
Abstract
Previous research into the relationship between religion and physical and mental health discloses scientific puzzles concerning causality and linearity, demonstrating the need to clarify underlying pathways. Therefore, we analysed a representative sample of the general Dutch population (n = 4659), simultaneously testing four underlying pathways: (1) health advantages due to social benefits of religious participation; (2) religious prohibitions encouraging temperance; (3) direct physiological benefits of religious practice; (4) health benefits of certainty on existential matters. Regarding the first pathway, we found no direct association between church attendance and health. Regarding the second pathway, we found that church attendance is indirectly associated with better physical health through less smoking. However, this positive indirect association is counterbalanced by a negative indirect association between church attendance and physical health through less alcohol consumption, which we found to be positively associated with physical health. Regarding the third pathway, we unexpectedly found a negative association between praying and physical and mental health. Although our cross-sectional design precludes determination of causality, this negative association may be attributable to praying induced by adversity. Regarding the fourth pathway, we found a curvilinear association between religious belief and mental health, with convinced believers and convinced non-believers both having better mental health than those uncertain about the existence of God and an afterlife. However, we found no such association for physical health. Considering the percentage of explained variance, we found no substantial association between religion and health in the Netherlands, a secularized society with excellent healthcare access.
Introduction
Since the turn of the century, many studies have demonstrated a positive relationship between religiosity and health, evaluating different dimensions of religion (religious participation, religious education, praying) and of health (lower mortality rates; fewer functional limitations; less depressive symptoms; better mental health; better self-rated health; less long-term health problems; lower odds of heart attack, stroke, diabetes and cancer; Ahrenfeldt et al., 2017, 2019; Assari, 2013; Ellison et al., 2000; Gillum et al., 2008; Koenig et al., 2024; Morton et al., 2017; Nicholson et al., 2009; Opsahl et al., 2019). Although this relationship has been studied in great detail, two scientific puzzles remain, concerning its causality and linearity. Concerning causality, three possible causal relationships are mentioned in the literature. The first is a causality from religion to health in a positive way: religiosity contributes to better mental and physical health; a claim that is supported by many longitudinal studies (Ahrenfeldt et al., 2017, 2019; Ellison et al., 2000; Gillum et al., 2008; Opsahl et al., 2019). The second is a causality from health to religion in a positive way, with ill health potentially preventing religious involvement (Immerzeel & van Tubergen, 2013; Nicholson et al., 2009) or with depression potentially leading to discontinuation of religious service attendance (Opsahl et al., 2019). The third is a causality from health to religion in a negative way. Norris and Inglehart (2004) hypothesize in their existential security theory that feelings of vulnerability to physical, societal and personal risks are major factors inducing religiosity. They argue that both the experience of ego-tropic risks (direct threats to oneself and one’s family) and of socio-tropic risks (threats to one’s community) fuel religiosity and that people raised under relatively secure (thus, also relatively healthy) conditions tolerate more ambiguity and have less need for the absolute and predictable rules provided by religion. In support of this claim, Immerzeel and van Tubergen (2013) found in a longitudinal European study that healthier people have lower religiosity. Moreover, in a longitudinal international study, van Ingen and Moor (2015) found that an increase of life expectancy at birth causes a decrease of church attendance.
Concerning linearity, most previous studies interpret the relationship between religion and health as linear. However, some scholars, assuming a causality from religion to health, pose that the relation is curvilinear, suggesting that committed religious believers and committed atheists both have health benefits compared to people with weak religious commitment. Such curvilinear relationships have been found in empirical research on the relationship between religiosity and physical and mental health (Baker et al., 2018; Brammli-Greenberg et al., 2018), mental health (Gontijo et al., 2022), subjective well-being (Galen & Kloet, 2011; Mochon et al., 2011), distress (Ross, 1990), depressive symptoms (Eliassen et al., 2005) and death anxiety (Spitzenstätter & Schnell, 2022; Wink & Scott, 2005). This curvilinear relationship has been ascribed to the existential certainty provided by a strong commitment to one’s belief system, whether religious or nonreligious, which provides health benefits (Fortuin, 2021; Jimenez et al., 2020).
Scientific puzzles regarding causality and linearity can be addressed when the underlying pathways for the relation between religion and health are clarified. Therefore, the aim of this study is to advance our knowledge concerning such pathways by incorporating different potential pathways in a single model, using recent, high-quality, extensive and representative research data on religion and health in the Netherlands. This study addresses the following research question: What is the relationship between religion and physical and mental health in the Netherlands, and to which pathways can it be attributed? For three reasons, the Netherlands are a promising setting for research into this relationship. First, most incontestable evidence of a positive relationship between religiosity and health has been gathered in US studies, while studies in the more secularized European context have been found to be contradictory (Lalive d’Epinay & Spini, 2004), although more recent large-scale European studies confirm the positive relationship found in the United States (Ahrenfeldt et al., 2017, 2019; Nicholson et al., 2009; Opsahl et al., 2019). Still, the less conclusive evidence gathered in European countries indicates the need to study the underlying pathways especially in this context. Second, the occurrence of a curvilinear relationship between religion and health can only be investigated if the study sample contains sufficient nonreligious people, which is certainly the case in the Netherlands (Kregting et al., 2018). Third, data from the Netherlands preclude associations between religion and health due to direct influences on healthcare access, which could complicate insight into the more subtle pathways we evaluate. The Netherlands offers excellent access to healthcare, performing considerably better than the average of the 38 member countries of the Organisation for Economic Co-operation and Development (OECD, 2023) regarding healthcare service coverage and coverage of healthcare expenditure by compulsory prepayment. Therefore, Dutch people do not depend on religious organizations for availability or affordability of healthcare.
Theory and hypotheses
Because a multitude of empirical studies reports a positive relationship between religion and health, our hypotheses are grounded in the assumption that such a positive relationship does indeed exist. Although many pathways explaining this positive relationship are mentioned in the literature (Koenig et al., 2024; Park & Slattery, 2013), in our view, four of them are the most prominent (Ellison et al., 2000; Fortuin, 2021; Idler, 2004; Jimenez et al., 2020; Koenig, 2002; Morton et al., 2017): social support, temperance, physiological benefits and existential certainty.
Social support
The first pathway attributes the relationship between religion and health to enhanced social integration due to religious participation. Social support networks are generally associated with better physical and mental health (Holt-Lunstad et al., 2010; Krause, 2006). Fellow members of a religious community can assist each other emotionally, practically and spiritually (Krause, 2006, pp. 506–508). Membership of a religious community increases the likelihood that monitoring for health problems will occur, health problems are detected sooner and compliance with medical treatment is stimulated. Moreover, support provided by religious sources appears to be more satisfying and more resilient than support from secular sources (Koenig, 2002, pp. 15, 21–22). As a major driving force behind religious social interaction, religious service attendance is proposed as the indicator for the first pathway. Frequency of religious service attendance is associated with lower mortality rates (Ellison et al., 2000; Gillum et al., 2008), better self-reported health (Nicholson et al., 2009), better mental health (Assari, 2013), lower odds of limitations in activities and depressive symptoms (Ahrenfeldt et al., 2017; Opsahl et al., 2019), and lower odds of heart attack, stroke, diabetes and cancer (Ahrenfeldt et al., 2019), leading to the following hypothesis:
Hypothesis 1: Religious service attendance is associated with better physical and mental health.
Temperance
The second pathway attributes the relationship between religion and health to religiously motivated temperance. When people follow their religion, they will encounter religious prohibitions stimulating temperance and discouraging substance use. These prohibitions are probably conveyed most insistently during religious services. Following these prohibitions induces a healthier lifestyle, thereby improving physical and mental health. Indeed, a nationwide US survey indicates that religious service attendance is associated with lower odds of alcohol, tobacco and cannabis use disorder (Livne et al., 2021). Moreover, a longitudinal analysis of data collected between 2004 and 2015 among Europeans aged 50 years and older participating in the Survey of Health, Ageing and Retirement in Europe (SHARE) shows that religious service attendance is negatively associated with drinking and smoking (Ahrenfeldt et al., 2018). Furthermore, a decrease of substance use has a positive impact on physical and mental health (Patrick et al., 2020). Therefore, we propose the following hypothesis:
Hypothesis 2: Substance use mediates the relationship between religious service attendance and physical and mental health, whereby religious service attendance is associated with lower use of alcohol, drugs and nicotine, and lower use of alcohol, drugs and nicotine is associated with better physical and mental health.
Physiological benefits
The third pathway links the relationship between religion and health to physiological processes (Koenig, 2002, pp. 22–25). Engagement in religious practices such as praying, meditation and religious services provides direct physiological benefits through reduction of stress hormones, lowering of heart rate and blood pressure and increased effectiveness of the neuroendocrine and immune system (Idler, 2004, pp. 29–30; Koenig, 2002; Krause, 2006, p. 502, Masters et al., 2023, pp. 336–337). Although collective religious practice (e.g. religious service attendance) may provide physiological benefits as well, this practice also provides social benefits (conform Hypothesis 1) and it may influence substance use (conform Hypothesis 2), which blurs the empirical insight into the influence of physiological processes. Therefore, in this study individual religious practice in the form of prayer is used as an indicator for the third pathway. Experimental designs indicate that praying is associated with reduced pain and healthier cardiovascular responses to stress (Masters et al., 2023). Moreover, longitudinal studies indicate that praying or meditating is associated with positive affect, emotional processing and emotional expression among American adolescents (Chen & VanderWeele, 2018) and that praying is associated with lower mortality among Americans with a chronic illness (Ironson & Ahmad, 2024), with better cognitive function, less sleep disturbances and lower neuropsychiatric symptoms among older Americans with dementia (Britt et al., 2022), with better cognitive function among older European men (Ahrenfeldt et al., 2024), and with less hopelessness and less suicidal thoughts among older Europeans (Opsahl et al., 2019). Finally, praying is inversely associated with several Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) anxiety disorders (Hodge et al., 2022). Therefore, we propose the following hypothesis:
Hypothesis 3: Praying is associated with better physical and mental health.
Existential certainty
The fourth pathway attributes the relationship between religion and health to the provision of frameworks of meaning, thereby enhancing the certainty people experience concerning existential matters. The term ‘existential certainty’ was posed by Ellison (1991, p. 82), referring to ‘strong beliefs regarding matters of ultimate concern’. Perceived certainty concerning existential questions benefits mental health due to anxiety reduction (Ross, 1990; Wink & Scott, 2005). Moreover, when their beliefs help people relieve their existential concerns, this may benefit their health perceptions, choices and coping, thus also improving their physical health (Jimenez et al., 2020). Previous research demonstrates that religious doubt is associated with less well-being (Ellison, 1991; Krause, 2015). Moreover, people with weak religiosity were found to have lower mental health (Gontijo et al., 2022), more psychological distress (Ross, 1990), more depression (Eliassen et al., 2005), lower well-being (Galen & Kloet, 2011; Mochon et al., 2011) and worse physical and mental health (Baker et al., 2018; Brammli-Greenberg et al., 2018) than people with strong or no religious belief. Therefore, while the previous pathways predict a positive linear relationship between religion and health, this fourth pathway predicts a curvilinear relationship, whereby convinced believers and convinced non-believers both have better health than people who are uncertain about the existence of God and an afterlife. In this study, we conceive existential certainty as an individual’s certainty on the question of whether there is a God or higher being and on the question of whether there is an afterlife, since both are important matters of ultimate concern. This should not be confused with the concept of existential security as proposed by Norris and Inglehart (2004, p. 4), which refers to ‘the feeling that survival is secure enough that it can be taken for granted’. Therefore, we propose the following hypothesis:
Hypothesis 4: Convinced believers and convinced non-believers have better physical and mental health than people who are uncertain about the existence of God and an afterlife.
For each pathway, we have selected the most obvious religious variable, based on relevant scientific literature. However, these religious variables interact with health through intermediate variables that were not measured. For the first pathway, we assume that church attendance is associated with social support, which is associated with better health. For the second pathway, we assume that church attendance is associated with following religious prohibitions, which is associated with lower substance use, which is associated with better health. For the third pathway, we assume that praying is associated with reduced stress levels, which is associated with better health. Finally, for the fourth pathway, we assume that existential certainty is associated with lower anxiety, which is associated with better health. Existential certainty is the only pathway with theoretical grounds for a curvilinear relationship; therefore, we only evaluate curvilinear associations between belief in God and an afterlife and physical and mental health.
Control variables
We control for religious denomination, because previous research indicates that it may influence the relationship between religion and substance use, especially regarding alcohol consumption (Michalak et al., 2007). Based on previous research we expect health to be associated with gender, age, educational level, income and marital status (Gobbens & Remmen, 2019) and with migration background (Nazroo, 2003). Therefore, these factors are also added as control variables.
Methods
Sample
In this article, we make use of data of the LISS (Longitudinal Internet studies for the Social Sciences) panel administered by Centerdata (Tilburg University, The Netherlands). The panel consists of approximately 7500 individuals and is based on a large representative sample of people of 16 years and older drawn from the general Dutch population by Centerdata and Statistics Netherlands. All respondents have agreed to the LISS informed consent procedure. Respondents participated in both the LISS Core Studies on Health (wave 15, collected in November and December 2022; response rate 83%) and on Religion and Ethnicity (wave 15, collected in August and September 2022; response rate 85%). The control variables gender, age, educational level, income, marital status and migration background originate from the dataset with panel members’ background variables (October 2022; background variables are registered for all panel members). 1 Our sample is cross-sectional. Therefore, we only express our results in terms of associations, instead of (causal) relations.
Measures
Dependent variables
For this study, we constructed a new scale to assess physical health. The initial scale contains 23 items describing activities that are scored on a 5-point scale ranging from 1 (without any trouble) to 5 (not). These were tested in a principal axis factoring factor analysis with oblique (oblimin) rotation. Initial factor analysis and reliability runs indicated that two items (‘shopping’ and ‘dressing and undressing’) had to be removed because they loaded high on two factors, one item (‘sitting for around two hours’) had to be removed because it lowered the reliability of the first factor and four items (‘taking medicines’, ‘reading a map to find your way in an unfamiliar area’, ‘taking care of financial affairs’ and ‘picking up a small coin lying on the table’) had to be removed because they lowered the reliability of the second factor. Removal of these items led to the final scale with 16 items. A principal axis factoring factor analysis (n = 5818) with oblique rotation (oblimin) indicates that two factors have eigenvalues over Kaiser’s criterion of 1 and together explain 69.93% of the variance. The scree plot shows inflexions that justify retaining two factors. The Kaiser–Meyer–Olkin measure (KMO = .96) verifies the sampling adequacy (‘marvelous’ according to Hutcheson & Sofroniou, 1999, p. 225) and all KMO values for individual items exceed .93, which is well above the acceptable limit of .5 (Field, 2024, p. 848). Bartlett’s test of sphericity is significant (p < .000). Table 1 shows the factor loadings. The items that cluster on the same factor indicate that factor one represents limitations in physical agility and strength (LPAS) and factor two represents limitations in performance of daily activities (LPDA). These factors have a strong positive correlation (factor correlation = .66). Reliability of the LPAS subscale (Cronbach’s α = .94) and the LPDA subscale (Cronbach’s α = .93) is very good (DeVellis, 2017, pp. 136–137). Scale scores were calculated as the mean of individual items and scores were given to all respondents who had a valid score on at least four of the nine items. After that, scale scores were reversed so that a higher value indicates high physical agility and strength (PAS) and high performance of daily activities (PDA). After this reversal of scores, the scale no longer evaluates limitations but abilities. Therefore, the factors were renamed into PAS and PDA. To evaluate physical health, in this study, we used the PAS subscale solely, because this construct most directly reflects physical health, while the PDA scale includes items that reflect physical health less directly (such as telephoning and preparing a hot meal).
Rotated factor loadings of the limitations in physical agility and strength (LPAS) and limitations in performance of daily activities (LPDA) subscales. Factor loadings over .50 appear in bold (n = 5818).

Mental health was examined using the Dutch version of the Mental Health Inventory (MHI-5), one of the subscales of the Short Form-36 (SF-36), a measure that has been used widely in surveys of mental health, general health, and quality of life (Hoeymans et al., 2004). The MHI-5 contains five items and has a 6-point response scale coded from 0 to 5, such that a higher value indicates better mental health (Cronbach’s α = .88; n = 4871). The MHI-5 score is calculated by summing up the individual values and multiplying them by four, so that the final score ranges from 0 (minimal mental health) to 100 (excellent mental health; Hoeymans et al., 2004).
Independent variables
Religious service attendance and praying were both evaluated by a single-item measurement (‘aside from special occasions such as weddings and funerals, how often do you attend religious gatherings nowadays?’ and ‘aside from when you attend religious gatherings, how often do you pray?’) and were both scored on a 6-point scale ranging from 1 (every day) to 6 (never). Scores were recoded so that a higher value indicates higher frequencies of religious service attendance and prayer. To evaluate religious belief, we distinguished six groups of respondents, based on the certainty and nature of their belief in God and an afterlife. We situate these groups on a ‘religious belief’ spectrum from nonreligious to religious in the following way: the first group, ‘nonreligious certain’, consists of respondents who neither believe in a life after death nor in God or a higher power. The second group, ‘nonreligious with doubt’, consists of respondents who do not believe in an afterlife and doubt whether God exists (i.e. they do not know if God exists, believe in God at some moments but do not believe in God at other moments or believe in God, although they have their doubts). It also consists of respondents who do not know whether there is an afterlife but do not believe in God or a higher power. The third group, ‘uncertain’, does not know whether there is an afterlife and doubts whether God exists. The fourth group, ‘religious with doubt’, consists of respondents who believe in a life after death but doubt whether God exists. This group also consists of respondents who do not know whether there is an afterlife but who do believe in God or a higher power. The fifth group, ‘ambiguous certain’, is characterized by certainty concerning existential matters that is partly religious and partly nonreligious. This group consists of respondents who believe in a life after death but not in God or a higher power and of respondents who do not believe in life after death but believe in God or a higher power. Finally, the sixth group, ‘religious certain’, believes both in the existence of God or a higher power and in an afterlife. As we expect that being uncertain is associated with lowest health, the third group (‘uncertain’) is taken as reference.
Mediating variables
For alcohol consumption, a measure was constructed based on the number of days during the past week that respondents consumed alcohol, multiplied by the number of alcoholic drinks they consumed on the day they drank most. 2 Drug use was evaluated by the number of times respondents used sedatives, soft drugs, XTC, hallucinogens, hard drugs and/or laughing gas during the past month. 3 Smoking was indicated by the average number of cigarettes, pipes and cigars plus the millilitres of e-cigarettes smoked daily. 4
Control variables
Religious denomination of respondents was categorized into six groups: religiously unaffiliated respondents (the reference group), Catholics, Protestants (consisting of both mainline and small Protestant denominations), other Christian denominations (including Eastern Orthodox Christians), Muslims and different religious groups (Hinduism, Buddhism, Judaism, and other non-Christian faith). Gender was determined as female (0) or male (1). Age was measured as scale variable. Educational level was determined by the level of education on a scale ranging from (1) ‘primary school’ to (6) ‘university’. Income was measured as personal net monthly income in euros. 5 Regression analyses were performed with the logarithm of income. Marital status was measured in four groups: married (the reference group), separated or divorced, widowed and never been married. To evaluate the influence of living together while never having been married, we divided the latter group into singles (never been married and not living together with a partner) and cohabitants (never been married but living together with a partner). Migration background was evaluated as 0 (Dutch background) or 1 (first- or second-generation foreign background).
Models and assumptions
We performed two hierarchical linear regression analyses predicting physical health and mental health respectively, in which the simultaneous influence of the four proposed pathways was evaluated. In both analyses, three models were evaluated based on forced entry of predictors. In the first model, religious service attendance, praying and religious belief were entered as predictors. In the second model, use of alcohol, drugs and smoking were added as predictors. In the third model, we controlled for religious denomination, gender, age, educational level, income, marital status and migration background. Based on the criteria presented by Sullivan et al. (2021) for a sample size of 4871, 24 predictors and an α of .05, the cut-off value of the Mahalanobis distance is 65.43. The first regression run indicates that 212 cases have a Mahalanobis distance exceeding the cut-off value. These 212 cases include all respondents who are Muslim (n = 76), belong to different religious groups (n = 47) or have a Christian denomination that is not Protestant or Catholic (n = 34), indicating that these respondents do not have the same characteristics concerning the association between religion and health. To correct for cases with undue influence, these 212 cases were removed from the dataset and regressions were recalculated. After this correction, the sample size decreases with 4%; however, it is still adequate for our analyses (4659 respondents with widespread groups regarding religiosity). 6 Because all respondents with a non-Christian religion have been removed from the dataset, after this correction, the variable religious service attendance becomes church attendance. Table 2 shows the sample characteristics after removal of cases with undue influence.
Composition of the sample (n = 4659).

In our final regressions, variance inflation factors (VIF) of predictors are below 2.52, which is well below the cut-off value of 10 (Meuleman et al., 2015). Moreover, the average VIF (1.59) is not substantially greater than 1, indicating that there are no problems with multicollinearity (Field, 2024, p. 441). Casewise diagnostics indicate that for both regression runs, 95.30% of cases have standardized residuals within ±1.96, which is very close to the expected 95%. The histogram and the p-p plot of the regression standardized residual for physical health (PAS) shows substantial deviation from normality (skewness = −2.57 and kurtosis = 9.87). Moreover, the partial regression plots for physical health (PAS) show funnelling, indicative of heteroscedasticity. The histogram and the p-p plot of the regression standardized residual for mental health (MHI-5) shows much less deviation from normality (skewness = −.83 and kurtosis = .64). However, the partial regression plots for mental health (MHI-5) also show some funnelling, indicative of heteroscedasticity. Therefore, for both regression analyses 3000 bootstrap samples were used to determine the 95% Bias Corrected accelerated (BCa) confidence intervals and significance levels of B, which do not rely on assumptions of normality or homoscedasticity (Field, 2024, p. 467).
In Tables 3 and 4, both the B values and the β values are reported; the B values give insight in the bootstrapping results and the β values allow for mutual comparison of the different predictors. However, if the significance levels of both values differ, the B values based on bootstrapping are leading, since they are most reliable. None of the confidence intervals of the B values that are significant at p < .050 cross zero, giving confidence that for these predictors, there is a genuine association in the population.
Linear regression analyses for physical health (PAS) with 95% BCa confidence intervals of B based on 3000 bootstrap samples reported in brackets.

p < .05. **p < .01. ***p < .001.
Linear regression analyses for mental health (MHI-5) with 95% BCa confidence intervals of B based on 3000 bootstrap samples reported in brackets.

p < .05. **p < .01. ***p < .001.
To evaluate to what extent substance use mediates the association between church attendance and physical and mental health (conform hypothesis 2), we used the PROCESS tool, version 4.2, by Andrew F. Hayes (2022). First, we ran model 4 with physical health as dependent variable, church attendance as predictor variable, alcohol consumption, drug use and smoking as parallel multiple mediators and praying, religious belief, religious denomination, gender, age, educational level, income, marital status and migration background as covariates. Second, we ran the same model with mental health as dependent variable. For the indirect effects, bias corrected and accelerated confidence intervals were calculated with 5000 bootstrap samples.
Results
Table 3 shows the results of the regression analyses for physical health (PAS). It demonstrates that, according to model 1, church attendance is associated with better physical health and the same applies to model 2, after controlling for substance use. However, in model 3, which controls for background variables, the association between church attendance and physical health becomes non-significant (considering the p value of B calculated with bootstrapping). In models 1 and 2, praying is associated with worse physical health and this association remains after controlling for background variables in model 3, although at a lower level of significance (p < .05). There are hardly any associations between religious belief and physical health. Only in model 2 we find that, nonreligious Dutch people with doubt have worse physical health than Dutch people who are uncertain about existential matters. However, after controlling for background variables in model 3, this association becomes non-significant.
Regarding our nonreligious variables in model 3, alcohol consumption is associated with better physical health – which is unexpected and will be evaluated in the Discussion section – and drug use and smoking with worse physical health. In addition, men have better physical health than women, married people have better health than people who are separated or divorced, widowed or single, and physical health decreases with age and increases with the level of education. Finally, models 1 and 2 with religion and substance use barely explain any variation of physical health (1% and 2% respectively); only after adding our background variables in model 3, this explanation rises to a somewhat considerable level (13%).
Table 4 shows the results of the regression analyses for mental health (MHI-5). It demonstrates that, according to model 1, church attendance is associated with better mental health. However, after controlling for substance use and background variables (models 2 and 3), the association between church attendance and mental health becomes non-significant. In models 1 and 2, there is no significant association between praying and mental health. However, after controlling for background variables (model 3), we find a significant negative association between praying and mental health (p < .05). Concerning religious belief, according to model 1, we find that nonreligious certain people, nonreligious people with doubt and ambiguous certain people have better mental health than those who are uncertain concerning existential matters (the reference group). The same applies to model 2, after controlling for substance use. In model 3, after controlling for sociodemographic variables, religious certain people are added to the categories that have better mental health than uncertain people. This final model of analysis shows signs of curvilinearity: people at the lower end of the nonreligious-religious spectrum (the ‘nonreligious certain’ group) and people at the upper end of the nonreligious-religious spectrum (the ‘religious certain’ group) both have better mental health than uncertain people, the reference group, which falls in the middle of the nonreligious-religious spectrum (β’s are .05**). However, the curvilinearity is not perfect since the intermediate categories ‘nonreligious with doubt’ and ‘ambiguous certain’ differ from the reference category to almost the same extent (β’s respectively .06** and .04*) as the religious and nonreligious certain people, while the intermediate category ‘religious with doubt’ does not differ significantly from the reference category. In our final model, we also find that Protestants and Catholics have better mental health than religiously unaffiliated people (p < .05).
Regarding our nonreligious variables in model 3, drug use is associated with worse mental health. In addition, men have better mental health than women, non-migrants have better mental health than people with a migration background, married people have better mental health than people who are separated or divorced, single or cohabitant, and mental health increases with age. Finally, models 1 and 2 with religion and substance use barely explain any variation of mental health (1% and 3% respectively); only after adding our background variables in model 3, this explanation rises to a somewhat considerable level (10%).
The result of the mediation analysis for physical health is shown in Figure 1. According to this analysis, church attendance is associated with lower alcohol consumption and less smoking (conform our expectations), but it is not significantly associated with drug use. However, while smoking is associated with worse physical health (conform our expectations), alcohol consumption is associated with better physical health (contrary to our expectations). Due to this, there is a significant positive indirect association between church attendance and physical health through smoking but a significant negative indirect association between church attendance and physical health through alcohol consumption. Although drug use is associated with worse physical health, it is not significantly associated with church attendance and, therefore, has no significant indirect effect. The total indirect association between religious service attendance and physical health through substance use, which is the sum of the indirect associations through alcohol consumption, drug use and smoking, is non-significant. Figure 1 indicates a positive direct association between church attendance and physical health (B = .03*; p = .043), which corresponds with the B value of the regression analysis reported in Table 3 (model 3). However, Table 3 indicates a non-significant B value based on bootstrapping (p = .072). Since PROCESS calculates this p value without bootstrapping, which is less reliable, the level of significance of the B value indicated in Table 3 is leading.
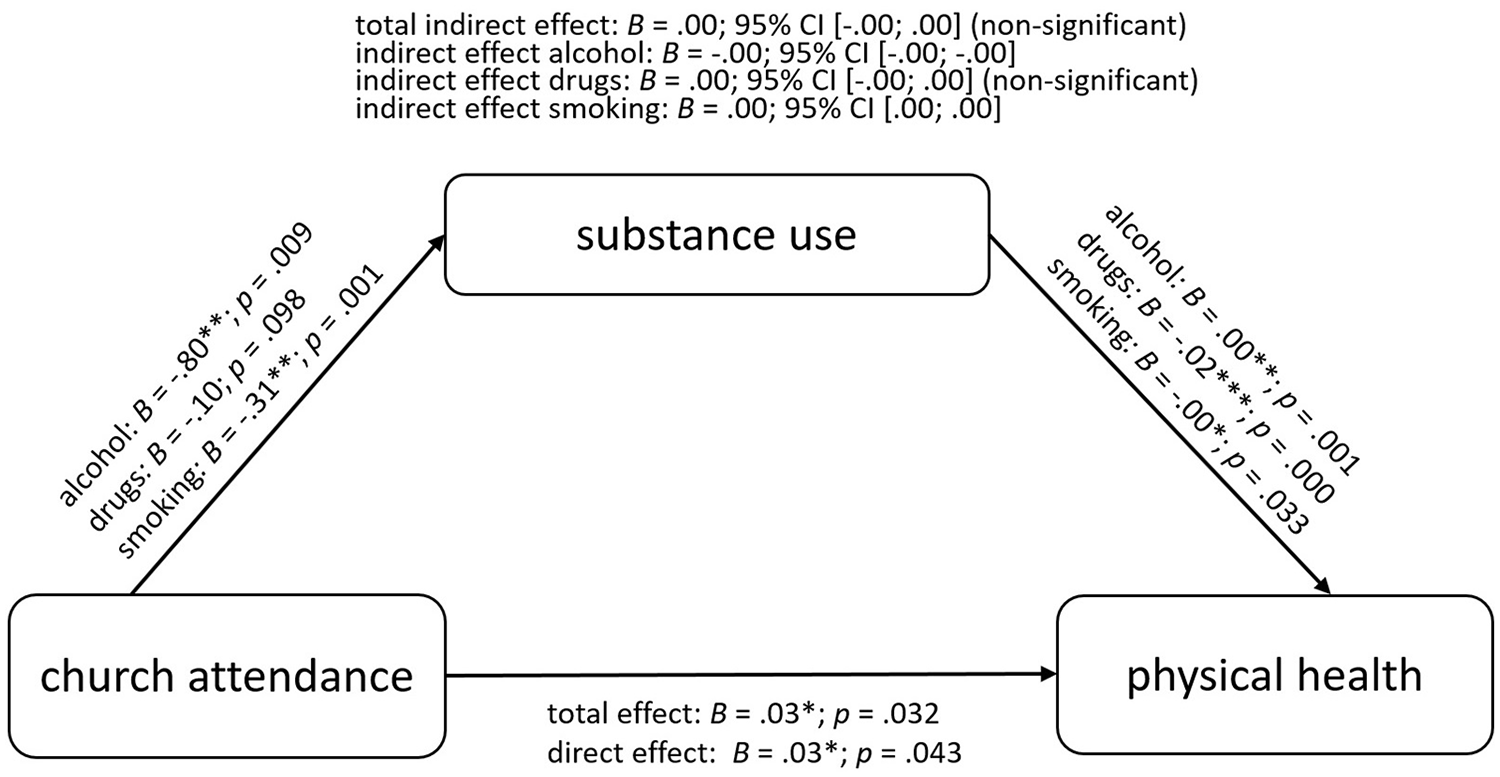
Mediation analysis performed with PROCESS model 4 (Hayes 2022, p. 622) of church attendance on physical health (PAS), mediated by substance use (n = 4659).
According to the mediation analysis for mental health in Figure 2 church attendance, again, is associated with lower alcohol consumption and less smoking (conform our expectations), but it is not significantly associated with drug use. However, both smoking and alcohol consumption are not significantly associated with mental health. Therefore, there is no significant indirect association between church attendance and mental health through alcohol consumption or smoking. Although drug use is associated with worse mental health, it is not significantly associated with church attendance and, therefore, has no significant indirect effect either. Consequently, the total indirect association between religious service attendance and mental health through substance use is also non-significant. Figure 2 also shows that there is no direct association between church attendance and mental health, which corresponds with the regression analysis reported in Table 4.
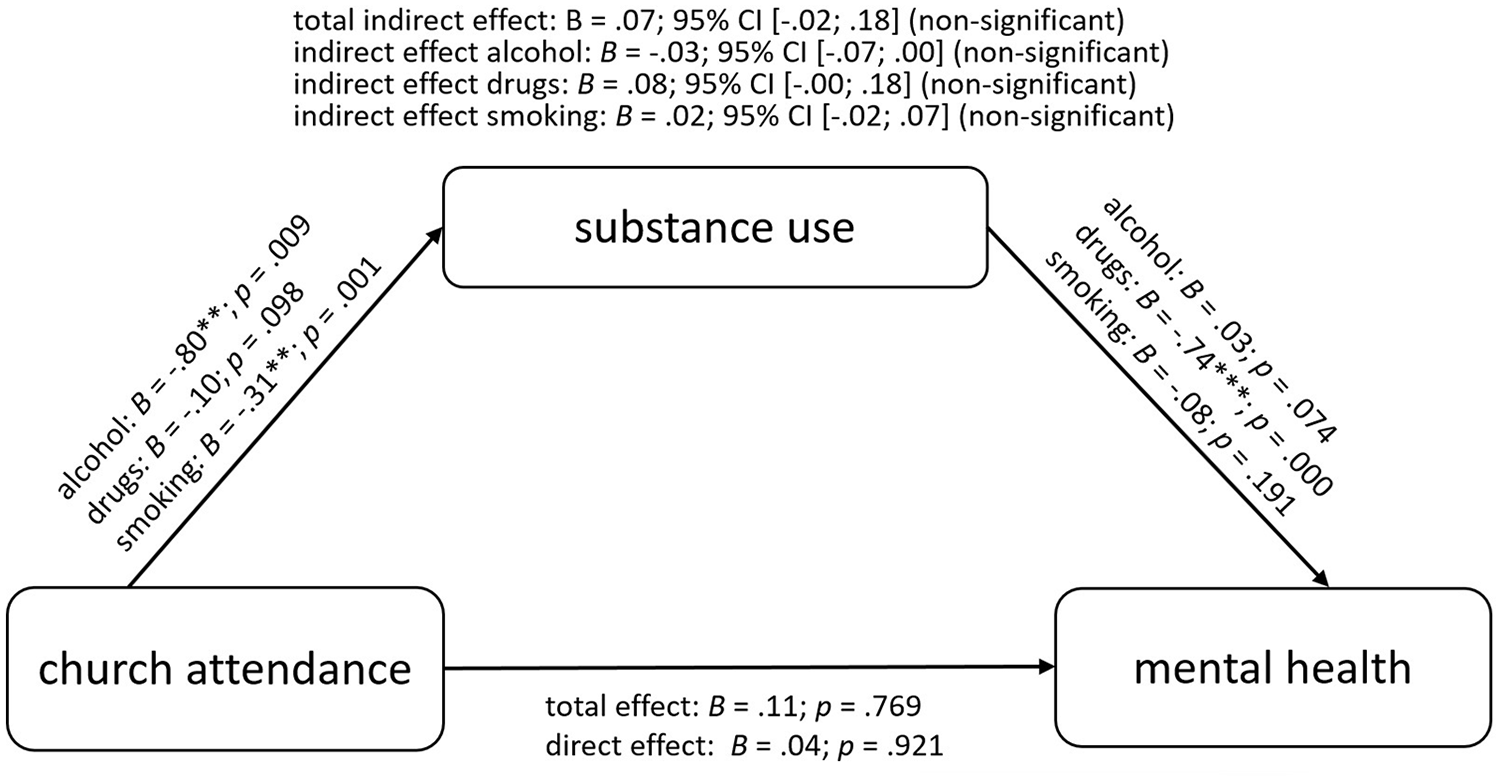
Mediation analysis performed with PROCESS model 4 (Hayes 2022, p. 622) of church attendance on mental health (MHI-5), mediated by substance use (n = 4659).
According to our final models of analysis (model 3 in Tables 3 and 4), our first hypothesis is refuted regarding both physical and mental health. The second hypothesis is only corroborated regarding smoking and physical health. Although alcohol consumption and smoking both mediate the association between church attendance and physical health, for smoking this mediation has the expected direction (a positive indirect association), but for alcohol consumption, it has the opposite direction (a negative indirect association). Our analyses refute the third hypothesis. We do find a significant association between praying and physical (p < .05) and mental health (p < .05), but it is negative instead of positive. Finally, our analyses partly corroborate the fourth hypothesis, but only regarding mental health.
Discussion
Below, we discuss our findings regarding the four pathways potentially underlying the association between religion and health.
Social support
The first pathway we evaluated ascribes the association between religion and health to the social benefits provided by religious participation. We did not find evidence of this pathway. This may be related to the COVID-19 pandemic. The questionnaire on religion was administered in August and September 2022, almost half a year after the termination of the last COVID-19 restrictions. Although in most religious communities the services had returned to normal at this time, the social benefits of religious participation may have lagged behind. Especially vulnerable people may still have been hesitant to be close to others (during but also after services when people drink coffee or tea together) because of health risks. This could imply that for those people, attending church did not have the social benefits it had before the COVID-19 pandemic.
A different indication for social benefits of religion regarding health, which was not formulated as an hypothesis, is found in a weak positive association between being Protestant or Catholic (instead of religiously unaffiliated) and mental health. This may be (partly) attributable to social benefits due to performing more secular voluntary work, which increases involvement in social networks. Two previous Dutch studies show that, after controlling for religious participation, being Catholic (Vermeer & Scheepers, 2012) and being Protestant (De Hart & Dekker, 2013) are positively associated with secular volunteering.
Temperance
The second pathway we evaluated is that of religious prohibitions inducing a healthier lifestyle due to encouraging temperance and discouraging substance use. Concerning this pathway, we only found a positive indirect association between church attendance and physical health through less smoking. The positive association we found between alcohol consumption and physical health is unexpected. It may be (partly) attributable to a positive association between physical activity (which benefits physical health) and alcohol consumption. Possible explanations that have been suggested for this positive association are that physical activity may create more social opportunities, which, in turn lead to increased alcohol use, individuals who consume alcohol may subsequently engage in physical activity to expend the additional calories (Dodge et al., 2017) or achieving goals during physical exercise may provide a ‘license’ to indulge in drinking afterward as a rewarding pathway (Shuval et al., 2022). Furthermore, people may reduce or quit drinking due to illness experiences (Liang & Chikritzhs, 2011) or decide not to start drinking due to poor health (Ng Fat & Shelton, 2012). Moreover, previous epidemiological studies demonstrate a J-shaped curve between alcohol consumption and relative risk of ischaemic heart disease, suggesting a cardioprotective effect of low to moderate alcohol consumption. However, such a cardioprotective association cannot be assumed for all drinkers, and most health effects of alcohol consumption are detrimental, such as the negative influence on several types of cancer and on injuries (Roerecke & Rehm, 2012). The combined associations between physical activity and alcohol consumption, between poor health and non-drinking, and between low to moderate alcohol consumption and lower risk of ischaemic heart disease may explain the positive association we found between alcohol consumption and physical health.
Physiological benefits
The third pathway we evaluated is that of religious practice contributing to physical and mental health by providing direct physiological benefits. Contrary to our expectations, we found a negative association between praying and physical and mental health. There are other studies that assessed the health benefits of prayer, but found a negative association instead. In a prospective longitudinal study among American adolescents, Chen and VanderWeele (2018) found that adolescents who prayed or meditated at least daily had more physical health problems than those who never prayed or meditated. Moreover, in a longitudinal analysis of SHARE data, Ahrenfeldt et al. (2019) found that praying is associated with higher odds of a heart attack and high cholesterol. In addition, analysing data from wave 1 of the SHARE, Hank and Schaan (2008) found that praying is associated with worse general health, worse physical health, more functional limitations and more depressive symptoms. Furthermore, in a longitudinal analysis of SHARE data with a random-effects model, Van Herreweghe and Van Lancker (2019) found that praying is associated with more depressive symptoms. However, comparison with a fixed-effects model suggested a selection effect: more depressed individuals are more likely to pray multiple times a day, and continue to do so, than less depressed respondents. This suggests a reversed causality, conform the existential security theory by Norris and Inglehart (2004): insecurity concerning one’s health drives religiosity. Indeed, some recent studies demonstrate that physical health threats induce prayer. A recent German study (Kanol & Michalowski, 2023) indicates that testing positive for a COVID-19 infection during the COVID-19 pandemic or having family members or friends who contracted the coronavirus (i.e. an ego-tropic health risk) are associated with more frequent prayer, while rising national infection rates (i.e. a socio-tropic health risk) are not. Also, an Italian study indicates that a corona contagion in one’s family is associated with increased praying (Molteni et al., 2021). Moreover, a recent US study shows that 60% of women diagnosed with metastatic breast cancer prayed more after their diagnosis, against 35% who reported no change and 5% who prayed less (Kraus, 2022). Although our cross-sectional design does not allow determination of causality, the negative association we found between praying and physical and mental health could be due to health problems inducing prayer.
As people can go through several causal prayer-health relationships, for example, by distress leading to prayer, then prayer decreasing distress, then thanking God for the decreased distress (Møller et al., 2020), relationships between praying and health are complex. The complexity of research into this relationship is intriguingly illustrated by different studies analysing SHARE data on praying and depression. Hank and Schaan (2008) found a positive relationship between praying and depression in a cross-sectional analysis of wave 1. Moreover, in a longitudinal ordinary least squares regression analysis using a random-effects model of 7719 respondents participating in wave 1 of the SHARE who were followed up in at least one wave between 2006 and 2013, Van Herreweghe and Van Lancker (2019) found that more frequent prayer is associated with more depression. However, using a fixed-effects model, they found that within-persons variations in praying behaviour were not significantly associated with depression. To make matters even more complicated, in a logistic regression analysis of 23,864 SHARE participants who participated in wave 1 and were followed up in at least one wave between 2006 and 2015, Opsahl et al. (2019) found that higher frequency of prayer is associated with lower odds of having no hopes for the future and of suicidal thoughts. Finally, Denny (2011) demonstrates that a linear regression analysis of wave 1 indicates a positive association between praying and depressive symptoms. However, instrumental variable analysis of the same data, which allows isolation of exogenous variation in prayer frequency, indicates that praying has a negative or zero effect on depression. These contradictory results demonstrate the need for sophisticated research designs and analysis techniques to unravel the interaction between praying and health.
Existential certainty
The fourth pathway we evaluated is that of health benefits due to certainty regarding existential matters. In accordance with previous studies (Baker et al., 2018; Brammli-Greenberg et al., 2018; Eliassen et al., 2005; Galen & Kloet, 2011; Gontijo et al., 2022; Mochon et al., 2011; Ross, 1990), we found a curvilinear association between religious belief and mental health: convinced religious believers (who believe in both the existence of God and an afterlife) and convinced non-believers (who neither believe in the existence of God nor in the existence of an afterlife) both have better mental health than people who are uncertain about the existence of God and an afterlife. However, we did not find such a curvilinear association between religious belief and physical health. Our study does not only demonstrate that strong belief systems, whether religious or nonreligious, are associated with better mental health, but it also provides new insights due to the way the different groups were defined, based on their extent of doubt concerning the (non-)existence of God and an afterlife. Of the seven aforementioned previous studies reporting curvilinear relationships between religiosity and mental health, only one (Gontijo et al., 2022) evaluated afterlife beliefs as an aspect of religiosity. 7 Our study contributes to this field of research by showing that not only certainty about the (non-)existence of God but also certainty about the (non-)existence of an afterlife should be considered when evaluating the relationship between religious belief and mental health.
Limitations
Our study has five limitations. First, although our analyses provide valuable insights into underlying pathways and curvilinearity, our cross-sectional setup does not allow determination of the causal direction of the found associations. A longitudinal setup with a panel would have been more appropriate, particularly considering the complexity of the relationship between prayer and health. Second, for each pathway, the religious variables that were measured interact with health through intermediate variables (social support, compliance with religious prohibitions, reduced stress levels and reduced anxiety) that were not measured, but assumed. Third, there may have been other underlying pathways for the relationship between religion and health that we did not evaluate. According to the terror management theory, worldviews do not only provide existential certainty, but they also offer culturally approved roles through which people can derive self-esteem (Jimenez et al., 2020). Indeed, previous research demonstrates that among European American and African American adolescents, self-esteem partially mediates the relationship between religiousness and depressive symptoms (Le et al., 2007); a pathway that we did not include in our analyses. Moreover, we included the pathway of religion tempering substance use in our mediation analyses, but did not account for the possible pathway of religion stimulating a healthier diet and more exercise (Ahrenfeldt et al., 2018; Morton et al., 2017). Fourth, the correction for cases with undue influence removed all people with a religious denomination other than Protestant or Catholic from the sample. Therefore, our study does not provide insight in the relationship between religion and health among, for example, the Dutch Muslims. Fifthly, the fact that data were collected only half a year after the cessation of COVID-19 restrictions complicates the evaluation of the social benefits of church attendance.
Conclusion
Based on our research results, we draw seven conclusions. First, we find that, based on our dataset and applied operationalizations and analyses, religion does not have a substantial association with physical and mental health in the Netherlands. The regression models that include religious and mediating variables (model 2) explain only 2% of the variance in physical health and 3% of the variance in mental health. Only after addition of sociodemographic variables, the explained variance increases to 13% of physical health and 10% of mental health. Second, we find a significant curvilinear association between belief in God and an afterlife and mental health. This suggests that it is not so much the content of their (religious or nonreligious) beliefs concerning God and an afterlife, but rather the certainty with which people hold them, that are associated with better mental health. Third, we find that church attendance is indirectly associated with better physical health through its association with less smoking. However, this positive indirect association is counterbalanced by a negative indirect association between church attendance and physical health through its association with lower alcohol consumption, which we found to be positively associated with physical health. Fourth, we find no indication that religion is associated with better health due to the social support provided by a religious community. However, the after-effect of COVID-19 restrictions may have countered the social benefits of church attendance. Fifth, we find that praying is associated with lower physical and mental health. Although this negative association suggests a reversed causality whereby physical and mental adversity induces praying, longitudinal panel research is needed to further investigate this relationship. Sixth, the setting of our research in the Netherlands, a highly secularized welfare state, allowed us to evaluate the social benefits of church attendance when people are not dependent on social networks provided by their religious community for availability or affordability of healthcare services and allowed us to demonstrate that both religious and atheist existential certainty are associated with better mental health. Moreover, the negative association we found between praying and physical and mental health suggests that even under conditions of relative social security, physical and mental health problems may still induce prayer. Seventh, the results of our research indicate interesting patterns that are well worthy of further research with similar high-quality panel data in other secular and also more religious countries.
Footnotes
Data availability statement
This work is original and has not been published elsewhere, nor is it currently under consideration for publication elsewhere. In this paper, we make use of data of the LISS (Longitudinal Internet studies for the Social Sciences) panel, administered by Centerdata (Tilburg University, The Netherlands), which can be accessed through https://www.dataarchive.lissdata.nl/study_units/view/1. Published LISS datasets can be downloaded free of charge for non-commercial scientific or policy-relevant purposes after signing a LISS data user statement. All respondents of the LISS panel have agreed to the LISS informed consent procedure.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.