
Abstract
Compared to patients not receiving treatment, antiretroviral therapy users may experience a lower viral load, an increased CD4 count, slower disease progression, fewer opportunistic infections, and more rapid recovery time from HIV-related illnesses. As such, health-related quality of life is likely to be considerably greater for antiretroviral therapy users than for patients not receiving treatment. The dearth of quality of life research in sub-Saharan Africa brings into focus the need for and importance of documenting the various dimensions of well-being among people living with HIV. We administered the Functional Assessment of HIV Infection to a convenience sample of patients receiving antiretroviral therapy in the Western Cape in South Africa. We used confirmatory factor analysis and exploratory factor analysis to determine the factor structure of the Functional Assessment of HIV Infection. The confirmatory factor analysis revealed a poor model fit of the data. However, the exploratory factor analysis factor structure closely approximated the subscales of the measure, indicating the dimensions of physical, emotional, functional, and social well-being and cognitive functioning. We identified problematic items on the Functional Assessment of HIV Infection contributing to the poor model fit and argue that the measure is potentially useful in assessing quality of life among antiretroviral therapy users in South Africa.
Over the last two decades, the introduction of life-saving antiretroviral medication has meant that living with HIV has changed from a death sentence to a chronic illness (Nischal, Khopkar, & Saple, 2005). Antiretroviral therapy (ART) offers people living with HIV the opportunity of a healthy life for several decades into the future. Compared to patients not receiving treatment, ART users may experience a lower viral load, an increased CD4 count, slower disease progression, fewer opportunistic infections, and more rapid recovery time from HIV-related illnesses (Karim & Karim, 2010). As such, health-related quality of life (HR-QOL) is likely to be greater for ART users than patients not receiving treatment (Jelsma, MacLean, Hughes, Tinise, & Darder, 2005).
HR-QOL is the subjective experience a patient has of the impact of his or her illness on various dimensions of well-being (Cella, McCain, Peterman, Mo, & Wolen, 1996). According to Cella et al. (1996), these dimensions are physical, emotional, functional, and social well-being. These dimensions may be affected by living with HIV, the side effects of ART, or other factors such as HIV-related stigma. Various measures have been developed to assess QOL, including the Medical Outcomes Study Short Form-36 (SF-36) (Ware, Kosinski, & Keller, 1994), the Quality of Well-Being Scale–Self-Administered (QWB-SA) (Kaplan, Anderson, & Ganiats, 1993), and the World Health Organization Quality of Life Measure (WHOQOL) (Hays & Shapiro, 1992). The Functional Assessment of Chronic Illness Therapy (FACIT) system was originally designed for the assessment of QOL among patients diagnosed with various forms of cancer but also used with other chronic illnesses. The Functional Assessment of HIV Infection (FAHI) is one of the FACIT suite of measures and was designed specifically for use among populations seeking treatment for HIV. The measure assesses well-being on the various dimensions delineated by Cella et al., (1996), as well as cognitive functioning.
Clayson et al. (2006) reviewed several HR-QOL measures, including, inter alia, the Health Utilities Index, the Nottingham Health Profile, QWB, and WHOQOL Brief Questionnaire (WHOQOL-BREF). In their review, these authors found that the FAHI and the Medical Outcomes Study–HIV scale were the most appropriate as disease-targeting measures (Clayson et al., 2006, p. 760). Various studies have found the FAHI to be internally consistent (e.g., Cella et al., 1996) and responsive to changes in health status (Abrams, Steinhart, & Frascino, 2000; Peterman, Cella, Mo, & McCain, 1997). Among a sample of HIV-infected patients in two clinical programmes, higher FAHI scores were observed among patients in the earlier stages of the disease and a small association was found between the scale’s total score and CD4 count and viral load (Viala-Danten et al., 2010). Despite a comprehensive search using databases such as PsycINFO, MEDLINE, and PubMed, we found no publications on the use of this instrument in low- and middle-income countries. This is surprising as sub-Saharan Africa is the region where people living with HIV are most concentrated, with prevalence rates among adults estimated at 17.8% in South Africa, 24.8% in Botswana, and 25.9% in Swaziland (Joint United Nations Programme on HIV/AIDS, 2010). The purpose of the study was therefore to report on the performance of the FAHI among South African patients enrolled in a public government-funded ART programme on a QOL measure.
Method
The study was a cross-sectional survey and was part of a larger investigation examining the structural barriers to adherence among ART users.
Participants
We recruited a convenience sample of 291 patients enrolled in the ART programme in the Western Cape in South Africa. Participants received ART services at the Infectious Diseases Clinic of a major public hospital in a peri-urban area outside of Cape Town.
Instruments
HIV-related QOL (FAHI version 4)
The FAHI version 4 is based on the Functional Assessment of Cancer Therapy–General Questionnaire (FACT-G), originally developed for use and validated among cancer patients. Additional items relevant to HIV infection were subsequently added to the FACT-G to yield the FAHI, which then underwent several iterations since its original version. Now in its fourth version, the instrument consists of 47 items that encompass the domains of physical, emotional, functional, social, and cognitive functioning. The FAHI has shown high internal consistency with alpha reliabilities between .73 and .91 on its various subscales. The FAHI has been validated with the Eastern Cooperative Oncology Group Performance Status Rating (ECOG-PSR), the Profile of Mood States (POMS), and HIV disease status as measured by CD4 count (Peterman et al., 1997).
Procedure
Patients were supported by patient advocates (PAs) who were employed by a non-governmental organisation (NGO) operating in the area. The role of the PAs was to encourage medication adherence by visiting patients at home, accompanying them to the clinic, and providing general social support so as to enhance the likelihood of treatment success. For the purpose of this study, PAs were trained to assist with patient recruitment and data collection. Each PA was provided with a flyer describing the study and was asked to inform the patients to whom they were assigned about the opportunity to participate. On agreement from patients, the PAs administered the questionnaire battery to their patients, at the patient’s home, at the clinic, or at the premises of the NGO. The self-report measures were administered in English and Afrikaans.
Patients who agreed to participate in the study signed an informed consent form and completed the questionnaire battery, after which they received a grocery voucher to the value of ZAR20 as a token of appreciation for their participation. PAs similarly received a shopping voucher of ZAR50 (US$6.25) for their assistance with participant recruitment.
Ethical considerations
Ethical clearance was obtained from the Health Research Ethics Committee of the University of Stellenbosch and access to the participants was granted by the Western Cape Department of Health and the City of Cape Town Health Department. We also obtained permission from the NGO and the hospital and clinic administrators.
Data analysis
Descriptive statistics for demographic variables such as age, income, marital status, and educational level were computed to describe the sample. For the psychometric analysis, only the cases with completed data (250 valid cases) were included in the analyses. We performed a confirmatory factor analysis (CFA) on the FAHI items using Mplus Version 6 (Muthén, & Muthén, 1998) to investigate the validity of the FAHI as a measurement model. The specification of the measurement model is based on the assumption that the underlying constructs measured by the subscales of the FAHI are physical well-being (13 items), emotional well-being (10 items), functional well-being (13 items), social well-being (8 items) and cognitive functioning (3 items). Model fit was estimated by using three absolute fit indices (Chi-square; p > .05), namely, the normed Chi-square (ratio 3:1; Hair, Black, Babin, & Anderson, 2010), the root mean square error of approximation (RMSEA < .09, Hu & Bentler, 1999), and two incremental fit indices (comparative fit index [CFI] > .90, Hu & Bentler, 1999; and Tucker–Lewis index [TLI] > .90, Tucker & Lewis, 1973). The absolute fit index is a direct measure of how well the measurement model reproduces the observed data. The incremental fit indices assess how well the estimated model fits relative to the null model that assumes that all observed variables are not correlated (Hair et al., 2010).
To evaluate the convergent validity of the FAHI, we examined the extent to which the items within each subscale converged on a common latent factor. Factor loadings were required to be statistically significant and have a loading of .50 or higher and ideally .70 or higher (Hair et al., 2010). We also calculated the average variance extracted (AVE) and considered values of .50 or higher to be adequate (Hair et al., 2010).
To evaluate the discriminant validity of the FAHI, we compared the AVE estimates for any two subscales with the square of the correlation estimate between those two subscales. The AVE estimate should be greater than the squared correlation estimate for adequate discriminant validity (Hair et al., 2010). We performed an exploratory factor analysis (EFA) to investigate the possibility that some items load substantially (>.40) onto more than one factor.
Results
Demographic characteristics
A total of 291 people living with HIV participated in the study. Demographic data for two participants were missing. The mean age of the sample was 35 years (M = 35.49 years, standard deviation (SD) = 9.05), with a range of 47 years (minimum: 18 years, maximum: 65 years). The sample consisted 186 females (63.9%) and 103 males (35.4%). Approximately 70% were unmarried (69.4%) and 15.8% were married or cohabiting. The rest indicated that they were separated (2.7%), widowed (5.2%), or divorced (1%). Approximately 42% of the sample completed primary school; 44% had attended secondary school but did not complete grade 12; 1.4% had either attended university or college but did not graduate; and 0.3% graduated from a tertiary institution. Almost 60% of the sample stated they were unemployed, while the remaining were employed part-time (21.6%), full-time (8.6%), were students (0.7%), or homemakers (1%). Nearly half the sample (46%) stated that they did not know their annual family income; 0.3% indicated no income; one-quarter reported an income less than ZAR12,000; 4.1% stated their income was between ZAR80,000 and ZAR110,000; and 9.3% indicated their annual family income was ZAR240,000 and above. The majority of participants (59.1%) reported Xhosa as their first language, approximately 22% reported Afrikaans as their first language, and 3.4% of the sample reported English as their first language.
QOL
The results of item-by-item descriptive analyses of the FAHI are presented in Table 1. In order to establish the relative salience of the various FAHI items among members of the sample, we summed the percentages of the sample who endorsed the ‘quite a bit’ and ‘very much’ response options. Using this summation, the most salient aspects of physical well-being that the sample endorsed were lack of energy (63.9%), nausea (67.8%), feeling ill (60.9%), being forced to spend time in bed (75.1%), getting tired easily (57.8%), feeling fatigued (66.8%), and feeling weak all over (61.6%). The most salient aspects of emotional well-being were feeling sad (66.3%), feeling nervous (60.6%), finding it hard to tell others about the infection (39.2), and being embarrassed about the illness (45.4%). In terms of Functional and Global Well-Being, 47.0% of the sample stated they were able to enjoy life and 59.1% stated they had accepted their illness. On the other hand, 57.9% indicated they were losing hope in the fight against the illness. In terms of Social Well-Being, 47% of the sample stated they felt close to their friends, 60.3% stated they received emotional support from their family, 63.9% stated they were satisfied with family communication about their illness, and 65.5% reported that they had people to help them if they needed it. On the other hand, 25.5% stated they were satisfied with their sex life. Cognitive functioning appeared to be a problem for a large percentage of participants as 46.7% and 45.3% stated they had trouble concentrating and remembering things, respectively.
Item analysis of the FAHI.
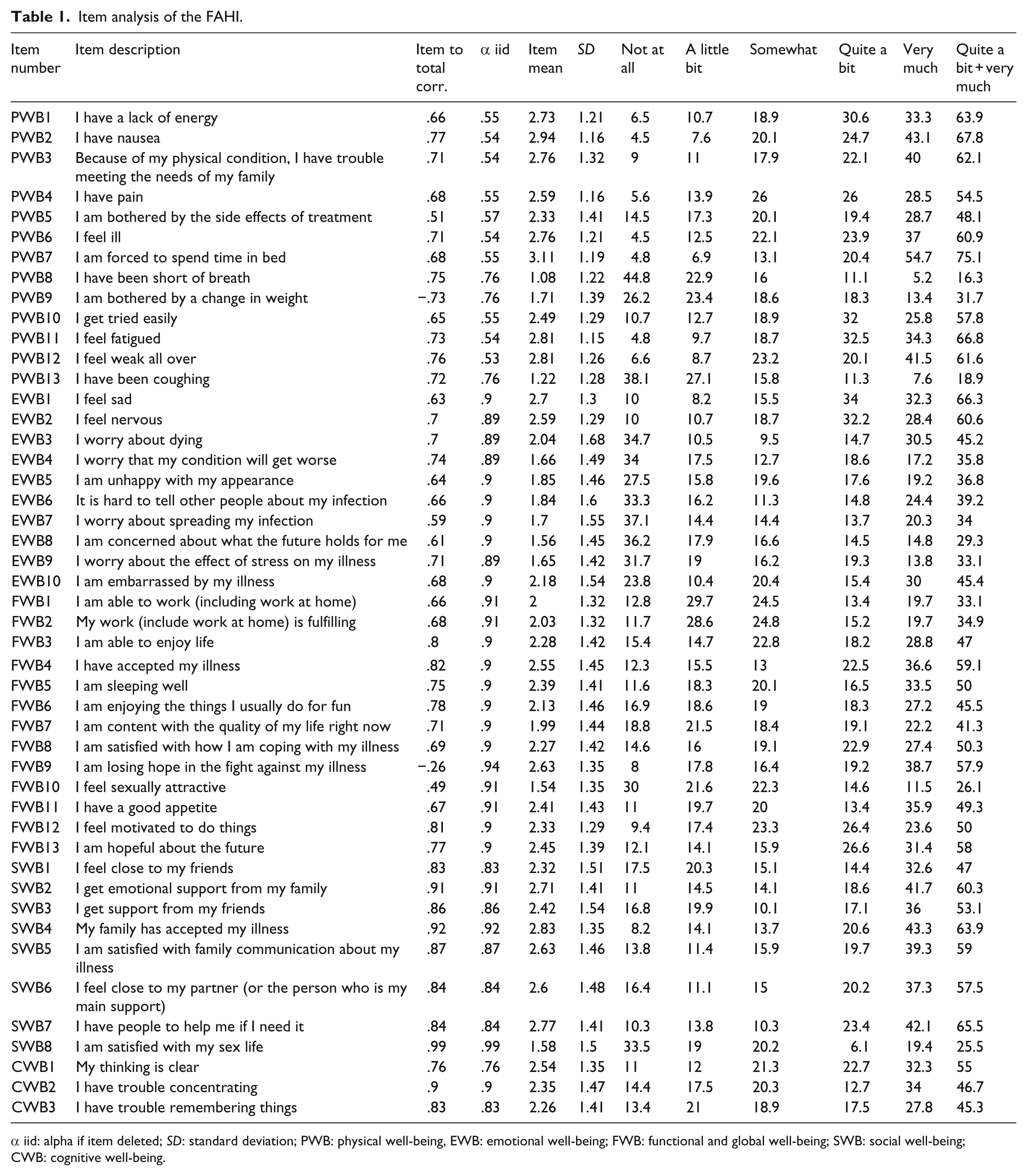
α iid: alpha if item deleted; SD: standard deviation; PWB: physical well-being, EWB: emotional well-being; FWB: functional and global well-being; SWB: social well-being; CWB: cognitive well-being.
In terms of gender, we found non-significant differences in all the dimensions of well-being except for emotional well-being and cognitive functioning. However, these differences disappeared when we corrected for multiple comparisons. We found no other demographic differences in subscale scores. We compared the subscale mean scores of our sample, presented in Table 2, with those obtained in a seminal validation study by Peterman et al. (1997) by means of a series of t-tests. As can be seen in Table 3, our sample means were uniformly significantly lower than those of the comparison sample with the exception of the Emotional Well-Being subscale.
Means, standard deviations (SDs), and Cronbach’s α.
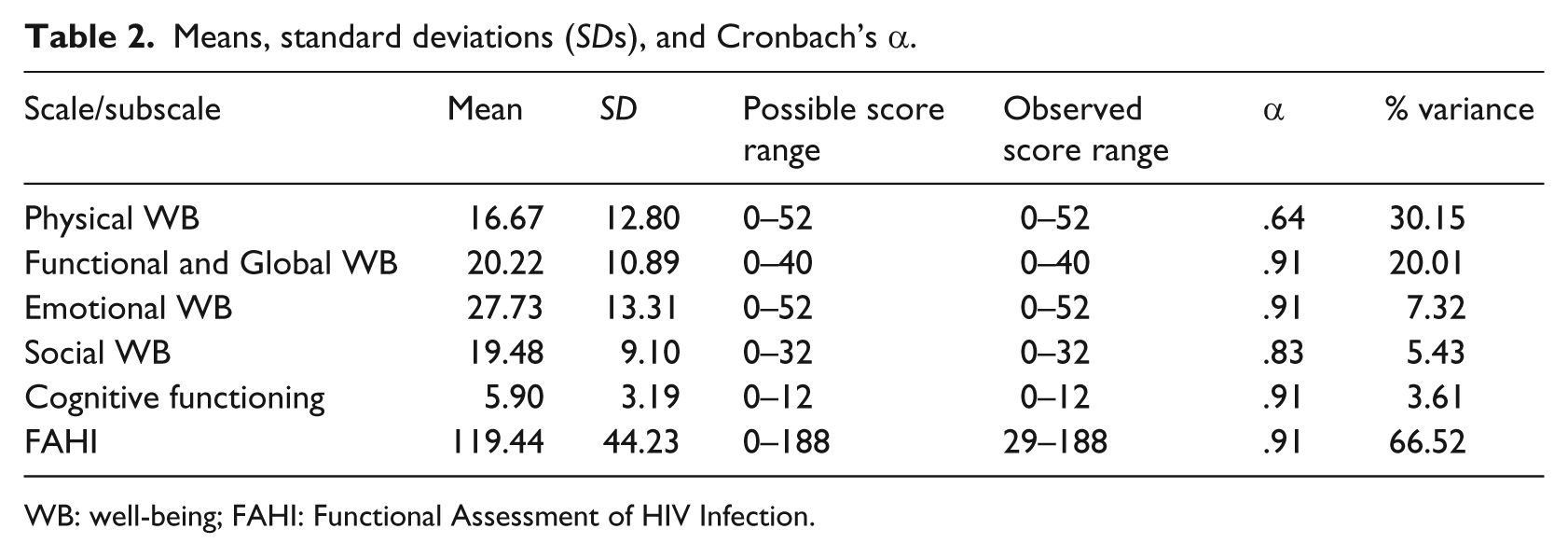
WB: well-being; FAHI: Functional Assessment of HIV Infection.
Results of t-test for difference between the sample subscale means and means obtained by Peterman et al.
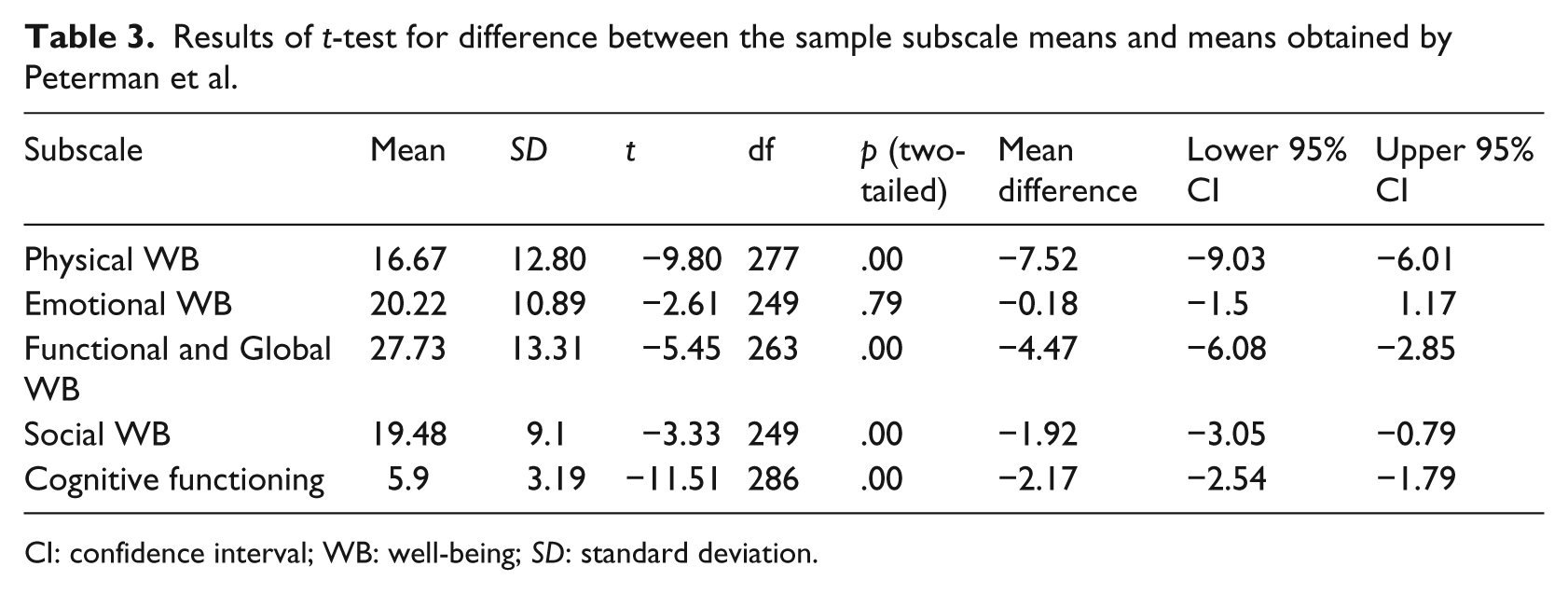
CI: confidence interval; WB: well-being; SD: standard deviation.
CFA
As can be seen from Table 4, all the indices did not reach the criteria for good fit: Chi-square = p < .05, the normed Chi-square ratio = 4:1, RMSEA = .105, CFI = .722, and TLI = .707. In terms of convergent validity, the factor loadings within each subscale were all statistically significant (p < .01).
CFA tests for model fit.
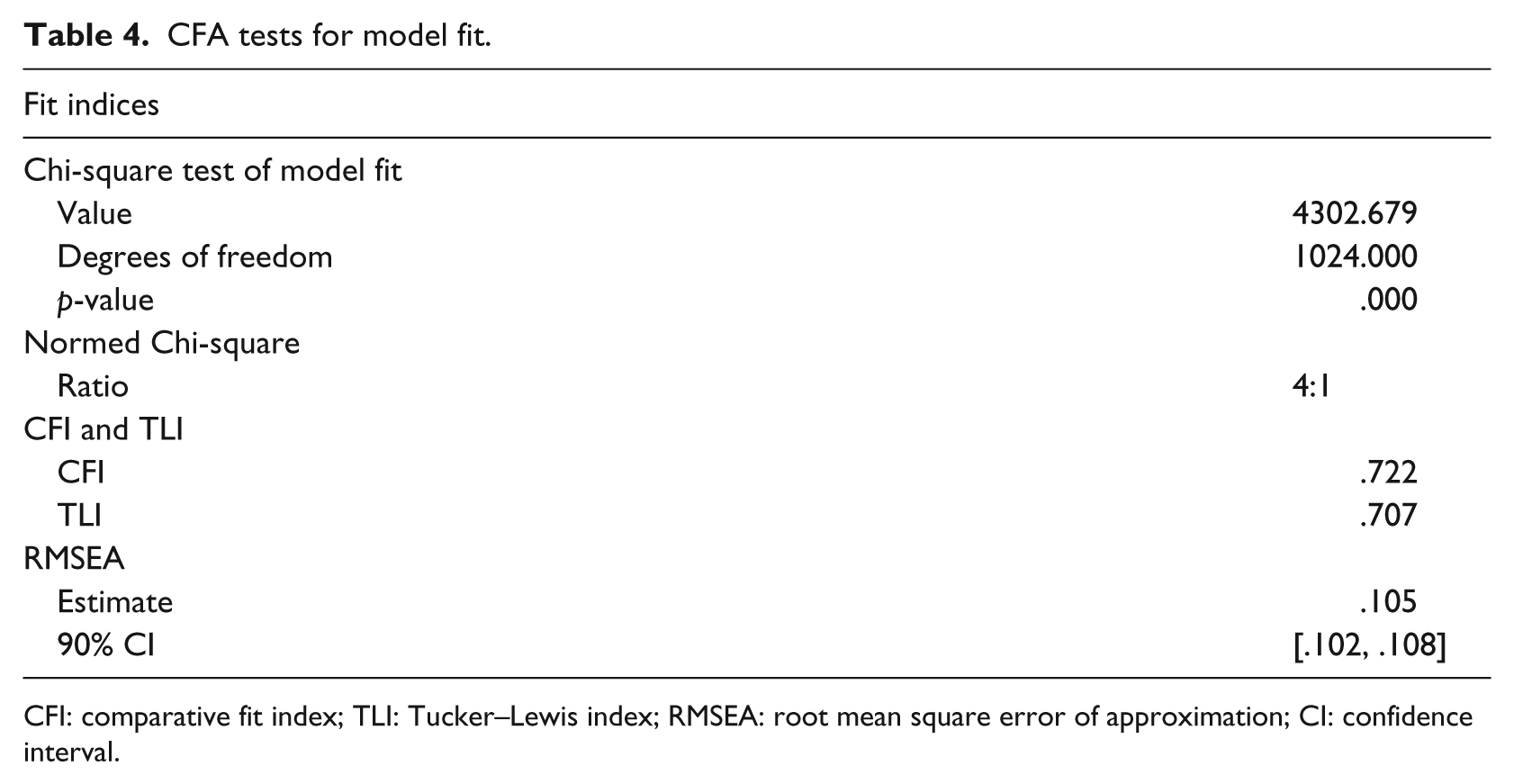
CFI: comparative fit index; TLI: Tucker–Lewis index; RMSEA: root mean square error of approximation; CI: confidence interval.
For physical well-being, the factor loadings ranged from .60 to .90, emotional well-being from .60 to .80, functional well-being from .63 to .85 (except for Items 9 and 10 which had loadings of .21 and .49, respectively), social well-being from .80 to .92 (except for Item 8 with a loading of .19), and cognitive functioning from .80 to .94 (except for Item 1 with a loading of .17) (please see Table 5). The AVE of the subscales ranged from .51 (functional well-being) to .65 (social well-being). Taken together, the evidence supports the convergent validity of the FAHI as a measurement model. In terms of discriminant validity, the AVE estimates for all the subscales were greater than the squared correlation estimates, except for functional well-being which showed an AVE estimate lower than the squared correlation estimate with social well-being (see Tables 5 and 6).
Standardised factor loadings for the CFA, AVE, and reliability coefficients (α).
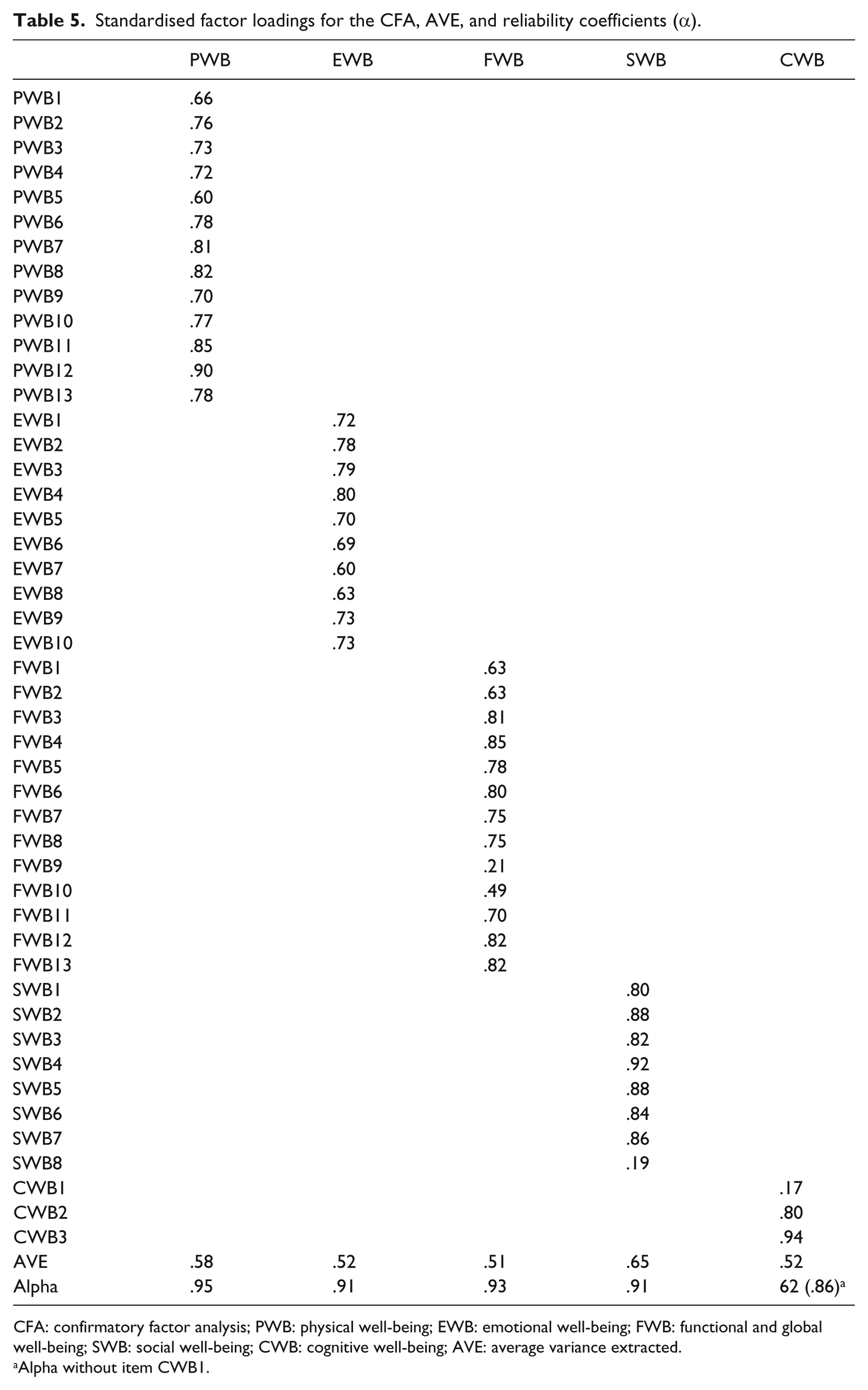
CFA: confirmatory factor analysis; PWB: physical well-being; EWB: emotional well-being; FWB: functional and global well-being; SWB: social well-being; CWB: cognitive well-being; AVE: average variance extracted.
Alpha without item CWB1.
FAHI subscale construct correlation matrix (standardised).
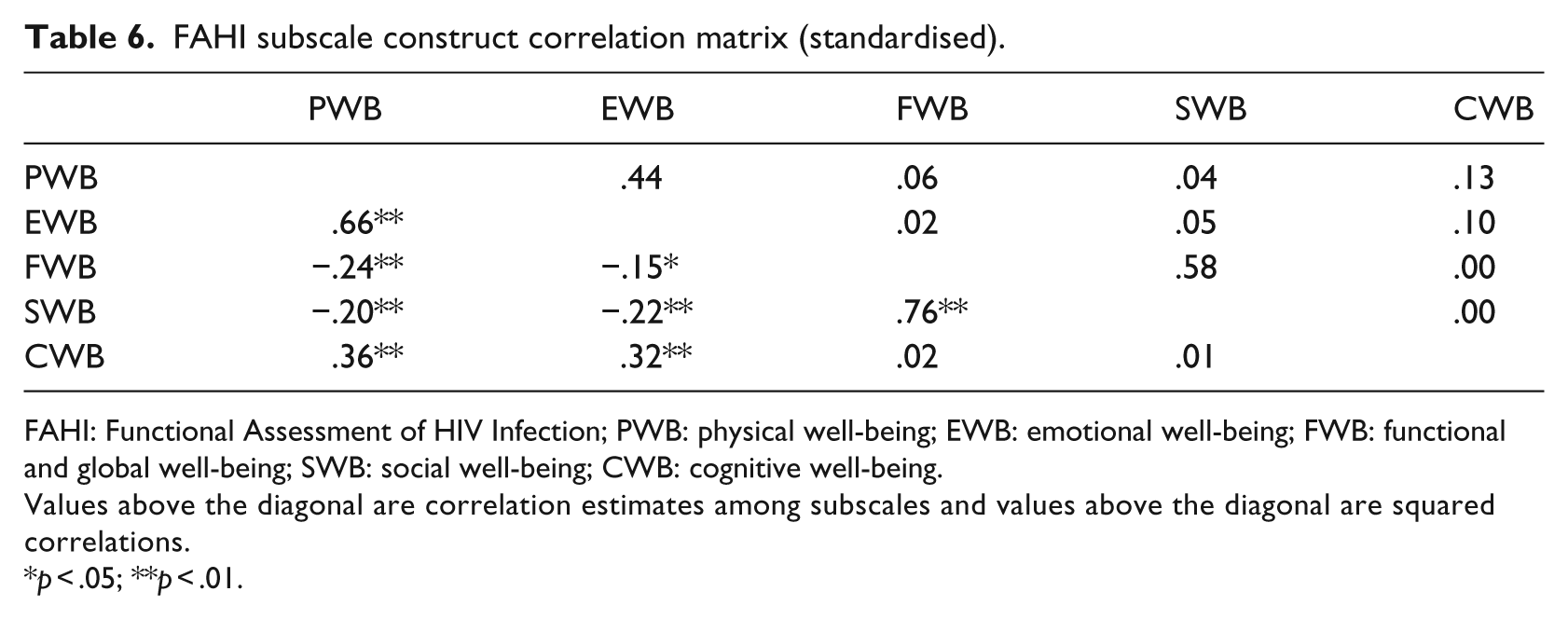
FAHI: Functional Assessment of HIV Infection; PWB: physical well-being; EWB: emotional well-being; FWB: functional and global well-being; SWB: social well-being; CWB: cognitive well-being.
Values above the diagonal are correlation estimates among subscales and values above the diagonal are squared correlations.
p < .05; **p < .01.
EFA
Principal component factor analysis was performed on the FAHI items. The results of the EFA showed that most items loaded substantially onto only one subscale, except for the items forming the functional well-being subscale. As can be seen from Table 7, seven of these items loaded (>.40) onto both the functional well-being and the social well-being subscales. Only one item from the social well-being subscale also loaded onto the functional well-being subscale.
Factor loadings for the EFA.
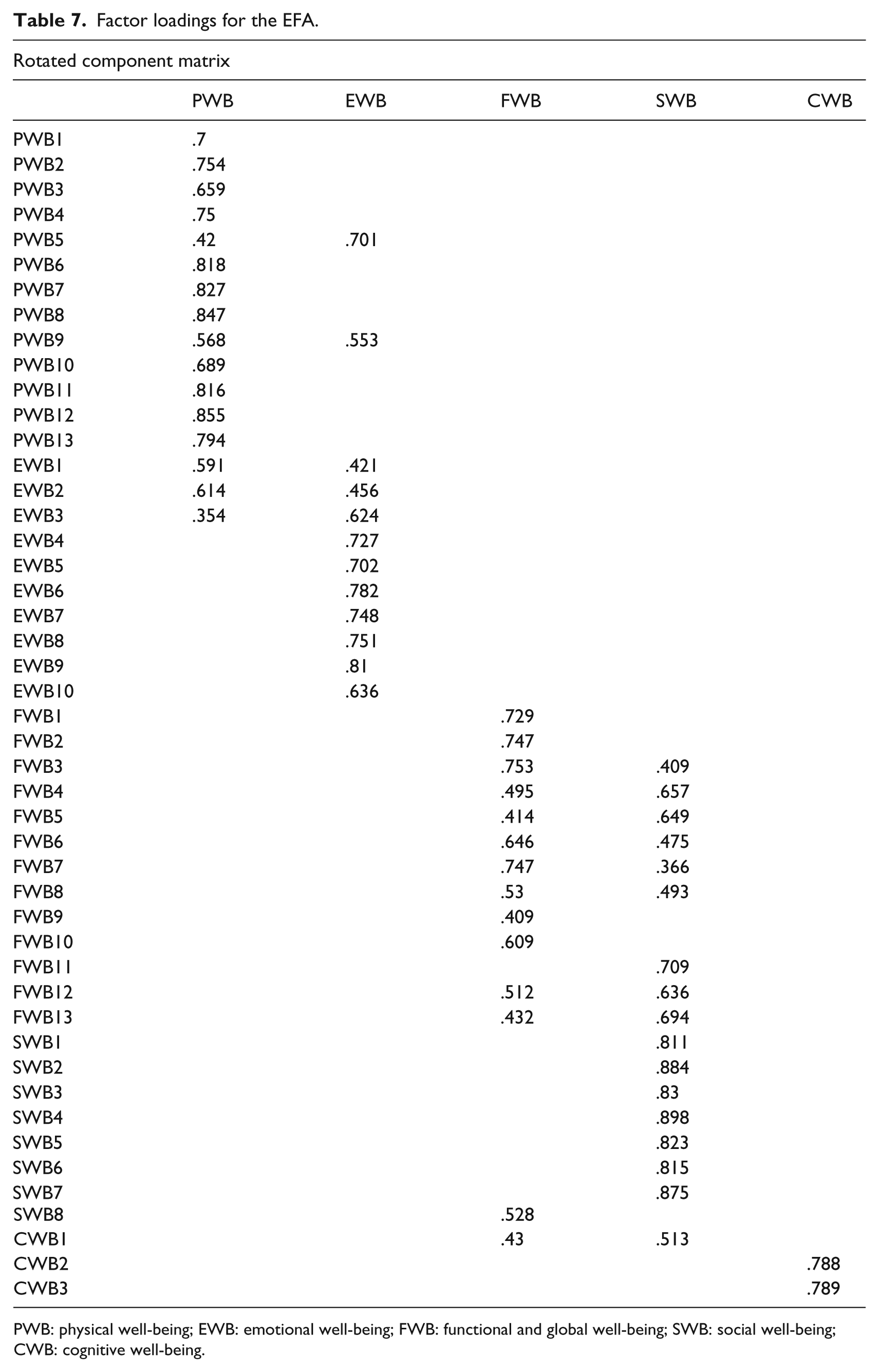
PWB: physical well-being; EWB: emotional well-being; FWB: functional and global well-being; SWB: social well-being; CWB: cognitive well-being.
Discussion
Living with HIV is accompanied by a variety of physical manifestations of the condition, including fatigue, weakness, and low levels of energy. For this reason, it is unsurprising that items reflecting these symptoms were commonly endorsed by the sample. Such symptoms may be common to the physical aspects of living with the virus and the side effects of treatment, as well as elevated levels of psychological distress that have been shown to be common among people living with HIV in resource-constrained contexts. For example, Kagee and Martin (2010), using the Hopkins Symptom Checklist, found that one-third of a sample of South African ART users living with HIV reported feeling low in energy, while 35% stated that they felt everything was an effort. The potential overlap of physical and psychological symptoms is a matter for further investigation.
In terms of emotional well-being, the most commonly endorsed FAHI items were feeling sad and nervous, which approximated symptoms of depression and anxiety. While major depression and generalised anxiety have been shown to affect only a minority of people living with HIV (11.1% and 0.4%, respectively) (Freeman, Nkomo, Kafaar, & Kelly, 2007), non-psychiatric distress has been shown to be common among South Africans living with HIV, including symptoms such as worrying too much about things, feeling tense, feeling hopeless, and feeling worthless (Kagee & Martin, 2010).
Of the sample in this study, almost 40% found it difficult to tell others, such as loved ones, work colleagues, and friends, that they were living with HIV, and nearly half reported being embarrassed about their illness. This is hardly surprising, given the level of stigmatisation associated with being HIV positive (Kalichman & Simbayi, 2004). Stigma associated with HIV has been found to be one of the most salient barriers to adherence to ART (Coetzee, Kagee, & Vermeulen, 2011). Coetzee et al. (2011) found that many participants in their sample of ART users reported being unwilling to attend clinic appointments because they could not inform their employers of their need to do so. Several also reported the need to hide their medication from others, thus reducing the likelihood of pill-taking adherence. To this extent, HIV stigma, while compromising QOL at a general level as reflected by endorsement of the relevant FAHI items, also influences health outcomes by means of compromising ART adherence.
Despite the concerns surrounding stigma, participants reported surprisingly high levels of social support. Nearly half of the sample stated they felt close to their friends, and nearly two-thirds reported that they were satisfied with family communication about their illness and that they had people to help them if necessary. These data are encouraging and bring into focus the importance of social capital (Campbell, 2003), that is, a strong sense of connectedness within communities that play a role in the way people experience their illness condition.
The fact that close to half the sample reported having trouble concentrating and remembering things is in keeping with recent literature calling attention to neurocognitive problems among people living with HIV, although the causal trajectory of such problems is unclear (Becker, Thames, Woo, Castellon, & Hinkin, 2011). For example, non-adherence may lead to AIDS-related health problems, including neuropsychological deficits. Deficits such as forgetfulness and concentration difficulties may lead to poor adherence to pill-taking and clinic attendance, which in turn may impact HR-QOL. The high alpha coefficients for each subscale indicate that the measure has good internal consistency for these dimensions of HR-QOL.
The results of the CFA indicated a poor model fit with the data, indicating that the factor structure of the FAHI had limited applicability among our sample. On the basis of the discriminant validity analysis, the subscales were found to be different from one another. However, there was considerable overlap between the subscales of social and functional well-being. EFA showed that seven items on the functional well-being subscale also loaded on the social well-being subscale. The overlapping items were as follows: ‘I am able to enjoy life’, ‘I have accepted my illness’, ‘I am sleeping well’, ‘I am enjoying the things I usually do for fun’, ‘I am satisfied with how I am coping with my illness’, ‘I feel motivated to do things’, and ‘I am hopeful about the future’. On the basis of these findings, it may be argued that the items on the social and functional well-being scales were interpreted similarly among our sample. The high convergent validity of the items suggested that the items within each subscale converged on a common latent factor. There were, however, cross-loadings between the functional well-being and social well-being subscales.
The data indicate that the FAHI is a useful HR-QOL measure for use among clinical and research populations in the Western Cape. One of the limitations of the study was that we recruited a sample from only one region. As a society characterised by cultural, racial, and linguistic diversity, research on translated versions of the FAHI into local indigenous South African languages, such as Sotho, Zulu, and Xhosa, is necessary. This study did not examine data relating to the duration of the participants’ ART, which is an obvious limitation to the study.
Conclusion
This study has shown the utility of the FAHI among a sample of South African ART users. In keeping with its usefulness in other samples around the world, the FAHI has displayed good psychometric properties that make its use appropriate for South Africans living with HIV. The items have high relevance for ART users in the context of their illness, the side effects of treatment, and the level of stigmatisation associated with living with HIV.
Footnotes
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.