interval; CFI = comparative fit index; TLI = Tucker–Lewis index; Ts (ΔSB χ2) = scaled chi-square difference test statistic; Δdf = difference in degrees of freedom.
Modification indices of the single factor solution revealed improved model fit if error variances of two items (always feeling tired and easily tired) were constrained. Good model fit was similarly reported for males (CFI = .945, TLI = .939, RMSEA = .053) and females (CFI = .958, TLI = .953, RMSEA = .048). High reliability was reported for the single factor solution in males (Cronbach’s α = .81) and females (Cronbach’s α = .84).
Multi-group CFA
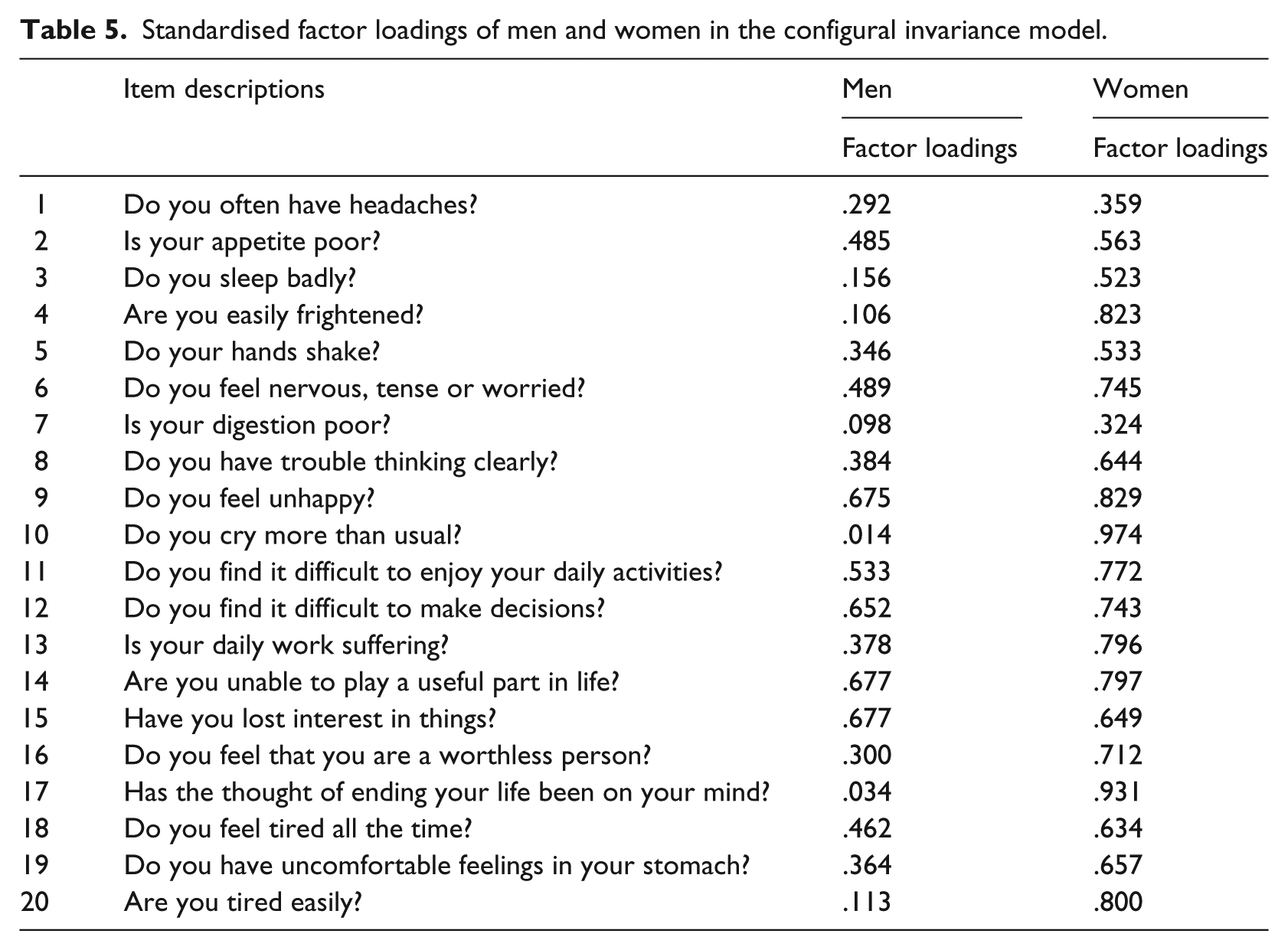
Fit indices of the modified single factor model indicated close fit for the configural model (CFI = .978, TLI = .951, RMSEA = .048) showing that the models for the male and female groups share a common single factor structure and identical item sets across the factor. The p-value of close fit (RMSEA < .05) for the multi-group CFA was .559, suggesting a close fit. Weak measurement invariance (i.e., equality of factor loadings) was not confirmed. The weak measurement invariance model did not fit the data well (CFI = .796, TLI = .796, RMSEA = .121). According to the scaled chi-square difference test, the restricted model showed a significantly worse fit compared to the less restricted configural model (χ2[16] = 164.68, p < .001). As weak invariance was not confirmed, further invariance testing (i.e., strong and strict) will not be reported. Table 5 shows an overview of the factor loadings of men and women in the configural model. Overall, women showed higher factor loadings on the single latent factor compared to men. Higher factor loadings for women were found on Item 10 ‘Do you cry more than usual?’ and Item 17 ‘Has the thought of ending your life been on your mind?’
Standardised factor loadings of men and women in the configural invariance model.
Discussion
This study aimed at testing the factor structure and gender invariance of the SRQ-20, a tool commonly used for the screening of mental disorders, in Johannesburg. A sample of 360 participants was analysed within a multi-group CFA framework.
The proportion of participants reporting distress in our study population was lower than what was previously reported in South African community settings. Rumble et al. (1996) found a weighted psychiatric morbidity prevalence of 27% in a rural community study using the SRQ-20 and the Present State Examination. Similarly, Bhagwanjee et al. (1998) reported a weighted prevalence of generalised anxiety and depressive disorders of 24% in a rural community based on clinical interviews by DSM-IV classification. More recently, Havenaar et al. (Havenaar, Geerlings, Vivian, Collinson, & Robertson, 2007) compared the prevalence of common mental disorders in an urban and rural community using the SRQ-20 and reported high prevalence rates for urban (35%) and rural (27%) settings respectively. However, our findings were in keeping with an earlier urban primary health-care study conducted in Johannesburg, where the authors reported a psychiatric disorder prevalence of 14% (Thom, Zwi, & Reinach, 1993).
Factor structure
At present, there is no consensus on the number of factors reported for the SRQ-20, with factor solutions ranging from 2 to 7 in the literature (Chen et al., 2009; Cherian et al., 1998; Iacoponi & Mari, 1989; Scholte et al., 2011; Sen, 1987; Stratton et al., 2013; Ventevogel et al., 2007). In the current study, all three models provided plausible factor solutions. Our single factor solution, in keeping with the original structure, demonstrated a close fit (Harding et al., 1980). The single factor model was modified by constraining the error terms of two items (always feeling tired and easily tired) further improving model fit. This can be considered reasonable as the two items were similar in wording and content. The modified one-factor solution demonstrated in our study population describes a general psychological distress factor that supports the interpretation of a common dimension for anxiety, depression, and somatic symptoms and may be of value as a screening tool to detect general psychological distress.
Measurement invariance
Our findings did not support gender invariance of the SRQ-20. Thus we can conclude that the SRQ-20 measured different concepts of mental ill health in men and women. These findings are in keeping with previous studies where substantial differences in male and female SRQ-20 scores were demonstrated (Ghubash et al., 2001; Ventevogel et al., 2007). In addition, our findings are in agreement with Stratton et al. (2013) who reported differences in factor loadings and thresholds of the SRQ-20 in Vietnamese men and women.
In the current study, women demonstrated overall higher factor loading values in comparison to men. In particular, women showed higher factor loadings on items relating to depressive symptoms (feeling unhappy, crying more than usual, and thoughts of ending their life), followed by somatic symptoms (poor appetite and sleeping poorly). These factor loading values may indicate that the SRQ-20 is better suited for the screening of common mental disorders in women. In the literature, women have been shown to report more aspecific complaints of distress than men (Mirowsky & Ross, 1995). According to Kroenke and Spitzer (1998), women are also more likely to report physical and psychological symptoms, such as fatigue and disturbances of appetite and sleep, than men (Kroenke & Spitzer, 1998).
In a review by Patel and Kleinman (2003) examining the association between poverty and common mental disorders in low and upper middle income countries, the authors state that consistent risk differences exist across gender for common mental disorders. Desjarlais (1996) postulates that poverty, domestic isolation, powerlessness (resulting from low levels of education and economic dependence), and patriarchal oppression are some of the social determinants associated with higher prevalence of psychiatric morbidity (exclusive of substance disorder) in women. In addition, Kehler (2001) describes that South African women have been struggling to overcome race, class, gender, and resource inequalities all of which possibly contribute to higher levels of distress in women.
Some limitations should be considered when interpreting the results of this study. The SRQ-20 is a screening instrument for measuring common mental disorders and cannot be mistaken as a formal psychiatric diagnosis. The instrument was administered in English, and field workers orally translated the questionnaire when participants could not understand. As a small proportion reported speaking English as their home language, participants may not have understood some symptoms and may have endorsed certain symptoms differently. Failure to address language and/or cultural differences across ethnic groups may have led to misleading conclusions regarding the comparability of the SRQ-20 in the study sample. However, further stratification of the data by language would have resulted in sample sizes too small to result in valid tests of hypotheses. Therefore, future research is needed to examine the relationship of culture and/or language in a larger population.
Conclusion
In conclusion, the study found a low proportion of distress overall in the study population, while women reported higher mean levels of mental distress than men. Gender invariance was not found for the SRQ-20, meaning that men and women in our study population do not perceive mental ill health in the same way. The differences in factor loadings between male and female subgroups suggest that the application of the SRQ-20 may be more suited to women and therefore should be used cautiously for the assessment of common mental disorders in South African urban populations.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.