
Abstract
In South Africa, traditional healers treat a wide range of health-related problems and culture-bound syndromes considered non-responsive to Western medicine. Given the widespread use of traditional medicine in treating common mental disorders, especially among low-income groups, it is important to explore the self-identification, training, and practices of traditional healers. We also explored traditional healers’ perceptions of collaboration with Western health care institutions (hospitals, clinics). IsiXhosa traditional healers (n = 50, female = 40, mean age = 52.7 years, SD = 14.7 years) were interviewed using both a structured and a semi-structured interview schedule, including the Patient Health Questionnaire-9. Data were analysed using SPSS version 24 and Statistica. Interview notes were typed soon after each interview and thematically analysed. Participants described similar experiences regarding the three steps of becoming a traditional healer and treating clients with mental illness using herbs (90%), candles (82%), and prayer (78%). Self-identification as a spiritualist or sangoma, and type of church attended (African Initiated vs. Mainline Christian) were both significantly associated with traditional healers’ mode of diagnosis and/or treatment. Participants were open about collaborating with Western health care institutions around treating mental health issues. However, this was hampered by mistrust, as evidenced in the reluctance of a few participants to share detailed information about treatment methods.
Introduction
Approximately half of all individuals seeking help for mental health issues in Africa choose to be seen by traditional/religious healers (Burns & Tomita, 2015). Traditional medicine is widespread in low- and middle-income countries (Gureje et al., 2015; Nortje, Oladeji, Gureje, & Seedat, 2016) and is increasingly recognized as a health care option in developed countries. The World Health Organization (WHO; 2013) defines traditional medicine as: . . . the sum total of the knowledge, skill, and practices based on the theories, beliefs, and experiences indigenous to different cultures, whether explicable or not, used in the maintenance of health as well as in the prevention, diagnosis, improvement or treatment of physical and mental illness. (p. 15)
In addition, the WHO (2013) defines complementary medicine as ‘a broad set of health care practices that are not part of that country’s own tradition or conventional medicine and are not fully integrated into the dominant health-care system’ (p. 15). In South Africa, traditional healers (THs) treat an array of health-related problems as well as culture-bound syndromes or ailments considered non-responsive to Western medicine (Truter, 2007). Traditional beliefs are common among communities such as the South African Xhosa community (Schierenbeck, Johansson, Andersson, Krantz, & Ntaganira, 2018) where THs are often sought to treat amafufunyana 1 (a culture-specific term used by THs to explain abnormal behavioural, and psychological phenomena or mental health issues; Niehaus et al., 2004) and other culture-bound syndromes. A systematic review has indicated a high degree of satisfaction among clients for mental health care received from THs (van der Watt et al., 2018). However, the review highlighted the limitation of the blanket term ‘traditional healers’ and the lack of a proper operational definition (both in the South African Traditional Health Practitioners Act of 2007 and academic research in general) in determining which specific methods of traditional healing is used in the treatment of mental illness and which is deemed most successful.
Schierenbeck and colleagues (2018) emphasized the importance of THs, especially in the delivery of mental health services and treatment of mental illness, since THs are often more accessible and their traditional interpretations of mental illness are viewed as more acceptable and less stigmatized by patients, compared to conventional medical care. Although South Africa’s Mental Health Care Act (No. 17, 2002) stresses a biopsychosocial approach to the delivery of mental health care, treatment, and rehabilitation to mental health care users; the Traditional Health Practitioners Act (Act 22, 2007) recognizes THs as legitimate health care providers (Schierenbeck et al., 2018). Thus, there appears to be a societal acceptance of both TH and biomedical medicine in the health care realm. However, a full and explicit collaboration between these two systems of treatment has not occurred. The implementation of collaborative care that encompasses both biomedical and traditional medicine appears to be challenged by ongoing tensions between the two approaches in the provision of mental health services in South Africa (Schierenbeck et al., 2018).
Moreover, providing culturally relevant mental health services is a challenge in the multicultural and multilingual society of South Africa where some Western-trained mental health professionals do not necessarily share the worldview or language of their clients. It is widely documented that language discord impedes access to health care and may negatively influence the quality of health care (Elkington & Talbot, 2015). Historically, Whites (mostly Afrikaans and English-speaking) have had easier access to psychological training programmes in South Africa compared to Black citizens (Vontress & Naiker, 1995). Although this trend has changed in post-apartheid South Africa (Leach, Akhurst, & Basson, 2003), the change remains slow. For example, in a survey by Pillay and Siyothula (2008), as little as 325 Black African clinical psychologists were identified as being registered at the Health Professions Council of South Africa (HPCSA). As such, many mental health providers still lack the culturally sensitive psychotherapeutic skills necessary for providing culturally competent services to a diverse and multilingual society where 11 official languages are spoken (Marchetti-Mercer & Cleaver, 2000). Many Black South Africans view Western approaches to health and healing with suspicion since it is not part of their traditional African worldview and cultural legacy of healing (Bojuwoye, 2005). In practice, however, an informal level of collaboration is usually initiated by the clients and/or their family members as they attempt to use both modalities for healing. Studies are thus needed to better understand the relationship between Western medical providers and THs. One way to do this is to explore the perceptions of THs regarding their role in providing mental health care as a complementary modality to Western medicine in South Africa.
Given the widespread use of traditional medicine in South Africa, especially among low-income Black African communities, the aim of this study was to explore the self-identification, training, and practices of THs; specifically in terms of mental health care. We also explored THs’ perceptions of collaboration with Western health care institutions (hospitals, clinics). This was a mixed-methods study that had the goal of gaining descriptive data from a specific community of isiXhosa-speaking THs.
Method
The study had two phases. In the first phase, all participants (N = 50) completed a questionnaire that was read by a member of the research team who also wrote down participant responses. The questionnaire included two open-ended questions that allowed participants to talk as long as they wanted. Where necessary, the researcher asked for clarification. In the second phase, participants (n = 4) who were purposefully recruited from Phase 1 participated in an in-depth interview. The findings of Phase 2 are published elsewhere.
Participants
A total of 50 isiXhosa-speaking THs, aged 21 years and older, born and raised in South Africa, and practicing as THs, were purposefully recruited using snowball sampling. Two members of the research team, who are also members of the Xhosa community from which participants were recruited, discussed the study with THs and invited them to participate in the study. Participants were encouraged to refer other interested THs to the study. All participants received ZAR150 to cover their time and transportation costs. An additional incentive of ZAR50 was offered to THs who were able to refer other THs who were later successfully recruited into the study.
Instruments
Data were collected using a structured questionnaire. The structured interview consisted of four sections: (a) demographic information, (b) becoming a healer, (c) traditional healing as occupation, and (d) client and diagnoses/treatment information. The interview schedule included two open-ended questions: (a) Describe the training to prepare you to become a traditional healer and (b) Describe the work that you do as a traditional healer from the first time a client comes to you for help. Although these were the only open-ended questions, participants, in keeping with their oral tradition, tended to respond at length to most questions. Thorough notes, including direct quotations where possible, were taken of participant responses and typed after each interview.
Patient Health Questionnaire
Due to the high rates of mental illness, in particular depression and depressive symptomatology, among biomedical health care providers (Brooks, Gerada, & Chalder, 2011; Mata et al., 2015; Ruitenburg, Frings-Dresen, & Sluiter, 2012; Tyssen & Vaglum, 2002), we screened for depression in this sample of THs using the Patient Health Questionnaire-9 (PHQ-9) to establish whether THs had similarly high rates. The PHQ is a nine-item self-report questionnaire based on the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria for major depressive disorder (Martin, Rief, Klaiberg, & Braehler, 2006). The PHQ-9 scores each of the depression criteria as 0 = not at all to 3 = nearly every day (Kroenke, Spitzer, & Williams, 2001). Cut-off scores of 5, 10, 15, and 20 (out of a total score of 27) represent mild, moderate, moderately severe, and severe depression, respectively (Martin et al., 2006). In the present sample, the PHQ-9 had high reliability with α = .81. Due to the sensitive nature of the PHQ-9, the instrument was administered in the participants’ preferred language by the third author, a member of the isiXhosa-speaking community.
Procedure
Participants could choose whether they wanted the interviews to be conducted in English (n = 24), Xhosa (n = 20), or a mixture of both (n = 6). All participants signed an institution-approved informed consent form after the study was reviewed with them and any questions they had were answered. Prior to participation, the voluntary and confidential nature of the research was emphasized. Two research team members were present at each interview. One took notes that were typed immediately after each interview, while the second researcher asked questions and served as a translator. The interviews were individually conducted and were not audio recorded.
Ethical considerations
Ethical approval for the study was obtained from the Chicago School of Professional Psychology (IRB16-01-0056) and Stellenbosch University (N/16/05/059) since both institutions collaborated on this study. All electronic files with identifiable information were password protected.
Data analysis
Quantitative data were analysed using SPSS24 (SPSS, 2016) and Statistica (2015). Frequencies and means were calculated. Chi-square tests and Fisher’s exact two-tailed tests were run to analyse the relationship between church attended, self-identification (e.g., as spiritualist, healer, or sangoma), mode of diagnosis, and mode of treatment. In addition, correspondence plots were conducted. All tests were two-sided and the p-value set at .05. Transcribed interview notes were thematically coded (Braun & Clarke, 2006). Typed notes and direct quotations (where possible) were used to enrich quantitative findings.
Results
This section presents results from Phase 1 of the study.
Participants
A total of 50 participants (female = 40, mean age = 52.56 years, SD = 14.6 years, range = 22–74 years) completed Phase 1. The majority of participants had family members who were also THs stating that ‘it’s like a family gene’ (Participant 3) and ‘it is where it come [sic] from’ (Participant 17). Additional demographic data are presented in Table 1.
Participant demographic information.
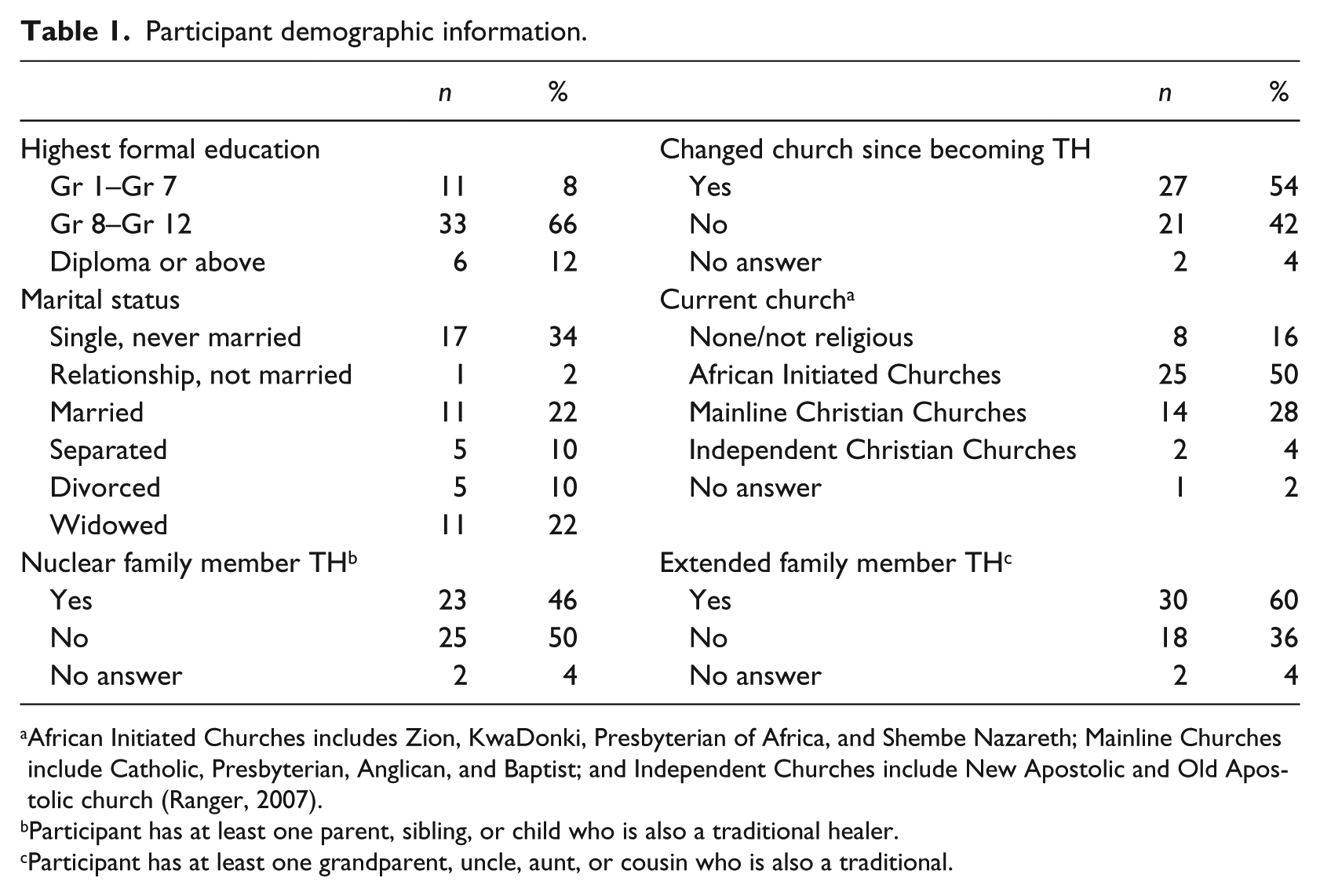
African Initiated Churches includes Zion, KwaDonki, Presbyterian of Africa, and Shembe Nazareth; Mainline Churches include Catholic, Presbyterian, Anglican, and Baptist; and Independent Churches include New Apostolic and Old Apostolic church (Ranger, 2007).
Participant has at least one parent, sibling, or child who is also a traditional healer.
Participant has at least one grandparent, uncle, aunt, or cousin who is also a traditional.
Mental health of the participants
Even though previous studies have reported high rates of depression and depressive symptoms among biomedical care providers (Brooks et al., 2011; Mata et al., 2015; Ruitenburg et al., 2012; Tyssen & Vaglum, 2002), a similar pattern was not found among THs in this study. Only three participants (6%) self-reported that they were previously hospitalized for mental illness. 2 However, this finding should be interpreted with caution due to response bias (Mata et al., 2015; Ruitenburg et al., 2012). PHQ-9 scores ranged from 0.0 to 20.0 (M = 2.7, SD = 3.7). Overall, 41 (82%) participants had scores indicative of minimal depression (PHQ Total ⩽ 4), with only 1 participant (2%) scoring above the cut-off for moderate depression (PHQ Total > 14). Even though the PHQ-9 had good reliability (α = .81), the data were not normally distributed.
Identifying as a healer, sangoma, herbalist, or spiritualist
Participants were asked about how they self-identified in terms of their traditional healing practice/s (see Table 2). Some participants appeared to have a clear preference: ‘I’m a doctor, not a herbalist’ (Participant 1) and provided brief explanations for why they self-identified in a particular way. For example, Participant 50 said he was a spiritualist ‘because I use water’. In contrast, Participant 6 cared little about what he is called: ‘They call us too many names. It is a calling; you can’t worry too much about names’. Nonetheless, data analysis indicated that how participants referred to themselves was related to how they diagnosed clients and the treatment methods that they used. In addition, correspondence analysis indicated spiritualists, healers, and sangomas differed in terms of diagnoses (see Figure 1). Specifically spiritualists and healers corresponded more closely to each other compared to sangomas in terms of their treatment methods (see Figure 2).
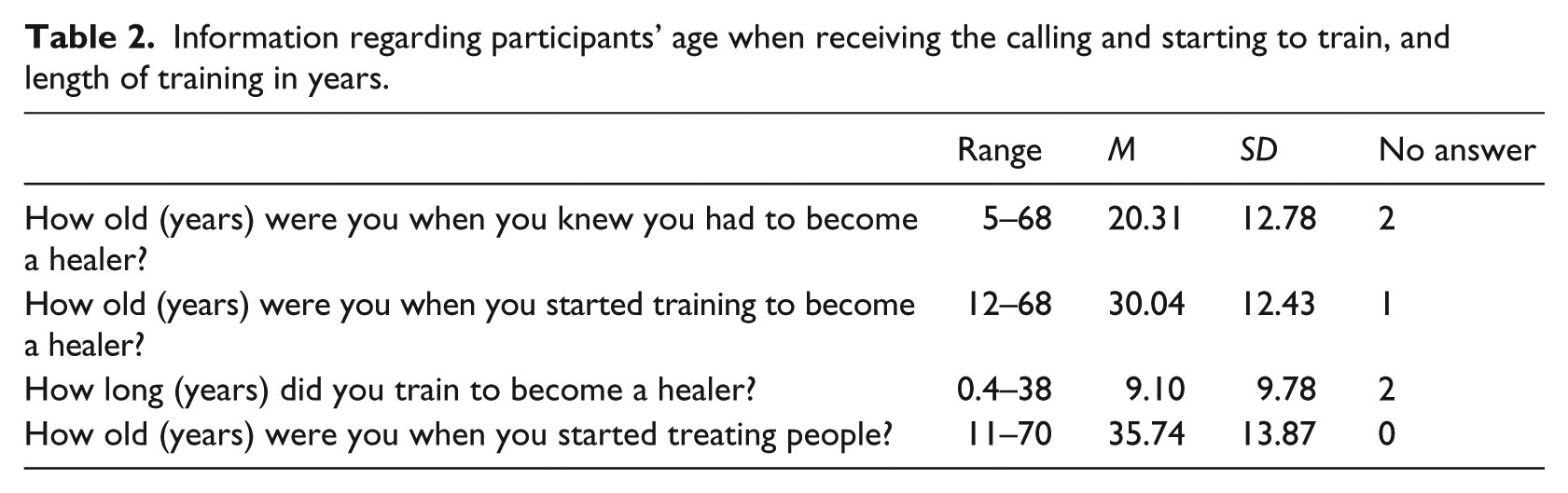
Information regarding participants’ age when receiving the calling and starting to train, and length of training in years.
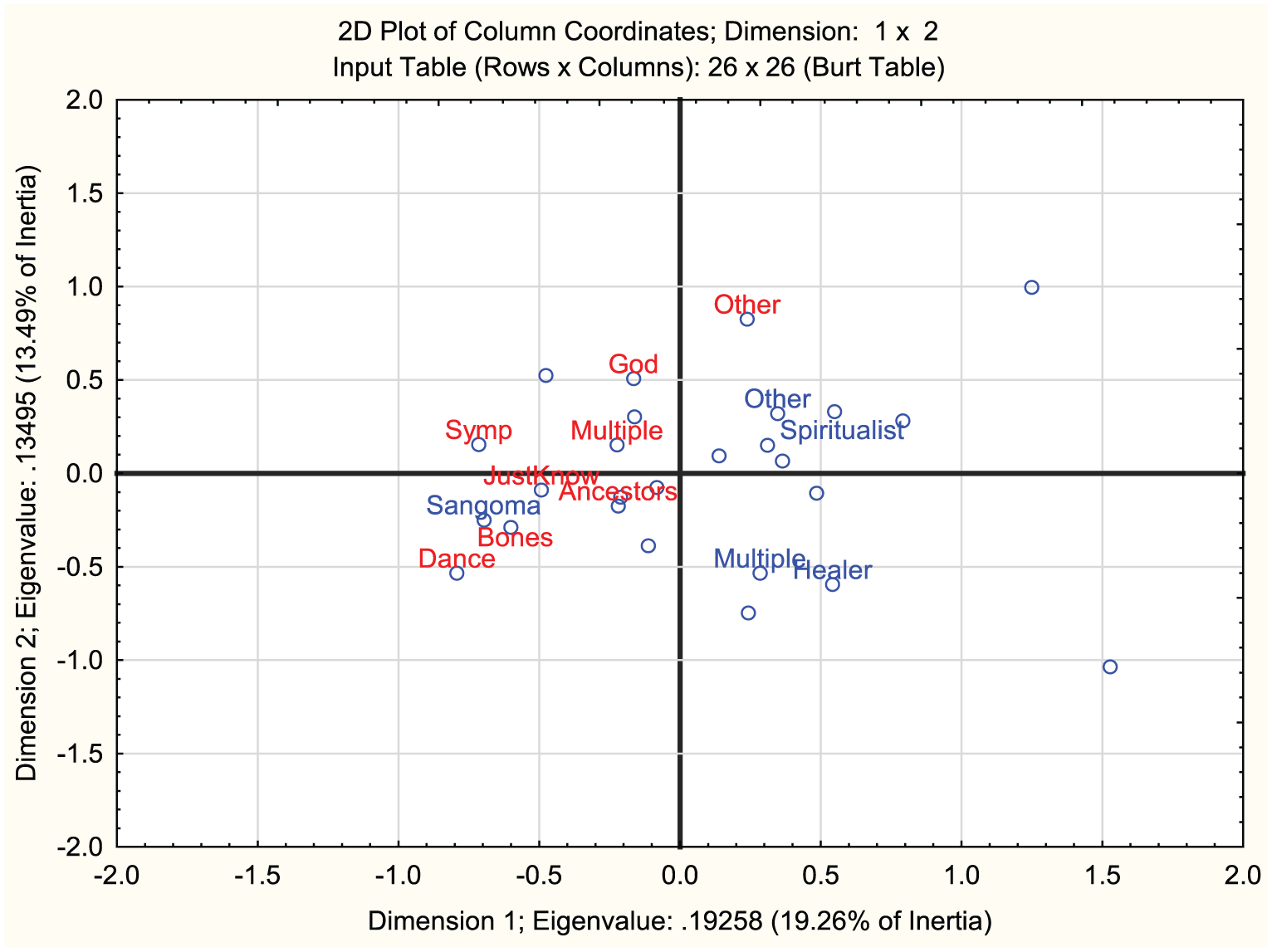
Correspondence analysis: Correspondence between what participants’ self-identify as and mode of diagnosis.
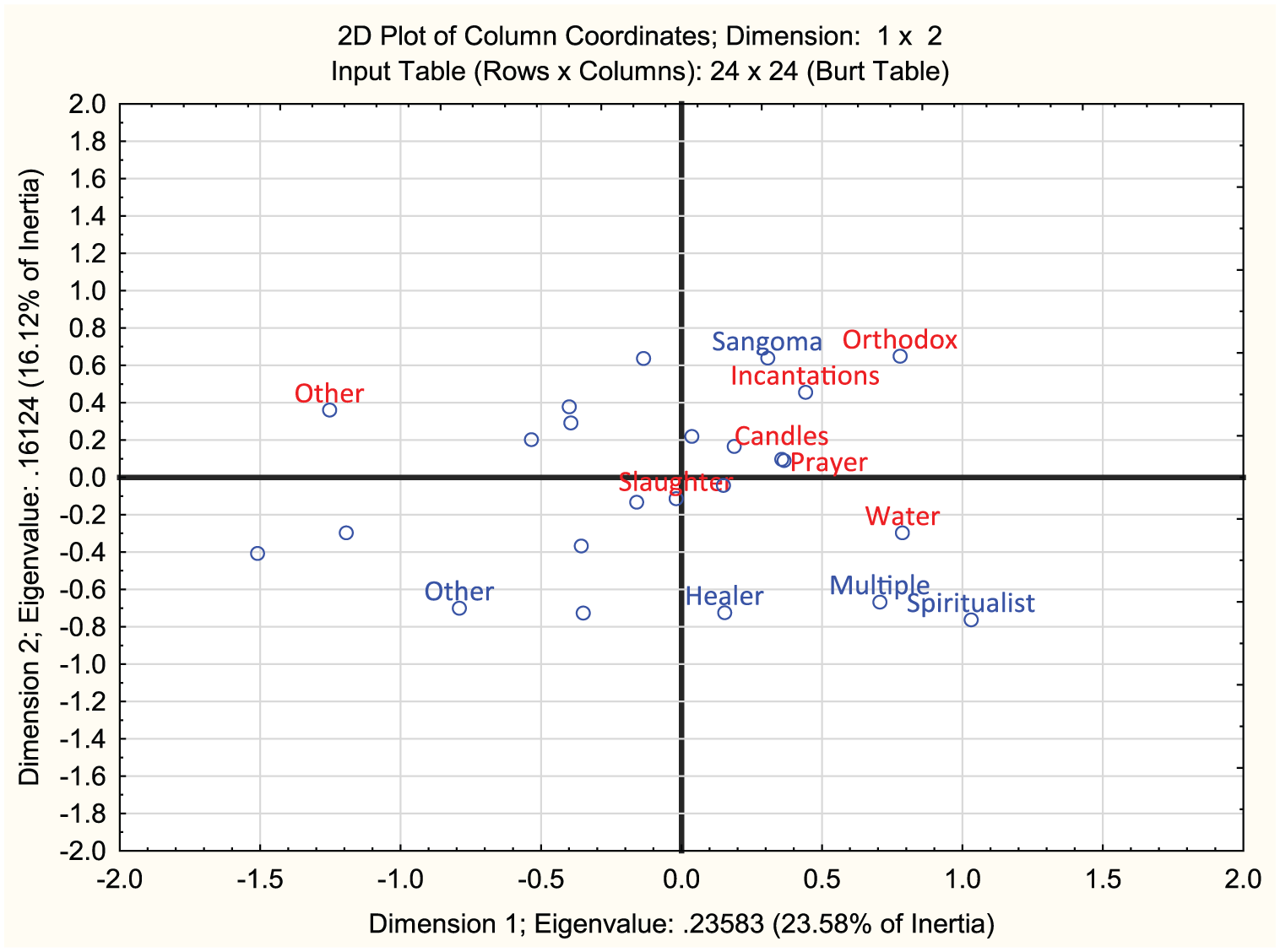
Correspondence analysis between participants self-identification and their mode of treatment.
Training to become a healer
In total, 29 participants (58%) indicated that they had attained certification as THs. These certificates ranged from a document issued by the participant’s trainer, certificates obtained through workshop attendance (including tuberculosis, HIV/AIDS, or capacity building workshops), to identification and registration documents that provided participants with the right to practice in specific geographical areas. The age at which participants were first aware that they had to become healers or received the calling varied widely as did their length of training (see Table 3). However, becoming a healer was described as ‘a long journey; it takes very long’ (Participant 18). To become healers, 23 participants (46%) were trained by more than one healer, with 27 (54%) trained by one healer only.
Identifying as a healer, sangoma, herbalist, or spiritualist.
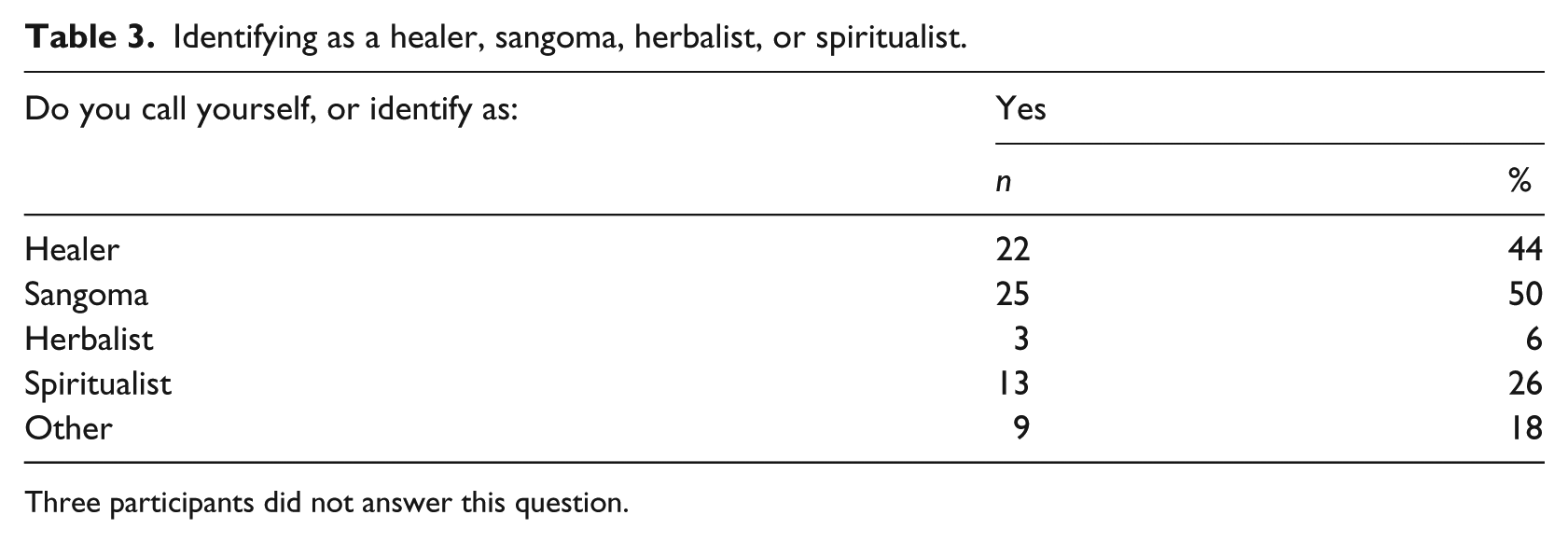
Three participants did not answer this question.
Participants’ descriptions of their training to become healers varied; however, it generally involved three steps:
Slaughtering of an animal to accept the calling;
Staying at a river (or in the forest) 3 to connect with ancestors;
Performing a final ceremony in which an ox or cow was slaughtered.
For example, Participant 22’s description of the first and second part of her training was as follows: After slaughtering a goat to accept her calling, her trainer took her to a river in the Eastern Cape. They took a bucket of isilawu [traditional beer], corn, beans, tobacco, and ubulawyo [traditional medicine] with them. This was all poured into the river as a gift to the ancestors. The gift swirled and was taken away by the river. At the river, they said many incantations in order to tell the ancestors why they were there.
The importance of dreams was also highlighted: ‘. . . the dreams have to guide you’, (Participant 7), and ‘you can’t do anything without a dream’ (Participant 1). Participants described that their trainers were revealed to them through their dreams or dreaming of the specific animal that they had to slaughter as part of their training. For example, Participant 38 described the following: In a dream, she was told to slaughter an ox. In her dream, she was told the exact house where she would find the specific ox and the colour of the ox. When she arrived at the specific house, the family told her that the ox did not come down to the kraal anymore, but that it lived in the veld. They went looking for the ox and as they were looking, she heard an ox cry. She told the family that she had to have the ox that cried and the family confirmed it as the ox she described. To transport the ox, they had to bring a truck and put branches of the umnquma tree inside. As the ox was standing by the gate, it urinated, bellowed, and looked in the direction they were to take. By doing this, the ox was indicating that it was happy with its destiny.
During the different stages of training, participants were taught about the different herbs and their specific purpose. They also observed how their trainers healed clients, sometimes assisted their trainers with treatment, or independently started treating clients under supervision.
Working as a healer
Most participants (n = 48, 96%) worked at home in an office that they described as their surgery, 4 regarded healing as their full-time job (n = 38, 76%), and depended on healing as their main source of income (n = 29, 58%). The majority of participants reported that clients were referred to them by word-of-mouth (n = 46, 92%), with only one participant (2%) advertising to recruit clients. Some participants acknowledged that the church often referred clients to them (n = 13, 26%), while others reported that church pastors informed congregants not to seek traditional healing, despite seeking traditional treatment themselves. For example, Participant 33 explained how pastors would secretly come to her at night to be ‘washed’ to ‘get lucky’ so that more people would join the congregation.
Modes of diagnosis and treatment
The majority reported that they treated both mentally and physically ill patients (n = 30, 60%). However, many participants who stated that they did not treat mental illness indicated that they treated Xhosa illness that was described as behaviour that is aberrant or unusual and/or of a psychological nature. All participants in this study reported a willingness to train others to become healers. Table 4 provides a summary of the mode of diagnosis and treatment applied.
Mode of diagnosis used and treatment used.
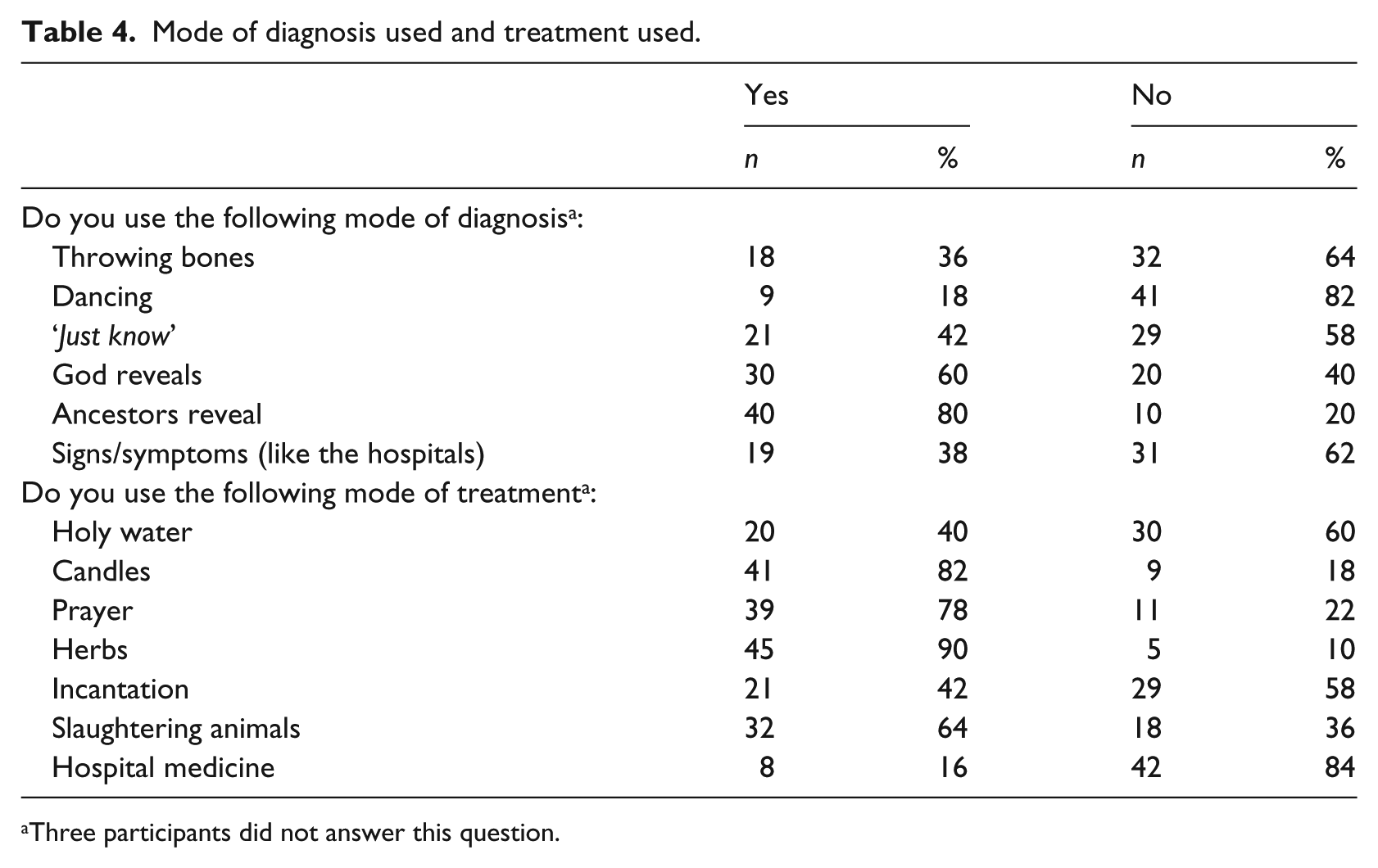
Three participants did not answer this question.
The procedure of healing
Diagnosis and treatment in traditional healing were described by participants as beginning with the healer first burning impepho and candles that were placed on a mat. This was done to connect with their own ancestors and sometimes with the client’s ancestors. Participant 2 described this as ‘enter[ing] the ancestor way’. The ancestors would then reveal to the healer what was wrong with the client and what treatment may be required. The healer would communicate this to the client and/or the client’s family who would then evaluate the feedback and make a decision on which direction to take. If the client did not agree with the TH’s report, he or she left, sometimes without paying for the services received. If the client accepted the report of the TH, treatment could begin with the healer suggesting specific mode/s of treatment.
The influence of God and the church
Chi-square tests indicated that the specific church that participants attended shaped how they referred to themselves (e.g., spiritualist, healer, or sangoma) and their modality of treatment. For example, participants who attended an African Initiated Church (Ranger, 2007) were more likely to refer to themselves as ‘Spiritualists’ compared to participants who attended a Mainline Christian Church, χ(df = 2) = 9.84, p = .007. 5 In addition, participants who attended an African Initiated Church were statistically more likely to use holy water, χ(df = 2) = 10.86, p = .004, and candles, χ(df = 2) = 8.68, p = .013, than those who did not attend an African Initiated Church. A number of participants also made it clear that the process of treatment had to ‘open with prayer’ (Participant 17) and that ‘I can’t do nothing [sic] without God . . . God is always on top’ (Participant 1). In some cases, the lines between God and the ancestors appeared blurred: ‘Maybe God is with the ancestors’ (Participant 37).
The relationship between self-identification and mode of diagnosis and treatment
Chi-square tests also showed that how participants referred to themselves was related to their preferred modality of diagnosis. For example, participants who self-identified as a ‘Sangoma’ were more likely to ‘just know’ what was wrong with a client, χ(df = 1) = 1.03, p = .04, or to use ‘signs and symptoms’, χ(df = 1) = 5.54, p = .018, Fisher’s exact two-tailed p = .04, than participants who did not self-identify as ‘Sangoma’.
Chi-square tests indicated that how participants self-identified was also related to mode of treatment. Participants who self-identified as ‘Sangoma’ were more likely to use incantations during treatment, χ(df = 1) = 8.37, p = .003, Fisher’s exact two-tailed p = .01, than participants who did not self-identify as ‘Sangoma’. Participants who self-identified as ‘Spiritualist’ were more likely to use holy water during treatment, χ(df = 1) = 15.16, p < .00, Fisher’s exact two-tailed p < .00, than participants who did no self-identify as ‘Spiritualist’. The use of candles and prayer were not significantly related to any specific self-identification.
Perceived working relationship with Western hospitals
The majority of participants reported that they often referred clients to the nearest medical hospital/clinic (n = 39, 78%). Only eight participants (16%) stated that they did not find it necessary to refer clients to a medical provider but stated that they would if they found it to be necessary. Most participants referred clients to a hospital if they had an illness that they did not treat (n = 37, 74%). This included illnesses such as cancer, HIV/AIDS, TB, and clients who were too weak to receive strong traditional medicines. Some participants were clear that ‘Before I do anything for you, go to the clinic’ (Participant 9). The majority liked working with hospitals and medical providers (n = 33, 66%). Participant 21 said: ‘I do trust the doctors because they also treat me right’. However, some had negative experiences of working with hospitals. For example, Participant 41 described how a doctor asked her patient: ‘Are you using the kaffir 6 medicine now?’ Another stated that talking about working with the medical doctors was ‘hurtful, this is hurting, it is a hurting place’ (Participant 47).
Discussion
Given the widespread use of traditional medicine for mental health care among Black South Africans, it is important to explore the self-identification, training, and practices of THs. We also explored THs’ perception of collaboration with Western health care institutions (hospitals, clinics). Increasing our understanding of the training practices of THs and investigating their treatment modalities for mental illness, and how this may be related to self-identification, is important. Participants in our study reported receiving the calling to become healers at different stages in their lives. Similarly, the length of time they spent in training was varied. However, the training for the majority of participants followed the same sequence. This suggests that their training was fairly standardized.
Working as a healer and the working relationship with Western hospitals
The majority of participants stated that they treated both mentally and physically ill clients; however, those participants who self-identified as spiritualists were more likely to report that they treated mental illness. The latter finding echoes the importance of more specified and detailed research required into the self-identification of THs (van der Watt et al., 2018) to better understand THs role in mental health provision in South Africa.
While participants perceived their clients to be generally satisfied with their treatment, evidence from other studies indicates that clients delay accessing Western medical and mental health services when THs are the first providers that they consult (Burns & Tomita, 2015; Sorsdahl, Stein, & Flisher, 2013). From a biomedical perspective, and if the client feels the treatment provided by THs is not efficacious, this can be problematic in mental health treatment since delayed treatment-seeking behaviour is a major contributory factor to poor outcomes among people living with mental illness (Burns & Tomita, 2015). For example, what the medical paradigm defines as mental illness such as schizophrenia, the traditional paradigm defines as ‘Xhosa illness’ (e.g., amafufunyana) for which traditional treatment is sought (Schierenbeck et al., 2018). This reiterates the importance of encouraging collaboration between mainstream providers and THs who have stronger appeal among people who have traditional and religious explanatory belief systems. Cultural beliefs often have a strong influence on health behaviours and culture-bound syndromes (Chilale, Silungwe, Gondwe, & Masulani-Mwale, 2017). These systems are dominant in African culture and the goal should be to determine how medical and traditional culture systems can work together, and to minimize the dominance of one over the other.
The majority of participants stated that they often referred clients to the nearest hospital/clinic, especially for illnesses that they could not treat such as tuberculosis and HIV/AIDS. This suggests a willingness to collaborate with medical health providers despite the inherent tensions between THs and medical paradigms (Schierenbeck et al., 2018).
Reluctance to provide details
Participants appeared reluctant to provide more detailed information regarding their training and treatment methods. For example, while they mentioned the use of herbs, the exact herbs were not named because ‘that’s a secret’ (Participant 49) and ‘you will not understand’ (Participant 48). It was not clear whether the participants’ reluctance was related to discomfort with the setting, a university office, or discomfort with talking to the ‘white doctors’ (Participant 21). In addition, there may have been an inherent hesitation based on cultural beliefs that TH skills are handed to selected people by the ancestors. Talking about it may have then been perceived as breaching this trust that was handed down to them. Previous research conducted among healers in three countries (Nigeria, Ghana, and Kenya), with a similar colonial history to South Africa, alluded to the persistence of mistrust between the traditional and the medical spheres (van der Watt et al., 2017).
Findings should be interpreted with caution. The interviews were not video/audio recorded, and this limited our ability to capture the richness of the data. Furthermore, the sample size limits the generalizability of our quantitative findings although it is more than adequate for thematic analysis. The current study has been duplicated in the Eastern Cape Province, South Africa, allowing for quantitative data from both sites to be combined and compared. This will likely enhance the generalizability of the quantitative data, which, to our knowledge, will be the first mixed-methods comparative study of isiXhosa-speaking THs in the Eastern and Western Cape Provinces. Finally, the interviews were conducted in a university setting, a location not ideal in the present context. It may have highlighted the power imbalance between the interviewers and interviewees. Since we anticipated the possibility of this occurring, a member of the participants’ community was part of the research team and present at all interviews. However, it is possible that some participants were not comfortable talking to the ‘white doctors’ (Participant 21) who were not from their community. Future researchers should attempt to conduct the interviews in a neutral setting, ideally by a community member.
Conclusion
The findings of this study provide an understanding of the training, self-identification, and practices of isiXhosa-speaking THs in the Western Cape and their collaboration with medical providers. The training and process of becoming a TH appears to be fairly similar for all THs, and their self-identification was statistically associated with different diagnoses and treatment modalities. However, participants appeared reluctant to elaborate on the details of their treatment approaches. It is possible that mutual mistrust between THs and the biomedical field may have prevented this from occurring. Future studies should focus on spending substantial time establishing trust between researchers and participants. Conducting the research at a location in which participants feels more comfortable may also support their ability to talk freely about their experiences. A more in-depth exploration of the varying forms and meaning of self-identification and its association with mode of diagnoses and treatment is warranted to better understand the work of THs.
Footnotes
Acknowledgements
The authors would like to thank all the participants who took part in the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The current research was funded by the South African Research Chairs Initiative in PTSD hosted by Stellenbosch University, funded by the DST and administered by the NRF (Tier-1-level Research Chair), and by research grant from the Chicago School of Professional Psychology (Washington DC Campus) funds received by Priscilla Das-Brailsford.