
Abstract
Students, especially women, are in the highest HIV incidence group in Sub-Saharan Africa. Willingness to participate is a crucial element in recruitment of participants for clinical trials, including HIV prevention trials. There is increasing incidence of HIV among university students, highlighting the importance of evaluating their willingness to participate in prevention trials. Assessment of willingness to participate assists in determining community preparedness for trials. This cross-sectional study aimed to evaluate willingness to participate and explore racial differences and factors associated with willingness to participate in HIV prevention research. The Clinical Research Involvement Scale and demographic questionnaire were administered online to university students aged 18–45 years at the University of KwaZulu-Natal in South Africa. The instruments evaluated associations between willingness to participate and age, gender, relationship status, parity, religion, education, student and employment status, and access to private health care. This study enrolled 636 participants, of which 509 records were analysable. Most students were willing to participate in HIV prevention research irrespective of race. However, Black students expressed greater intention to participate compared to White and Indian students. Racial differences in factors that affect intentions to participate were differences in risk perception and seeking access to better quality health care. The Clinical Research Involvement Scale is a reliable instrument in this population. Validity improved with removal of factors, motivation to comply, and outcome evaluations. These findings may not be generalizable to other student populations in Southern Africa.
Keywords
South Africa’s HIV epidemic is defined by The Joint United Nations Programme on HIV/AIDS (UNAIDS, 2008) as hyper-endemic since over 15% of 15- to 49-year-olds are infected, with HIV prevalence among 15- to 24-year-olds among the highest globally at 8.5% in 2013 (Statistics South Africa, 2013). In South Africa, all race groups are at risk of HIV infection, particularly youth, highlighting the urgency of developing effective HIV prevention strategies (Bekker & Gray, 2017; Harrison, Newell, Imrie, & Hoddinott, 2010) to combat the pandemic (Terry, Gallois, & McCamish, 1993). The target population for HIV prevention clinical studies include men or women aged between 18 and 45 years (de Oliveira et al., 2016). However, recruitment of individuals to participate in medical research remains a challenge (Trauth, Musa, Siminoff, Jewell, & Ricci, 2000). HIV prevention trials usually recruit high-risk individuals such as sex workers and drug users (Oguntibeju, Esterhuyse, & Truter, 2009). However, HIV infection in university students is increasing (Oguntibeju et al., 2009). The SAVVY vaginal gel (C31G) trial in Nigeria to prevent HIV infection reported that approximately 35% of the participants were students (Shisana et al., 2009). In the South African CAPRISA 004 microbicide trial to prevent HIV infection, 19.4% of the participants had some tertiary education. University students engage in high-risk sexual behaviour such as inconsistent condom use, drug and alcohol abuse, and multiple sexual partners (Abdool Karim et al., 2010; Abdool Karim et al., 2011; Oguntibeju et al., 2009). The Higher Education HIV/AIDS Programme (HEAIDS, 2010) survey on HIV and AIDS and related factors at University of KwaZulu-Natal (UKZN) in 2008 revealed an HIV prevalence of 1.1% among 18- to 24-year-olds and 15.1% among 25- to 34-year-olds, illustrating high levels of HIV risk among students. Although the majority of students at risk will never become infected, disease prevention in this group should remain a public health priority (Oguntibeju et al., 2009). University students are the next generation of leadership and the impact of HIV on students will have both health and economic consequences (Abdool Karim et al., 2011). Barriers to participation in HIV prevention research include concerns about personal safety, fear, mistrust, misunderstanding about study design, social risk, and pragmatic obstacles (Mills et al., 2004). A report from a World Health Organization (WHO)-UNAIDS consultation on HIV vaccine trials suggests that willingness to participate (WTP) varies with age, educational level, and perceived risk (Suhadev, Nyamathi, Swaminathan, Suresh, & Venkatesan, 2009).
In South Africa, HIV is perceived by some as a ‘black disease’, in part due to media portrayal of AIDS as a young Black female epidemic (Stadler, Delany, & Mntambo, 2008), supporting the misperception of low perceived risk in other race groups. Race is a complex issue and may be a proxy for a range of social and cultural factors including knowledge, information, and beliefs about HIV/AIDS-related stigma and discrimination (Anderson, Beutel, & Maughan-Brown, 2007). Racial differences in WTP have been widely researched in the United States (Shavers, Lynch, & Burmeister, 2002) but not in South Africa (Barsdorf & Wassenaar, 2005). Barsdorf and Wassenaar (2005) found that Black South Africans scored lower on perceived voluntariness in medical research compared to Whites and Indians, possibly owing to negative perceptions of medical research from the Apartheid regime or health service inequality based on race. A study conducted by Smit et al. (2006) assessing WTP in HIV vaccine research in a settlement outside Cape Town found that there was a low (23%) overall WTP that was associated with male gender, increasing age, and knowledge about vaccines.
Frew et al. (2010) developed the Clinical Research Involvement Scale (CRIS) using constructs from the theory of reasoned action (TRA) to understand factors driving participation in HIV vaccine trials. The TRA is a behavioural theory by Fishbein and Ajzen (1975) that explains volitional behaviour. Volitional behaviour is the act of making a conscious choice or decision. TRA proposes that the strongest predictor of voluntary behaviour is one’s behavioural intention to perform a particular behaviour. The TRA in general focuses on determinants of a single behaviour (Sheppard, Hartwick, & Warshaw, 1988). The model was specifically developed to assess behaviours that are under a person’s volitional control rather than outcomes that result from that behaviour. A meta-analysis by Sheppard et al. (1988) highlighted that attitudes and subjective norms as denoted in the TRA were a very good predictor of individuals’ intentions to perform certain behaviours. Furthermore, a study by Bosompra (2001) used the TRA to assist in understanding the beliefs that underlie Ghanaian university students’ attitudes, subjective norms, and intentions about the consistent use of condoms. Bosompra found that students who believed that advantages of using condoms were greater than the disadvantages were more likely to have intentions of using condoms. In addition, students who believed that significant individuals thought that people who are sexually active should use condoms were more likely to intend to use condoms. These findings support previous studies and confirmed that both subjective norms and attitudes are determinants of behaviour intention (BI; Bosompra, 2001). This opposes the argument that behavioural theories are ‘Western Models’ and do not apply to other cultures (Fishbein & Ajzen, 1975). In addition, Sheppard et al. (1988) found that the TRA model showed strong predictive utility even when used under conditions not originally specified for the model.
The TRA has been applied to many health-care behaviours and is a useful conceptual approach for understanding and promoting HIV prevention behaviours (Fisher, Fisher, & Rye, 1995) such as safe sex behaviour and condom usage (Frew, Archibald, Martinez, del Rio, & Mulligan, 2007). It has guided the development of effective behavioural HIV risk reduction interventions through behavioural prediction models (Kalichman, Carey, & Johnson, 1996).
Because KwaZulu-Natal is the epicentre of South Africa’s HIV epidemic (Abdool Karim et al., 2011), the aim of this study was to determine racial differences in WTP in HIV prevention trials among university students in KwaZulu-Natal using the CRIS.
Methods
Participants
An observational, analytic, cross-sectional study was conducted among university students at UKZN. Participants were 636 students comprising 507 Blacks, 52 Whites, 55 Indians, 8 Coloured, 1 and 14 Other (non-South African students). Race categories included were South African census/Statistics South Africa (2013) defined race groups of Black, White, Indian, and Coloured. Race is not used here as a proxy for culture. Students who accessed the survey and did not provide consent, students who did not provide race information on the survey, non-South African citizens (‘Other’ defined race group), and participants who skipped more than three questions were excluded from the analysis to yield a sample size of 509 as shown in Figure 1. Since the primary objective was to assess racial differences, responses not providing race information were excluded. Non-South African citizen students were excluded as it was assumed that they could have different perceptions of HIV prevention due to socialization in different social structures and epidemiological settings from South Africa. Students who skipped more than three questions were excluded due to missing essential data which would affect the eventual scoring of the scale. Coloured students were included in the analysis but due to the small sample size (n < 10, all female), meaningful conclusions could not be drawn from this group, hence were not reported on.
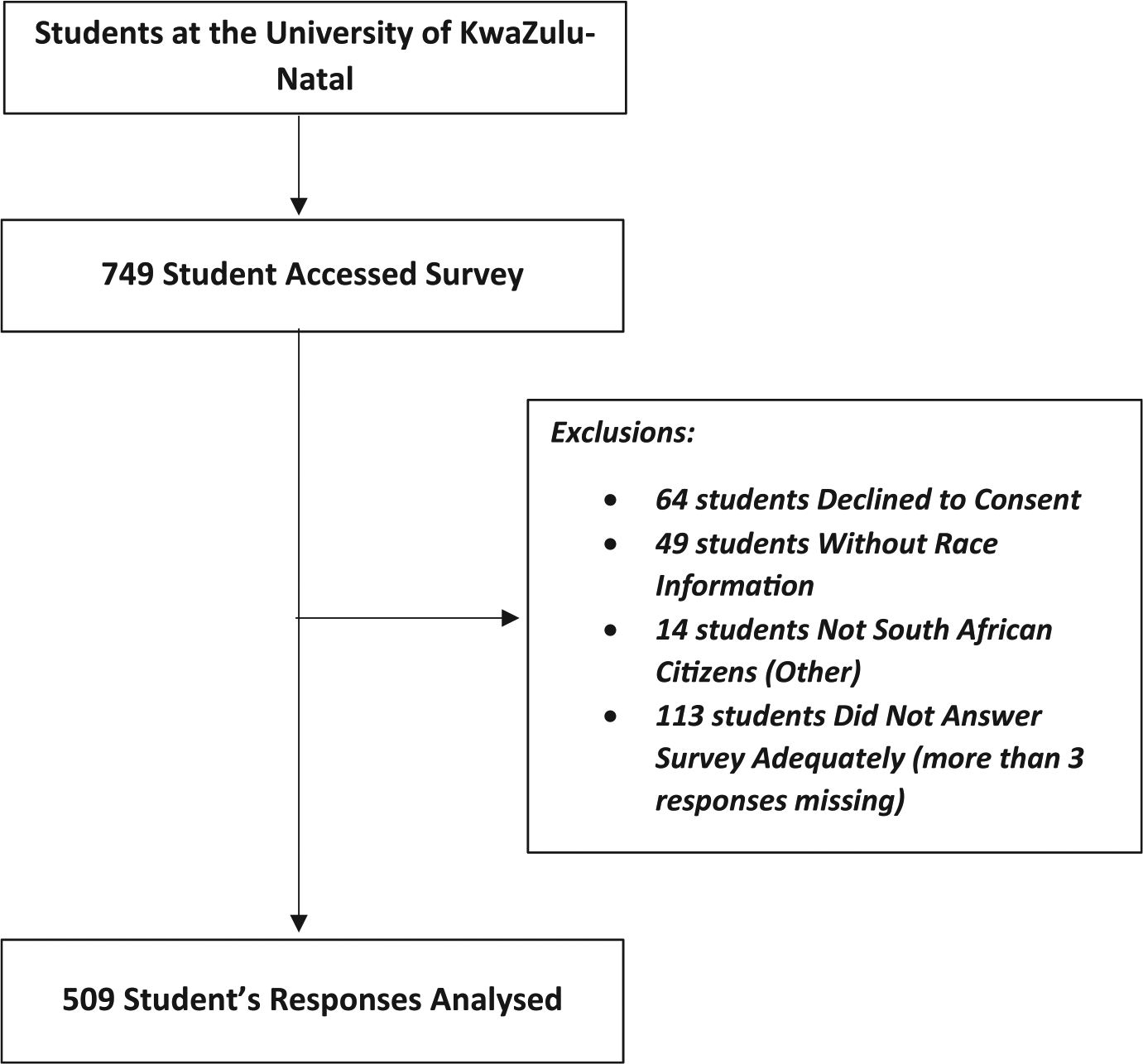
Consort diagram displaying the selection process for inclusion of data for analysis.
Instruments
The CRIS was designed specifically by Frew et al. (2010) with HIV prevention vaccines in mind (Figure 2). It was developed to understand factors influencing participation in HIV vaccine research since it is generally more difficult to enrol participants for this type of trial. The CRIS was, therefore, selected for this study due to its applicability to HIV prevention research which is the focus area of this study.
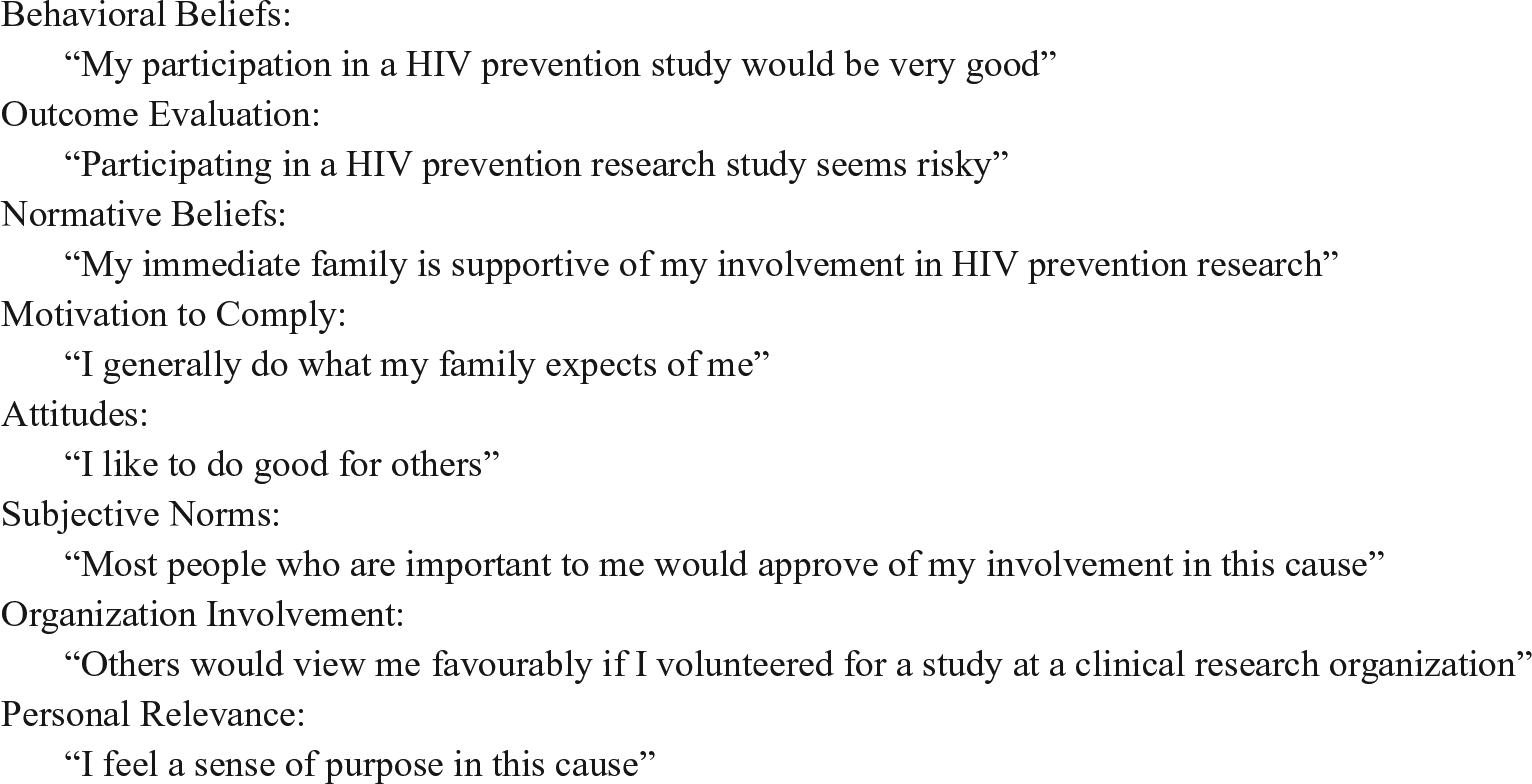
Examples of CRIS items (Frew et al., 2010) rated on a 5-point Likert-type scale.
The questionnaire for this study comprised two sections, demographics and the CRIS. The CRIS was used to measure WTP and intention to participate in HIV prevention research. The CRIS is a 5-point Likert-type scale (strongly agree to strongly disagree) consisting of 41 items with high reliability (0.734–0.918) and validity (Cronbach’s alpha = .850) (Frew et al., 2010). For this study, only 40 items from the CRIS were included. One question under Outcome Evaluation stating ‘I would participate in a research study, but I don’t like needles’ was specific to HIV vaccine trials and was excluded because our focus was on HIV prevention research generally, not just vaccine trials. The scale measured the following constructs in the TRA:

where AB = Σbiei, and SN = Σbimj (W1 = empirically derived weight of AB; W2 = empirically derived weight of SN)
Attitudes (AB): Assessed factors such as altruism towards participation in HIV prevention research, HIV as a community concern, HIV testing as a benefit of study participation, and medical care as a benefit of study participation.
Subjective norms (SN): Assessed opinions of referent others on HIV prevention research, approval of study participation, and support of study participation.
Behavioural beliefs (bi): The questions for this construct assessed beliefs around community and personal benefit of research, positive impact of action of participation on others, positive attitudes towards participation in HIV prevention studies, impact of participation in HIV prevention research, and non-monetary motivation to participate.
Outcome evaluations (ei): Assessed negative attitudes towards participation in HIV prevention research and barriers to participation such as time constraints and perceived risk of participation.
Normative beliefs (bj): Assessed referent doctors’ approval of participant involvement in research, approval of study participation by work colleagues and immediate family, opinion of referent others on participants’ involvement in HIV prevention research, support of referent others, and impact of religious leaders on study participation.
Motivation to comply (mj): Assessed concern over peers’ perceptions towards participation, actions towards family and friend perceptions, submission to superiors, and peer/social pressure.
The following additional constructs, even though not a part of the TRA, are also theorized to affect BIs and were assessed by the CRIS:
Organizational involvement: Assessed expression of self through the research organization, perception of involvement of others with the research organization, perception of others in respect of participants’ involvement with the research organization.
Personal relevance of volunteerism: Assessed empowerment through being involved with the research organization, feeling a sense of community in the cause and belonging through participation, altruistic intentions, sense of liberation through involvement, and a sense of purpose in the cause.
Procedure
Data were collected between September 2012 and April 2013 through invitations to participate on UKZN’s online notice system accessed by all registered students. Repeat postings were done daily except during university vacations. Students who volunteered completed an online informed consent before completing the questionnaire and were offered entry into a draw to win one of two mall vouchers after questionnaire completion. After 64 postings, a sample size of 636 students was reached.
Ethical considerations
This study received ethics clearance from the Biomedical Research Ethics Committee of UKZN (BE 094/11).
Data analysis
All data were analysed using IBM SPSS (v. 21) or SPSS AMOS Graphics (v. 21; IBM Corporation. SPSS AMOS, 1983, 2012).
Descriptive statistics
Means as a measure of central tendency and associated standard deviations were determined for age and both summed constructs and individual items in each construct.
Analysis of variance
Analysis of variance (ANOVA) was performed to determine racial differences in factors affecting WTP in HIV prevention research. The Bonferroni test was selected as a test for multiple comparisons. Significance was set at p < .05 as per accepted statistical standards.
Multiple linear regression
A multiple linear regression was performed to determine the effect of demographic variables on intentions to participate. The initial model was selected based on uncategorized independent demographic variables at a significance of p < .10 for forward selection. Based on the significance criterion, independent variables were selected and categorized into dichotomous variables for the final model. Selection of independent variables in the final model was based on significance of p < .05 (backward elimination).
Confirmatory factor analysis
A confirmatory factor analysis was performed to determine validity of the CRIS in this population. The model was created based on the design that all observed variables (constructs) are loaded onto a single factor (BI). Significance was set at p < .05 for each observed variable. Goodness of fit was determined by measurement of comparative fit index (CFI) and root mean square error approximation (RMSEA).
Results
Demographics
Participant demographics are shown in Table 1. Coloured students were not reported on separately due to the small sample size for this group (<10 females). Any students coded as ‘other’ were excluded from separate analysis.
Descriptive statistics.
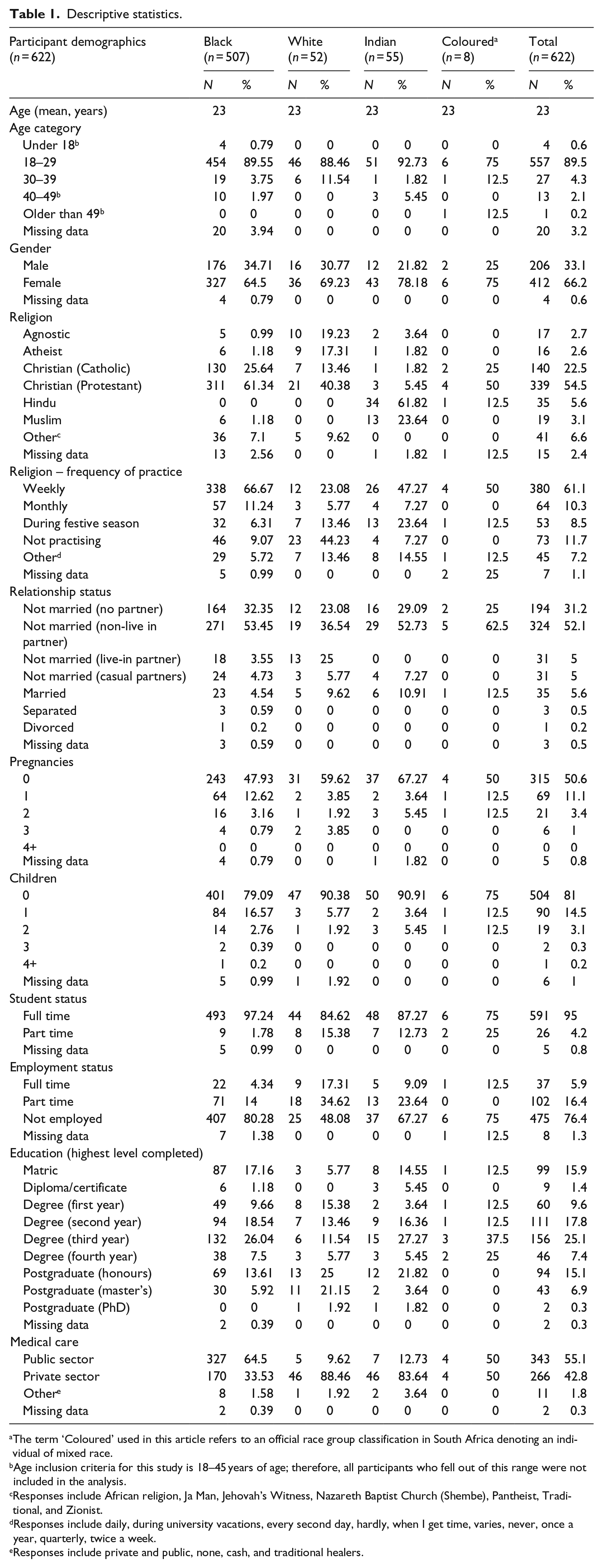
The term ‘Coloured’ used in this article refers to an official race group classification in South Africa denoting an individual of mixed race.
Age inclusion criteria for this study is 18–45 years of age; therefore, all participants who fell out of this range were not included in the analysis.
Responses include African religion, Ja Man, Jehovah’s Witness, Nazareth Baptist Church (Shembe), Pantheist, Traditional, and Zionist.
Responses include daily, during university vacations, every second day, hardly, when I get time, varies, never, once a year, quarterly, twice a week.
Responses include private and public, none, cash, and traditional healers.
The mean age of participants was 23 years, with two-thirds being female. Protestant Christianity was the most common religion among White and Black students and Hinduism among Indian students. Most (61.1%) actively practised their religion weekly. Most (52.1%) were unmarried but had a partner that they do not live with. Black female students reported three times more pregnancies (12.6%) than White (3.8%) and Indian (3.6%) students. Most (95%) students were full-time students with no employment. Of those with employment, White (34.62%) and Indian (23.64%) students reported higher rates of part-time employment compared to Black (14%) students. Public sector health facilities were used by 64.5% of Black students, while most White (88.4%) and Indian (83.6%) students accessed private health care.
WTP in HIV prevention research
WTP was determined by a single question under Behavioural Beliefs in the CRIS stating, ‘I would participate in a HIV prevention research study because it would help to prevent HIV/AIDS’. In total, 85.9% of the students were willing to participate, displaying positive behavioural beliefs about participation. Table 2 shows the ANOVA results of WTP in respect of race, and yielded non-significant results, F(3, 508) = .379, p = .768, indicating no difference in WTP determined by race. However, WTP was significantly higher among males than females, (p = .004) on the independent sample t-test.
Results of ANOVA measuring WTP across race.
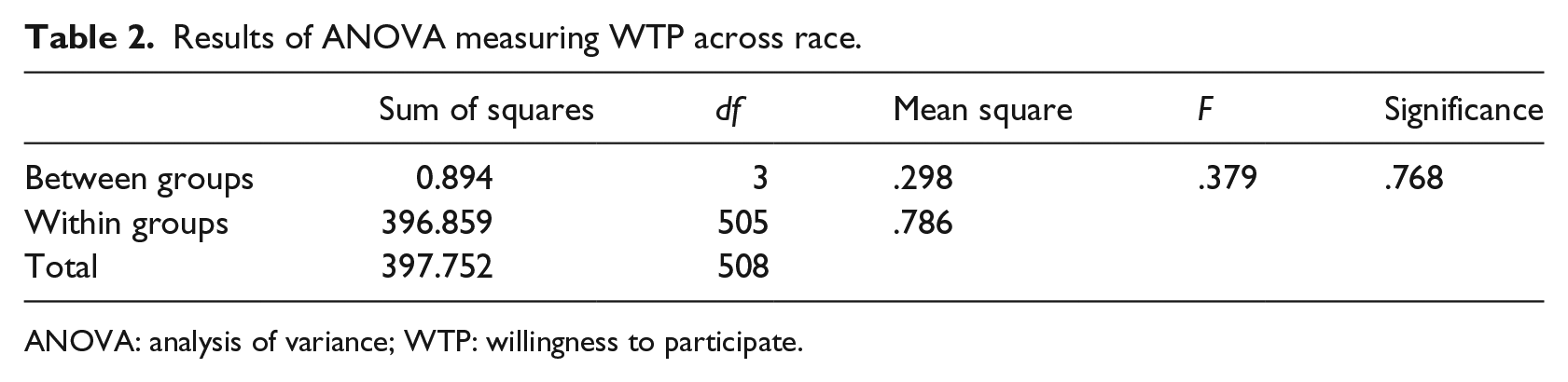
ANOVA: analysis of variance; WTP: willingness to participate.
Intentions to participate in HIV prevention research
Barriers to participation in HIV prevention research described in the literature, such as perceived benefit, time, and risk (Mills et al., 2004; Suhadev et al., 2009), were not perceived as barriers by students. HIV was perceived as a concern, and all participants showed positive attitudes towards HIV prevention research, benefits of research participation, and expressed positive perceptions towards being associated with a clinical research organization. Students expected approval and support for their participation in HIV prevention research. However, they were not highly influenced by peers and family expectations. Black students perceived a sense of purpose, belonging, and empowerment through potential involvement in HIV prevention research, compared to White and Indian students’ more neutral response.
There were similarities among race groups for most CRIS items, but the intensity of responses differed. ANOVA was conducted to determine the statistical significance of the difference in intensity. All factors except motivation to comply showed a statistically significant difference in responses (p < .05) as shown in Table 3. Bonferroni test for multiple comparisons was performed to determine in which race groups the difference lay. The differences were between Black and White students and Black and Indian students with no difference between White and Indian students (p > .05).
ANOVA of CRIS factors.
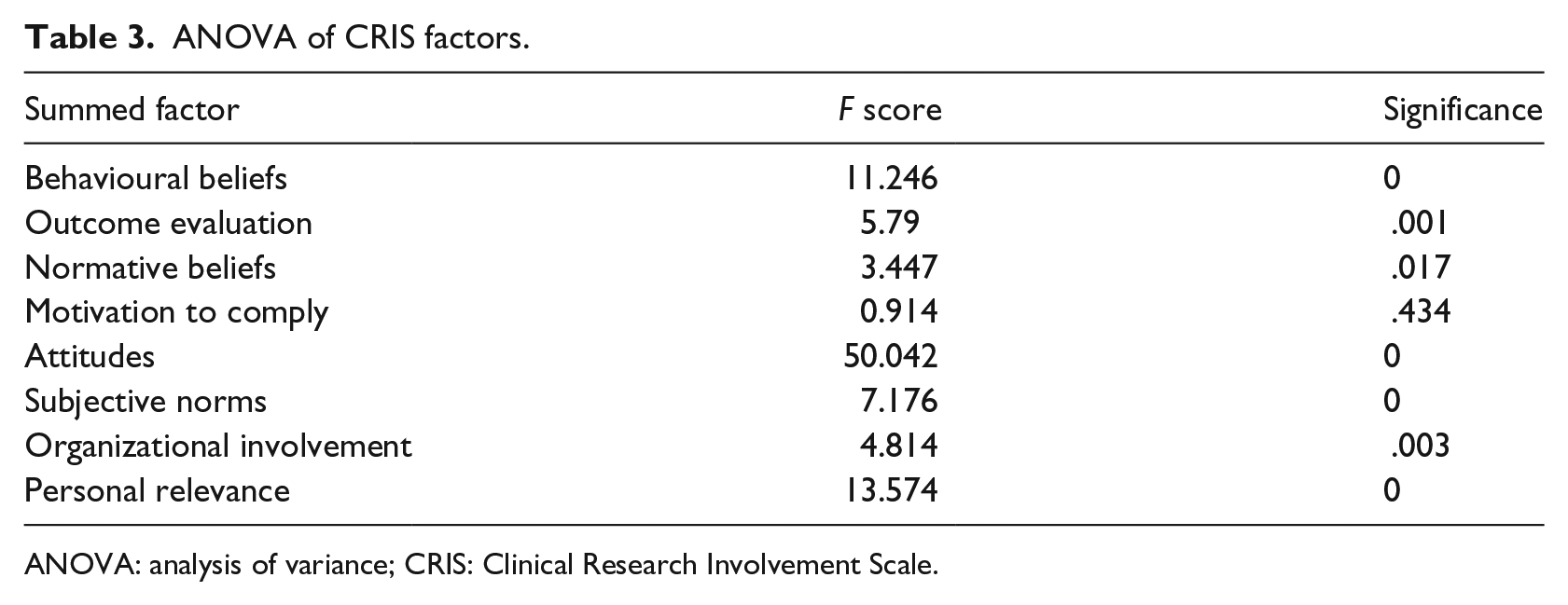
ANOVA: analysis of variance; CRIS: Clinical Research Involvement Scale.
For the multiple linear regression, a summation of all factors provided a measure of overall intent to participate in HIV prevention research and revealed that only age, gender, race, number of children, and access to medical care were statistically significant (p < .05) and influenced BIs to participate in HIV prevention research as shown in Table 4.
Results of multiple linear regression.
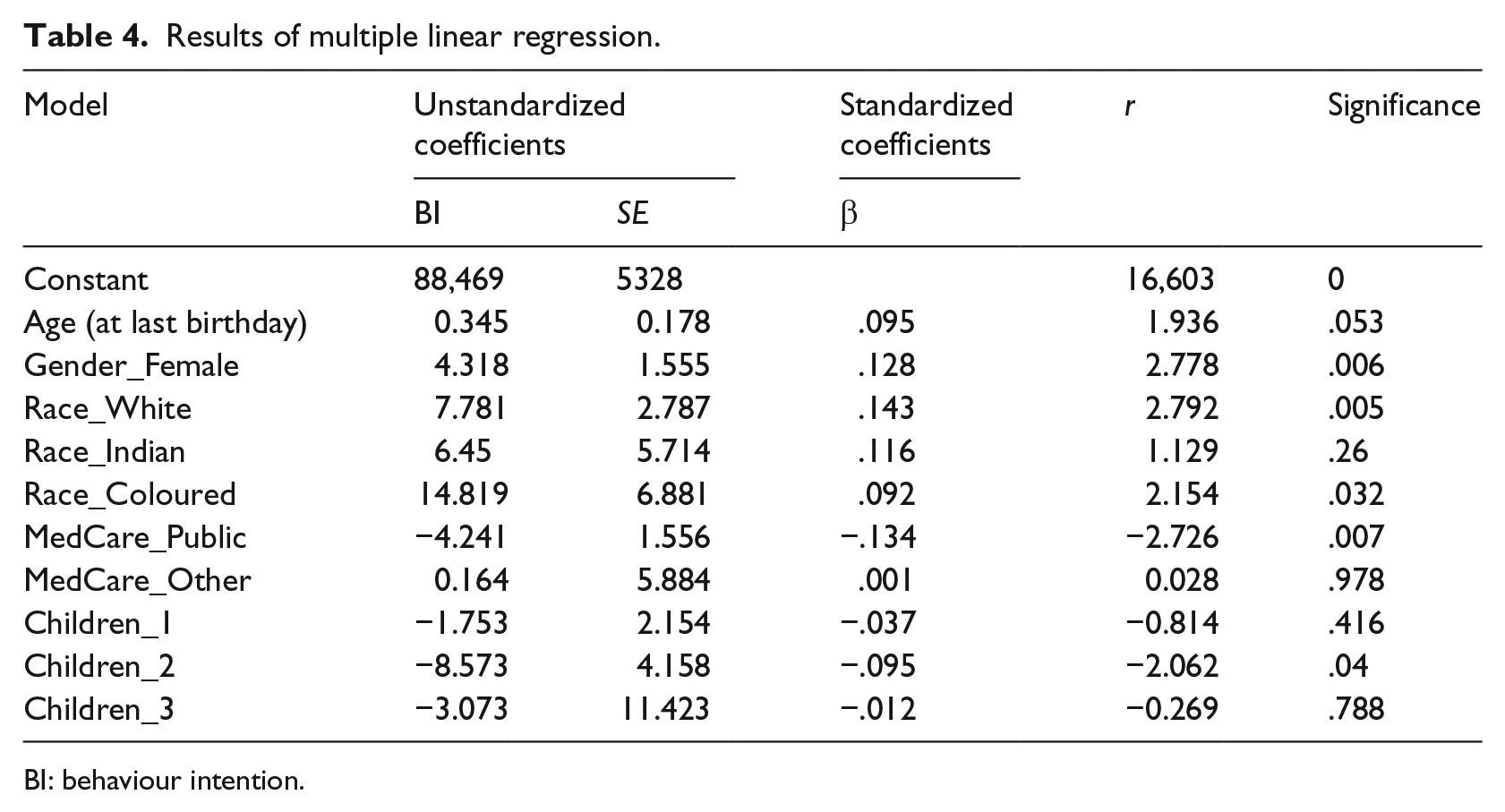
BI: behaviour intention.
The predictors of intention to participate in this regression model (Table 4) indicate that an increase in age showed declining intention to participate. Males showed greater intention to participate. Indian and Black students showed higher intention to participate than White students. Women with two children and students accessing public health care had greater intentions to participate.
The final linear regression model (ANOVA) was statistically significant (p > .05) but explained only 10.8% of variability in BIs to participate in HIV prevention research.
CRIS reliability, measured by confirmatory factor analysis, showed mediocre fit of the data per goodness-of-fit indices, CFI, and RMSEA. The CFI in this model was <.95 (CFI = .919), indicating mediocre fit. The RMSEA index favours a model with the least number of parameters. Current cut-off values suggest that an RMSEA close to .06 (upper limit of .70) indicates a good fitting model. The RMSEA for this model was .113 indicating a mediocre fit, which aligns with the CFI result. This could be due to the non-significance of motivation to comply in the model and low predictive value of outcome evaluation. This was substantiated when both motivation to comply and outcome evaluation were removed from the model, the CFI increased to .95, indicative of a well-fitting model.
Discussion
Willingness to perform a specific behaviour can be defined as a person’s openness to opportunity (Pomery, Gibbons, Reis-Bergan, & Gerrard, 2009). It involves little prior contemplation of the behaviour and its consequences (Pomery et al., 2009). Over 85% of this student sample reported WTP which favours future enrolment in HIV prevention studies. No significant racial difference in WTP in HIV prevention research was observed, similar to findings by Barsdorf and Wassenaar (2005) that reported no racial differences in WTP in future health research.
Even though there were no racial differences in WTP, Black students showed relatively greater interest in participating in this survey on HIV prevention. Racial differences were found in intention to participate in HIV prevention research. WTP was measured by a single question, whereas intention to participate was determined through cumulative scores from CRIS, which assessed attitudes, subjective norms, behavioural beliefs, outcome evaluation, normative beliefs, and motivation to comply. Intentions to perform a behaviour are assumed to reflect motivational factors that underlie specific actions (Pomery et al., 2009). Race was a significant predictor (p < .001) of intention to participate in HIV prevention research in the multiple linear regression model.
The attitudes of Black students towards participation in HIV prevention research differed significantly from White (p < .001) and Indian students (p < .001). Based on mean responses, Black students ‘agree’ that HIV is a serious concern in their immediate community, but White and Indian students displayed a neutral response (‘neither agree/disagree’) illustrating racial variability in risk perception. Students across all race groups perceived a benefit from HIV testing within an HIV prevention study, and mean responses show that Black students ‘strongly agree’ and White and Indian students ‘agree’. The intensity difference suggests that Black students perceived greater benefit from HIV testing in HIV prevention research than did White and Indian students. This illustrates that even though the epidemic is generalized, White and Indian students did not perceive as great a risk of acquiring HIV as did Black students.
Black students ‘agree’ that they would benefit from medical care associated with HIV prevention research, while White and Indian students ‘neither agree/disagree’. Demographic findings showed that 64.5% of Black students used public sector health-care services compared to 9.6% of White students and 12.7% of Indian students. Over 80% of White and Indian students reported utilizing private health care. South Africa has a fragmented health-care system split into public and private sectors (Coovadia, Jewkes, Barron, Sanders, & McIntyre, 2009; Pillay, 2009). Racial differences in utilization of the public and private health sector were evident in this sample. There is serious underperformance of the public health sector (Coovadia et al., 2009). Human resource issues, poor management, and HIV-associated illness burden have contributed to the current weakened state of the public health service (Coovadia et al., 2009).
However, the private sector, accessed by higher socio-economic groups, is reputed for world-class facilities and care provision (Pillay, 2009). As ethically required for biomedical HIV prevention trials, at a minimum, participants should have regular and supportive contact with health-care workers and counsellors throughout a clinical trial (UNAIDS, 2012). As a result, basic and ongoing health care is provided to all participants throughout trials (Essack, 2014; Slack, 2014). In settings where access to quality health services is an issue, access to health care rather than altruism may be a driving factor for participation in clinical trials (MacPhail, Delany-Moretlwe, & Mayaud, 2012). This was substantiated in our regression model where intention to participate in HIV prevention research was significantly higher among those accessing public health care compared to private health care.
Favourable social opinion of research involvement was theorized to increase participatory intention (Frew et al., 2010). Black students ‘agree’ that most people who were important to them thought that they should participate in HIV prevention trials compared to Indian students who ‘neither agree/disagree’, suggesting that Indian students did not expect the same social support as Black students regarding participation/involvement in HIV prevention research. This could be associated with low perceived risk among Indian students.
All race groups believed that HIV prevention research would benefit their community. However, the intensity of responses differed in Black students who ‘strongly agree’ compared with White and Indian students who ‘agree’. A similar finding was seen in responses to ‘My actions can inspire others to act’ and ‘my participation in a HIV prevention study would be very good’. Furthermore, Black and Indian students ‘agree’ that their involvement in prevention trials would improve their community’s trust in medical research, but White students ‘neither agree/disagree’. This implies a need for community engagement efforts among Black and Indian communities to improve trust in medical research. The legacy of human rights violations towards Black and Indian people during apartheid may have negatively impacted public perceptions of medical research in South Africa (Barsdorf & Wassenaar, 2005).
Both Black and White students ‘disagree’ that participation in HIV prevention research seemed risky, but Indian students ‘neither agree/disagree’, suggesting that Indian students had some indifference or uncertainty regarding the safety of HIV prevention research.
With regard to normative beliefs, Black, White, and Indian students ‘agree’ that their doctor, work colleagues, immediate family, and referent others would approve of their involvement in HIV prevention research. However, responses for Indian students were more ‘neutral’. Therefore, Black and White students believed that referent others in their community would support their participation in HIV prevention research.
Students did not appear to be swayed by concerns over peer perceptions or family expectations. Their responses indicated that their decision-making was individualistic rather than conformist. The greater self-agency displayed by these students should lead to greater participatory intention (Frew et al., 2010).
Black students ‘agree’ that being active in a clinical research organization would help express who they are while White students ‘neither agree/disagree’. Black students ‘agree’ that others would view them favourably if they volunteered for a study at a clinical research organization, while Whites ‘neither agree/disagree’. This indicates that Black students perceived involvement with a clinical research organization more favourably than White students.
Personal relevance of volunteerism may exert influence on behavioural intentions to participate in HIV prevention research. Black students saw greater personal relevance in volunteerism compared to White (p < .001) and Indian (p = .002) students. This could be linked to Black students’ risk perceptions. Black, White, and Indian students all ‘agree’ that their involvement would help advance and protect the rights of others and that through support of HIV prevention trials they would be advancing the public health and well-being.
Intention to participate in HIV prevention research was defined by the total score of the eight factors of the CRIS, referred to as the BI score (Frew et al., 2010). The higher the BI score, the less intent there was to participate in HIV prevention research (Frew et al., 2010). The demographic component revealed racial differences in WTP in HIV prevention research, as defined by the BI score, compared to the single question to assess WTP. White students had lower intentions to participate than Black students. There is no comparable data to draw from in the literature since the BI as defined by the CRIS has not been tested in this manner before.
WTP in HIV prevention research also declined with age (p = .05), but no racial differences were observed. Female participants accounted for two-thirds (66.2%) of the study sample, which is fitting for our South African epidemic since females are disproportionately affected in terms of acquisition of HIV in South Africa (Shisana, 2013). ‘The disproportionately high HIV prevalence levels amongst young females in the country, however, requires a rethinking of conventional approaches to HIV prevention that addresses the underlying socio-cultural norms . . .’ (Shisana, 2013). Female representation in this study shows that young female students are willing to participate in HIV prevention studies, especially since many HIV prevention studies are female specific. Nevertheless, Black (92.1%) and White males (92.9%) displayed greater WTP in HIV prevention research than Black (82.5%) and White females (78.8%), while Indian females (91.7%) displayed greater WTP in HIV prevention research compared to Indian males (77.8%), but this result could be attributed to the unequal sample sizes. Enrolment statistics by gender for the HIV prevention vaccine study called HVTN 503 (Phambili) showed that there were 55.1% males and 44.9% females (Gray et al., 2011). Even though females have higher HIV prevalence, males were more willing to participate in HIV prevention research, except Indian males, consistent with our findings. This could be due to females’ lack of awareness of HIV risk or due to constraints arising from greater poverty and lower literacy (Wassenaar & Barsdorf, 2007). However, it is promising that most students report WTP despite some race and gender differences.
The majority (81.0%) of female students reported no pregnancies. However, the proportion of Black female students who reported one pregnancy (12%) was 4-fold higher than White and Indian students and 96% of Black female students who reported one pregnancy were unmarried. In the preceding five decades, teenage and premarital pregnancy were a norm for Black women (Coovadia et al., 2009). Pregnancy can largely be seen as an indicator of unprotected sexual activity and low contraception adherence. The regression model indicated that females who had two children had greater intention to participate than those with no children. This could be due to a health preservation drive among those with dependants, suggesting a greater interest in preventing infection or could be driven by economic benefits derived from the reimbursement provided to clinical trial participants.
Most (94%) of respondents were unmarried, while over 50% of students reported being in a relationship. The 2012 National Population HIV survey revealed that HIV among unmarried individuals is twice that of married individuals (Shisana, 2013). This was correlated with unmarried individuals having a greater likelihood of reporting multiple sex partners in the preceding 12 months (Shisana, 2013). Our data revealed that 25% of White students and 3.55% of Black students were currently unmarried and cohabiting with partners. Furthermore, 7.27% of Indian students, 5.77% of White students and 4.73% of Black students reported having casual sexual partners. Cohabiting is viewed as a risk factor for HIV acquisition because condom use among couples who cohabit is lower, with resistance from males in these partnerships (Maharaj & Cleland, 2005). Resistance to condom use among cohabiting couples can be attributed to perceived lack of trust (Maharaj & Cleland, 2005). However, many infections occur in such relationships either as a result of infidelity or unknown prior infection by one partner (Maharaj & Cleland, 2005). Although casual sexual partners were low in this sample, their existence was still present. The level of risk associated with casual relationships is dependent on whether the individual has repeated or once-off contact with casual partner/s and if the individual has multiple concurrent casual partners (Mah & Shelton, 2011). Another important factor associated with casual partners is substance abuse (Mah & Shelton, 2011), which this study did not assess. Relationship status had an influence on the level of risk exposure, but it was not a predictor of intention to participate in HIV prevention research.
With regard to the possible role of incentives/inducements in WTP, national guidance suggests that participants be reimbursed according to time, inconvenience, and expenses incurred (Koen, Slack, Barsdorf, & Essack, 2008; National Health Research Ethics Council, 2012). In low- and middle-income countries, there is concern that reimbursement may be a driving factor for participation (MacPhail et al., 2012). Most (>80%) of the participants in this study were full-time students. However, more Black students (80.28%) reported being unemployed compared to White (48.08%) and Indian (67.27%) students. More White (34.62%; 17.13%) and Indian (23.64%; 9.09%) students were part- and full-time employed, respectively compared to Black students (14.00%; 4.34%). Lower financial status is a risk factor for HIV infection in South Africa (van Staden & Badenhorst, 2009). Students reliant on bursaries, which are often distributed late in the academic year, experience financial difficulties, resulting in some female students engaging in transactional sex (van Staden & Badenhorst, 2009). However, employment status in this study did not influence intention to participate in HIV prevention trials.
A study of sexual behaviour among Ugandan university students found religion to be an important determinant of sexual behaviour (Agardh, Tumwine, & Ostergren, 2011). HIV prevention clinical trials promote condom use and provide condoms to participants as part of a comprehensive package of prevention and require participants to use contraception to prevent pregnancy since the effect of biomedical agents on the foetus is unknown. Condom and hormonal contraception are prohibited in some religions and could affect intention to participate in HIV prevention research. Most (54.5%) participants were Protestant Christians of various denominations. Across all religions and race groups, the majority were willing to participate in HIV prevention research. Students displayed a neutral response to the item ‘If my religious leader supported HIV prevention research, I would be inclined to get involved’. Hence, religion and the influence of a religious leader on decision-making was not a predictor of WTP in this population, supported by the non-significance of the religion variable in the regression model for BI.
The CRIS was reliable in this study with a Cronbach’s alpha statistic of .90. However, the confirmatory factor analysis which measures structure validity indicated that in its current structure, the CRIS had a mediocre fit to the data from this population. Removal of the outcome evaluations and motivation to comply improved the fit of the data in the model. Selection bias, described as under-coverage/volunteer bias may affect this study. However, because the participation invitation was placed in a central location that all UKZN students could access, bias is likely to be minimal. Minimal under-coverage bias was present as Indian students were under-represented by 17% and Black students were over-represented by 18%. Coloured groups were not reported on separately because numbers (n < 10 females) were too low to analyse statistically.
Only UKZN students were selected for this study, so results are not necessarily generalizable to students from other South African universities.
Since an incentive was provided in this study, socio-economic status, which was not assessed, could have been a confounder to participation, and since the survey was conducted online, a single student could have done the survey more than once.
Conclusion
Encouragingly, most students reported WTP in HIV prevention trials. No significant racial differences in WTP were found. However, race appeared to play a pivotal role in intentions, being the interplay between attitudes, subjective norms, behavioural beliefs, outcome evaluation, normative beliefs, and motivation to comply, to perform such actions. Gender also played an important role with males displaying significantly greater intention to participate than females. Cultural, gender, and subjective norms need to be taken into consideration when developing community engagement strategies for recruitment of students into HIV prevention trials.
Footnotes
Acknowledgements
We thank Tamaryn Nicolson for assistance with formatting this article for publication.
Funding
This work was partially supported by the NIH/Fogarty International Center, Grant Number 5 R25 TW001599-15.