
Abstract
Objective
Religious and spiritual factors in intimate partner violence have received increasing attention. But are such factors related to outcomes in violent relationships? The purpose of this study was to assess the relative impact of spiritual symptoms and religious coping on attitudinal/behavioral and clinical outcomes among women in violent relationships.
Methods
Adult women with a recent history of husband-to-wife physical abuse were recruited from six primary care clinics. Once enrolled, 200 subjects completed a baseline interview and daily assessment of level of violence, using the Interactive Verbal Response for 12 weeks. At the completion of the study, contact with each participant was attempted to determine whether she had either sought professional help or left the relationship. Three religious/spiritual variables were assessed at baseline—number of visits to a religious/spiritual counselor, religious coping, and severity of spiritual symptoms. Stepped multiple linear regression was used to explain factor-analyzed outcomes (coping and appraisals, hope and support, symptomatology, functional status, readiness for change, and medical utilization), adjusting for demographic, marital, childhood, mental health, and violence variables.
Results
After controlling for duration, severity and dynamics of violence, the use of spiritual resources, and the level of spiritual symptoms were associated with most attitudinal/behavioral and clinical outcomes, while religious coping was only associated with staying in the relationship.
Conclusions
Religious and spiritual factors were associated with most outcomes. Spiritual symptoms had a consistently negative effect on outcomes while use of spiritual resources had variable effects. Religious coping was only associated with refraining from leaving the relationship.
Introduction
The role of religious and spiritual factors in intimate partner violence (IPV) has received increasing attention in recent years. In terms of predictors of violence, a consistent correlate of husband-to-wife abuse is religious incompatibility between spouses.1,2 Generally, interfaith marriage and more religious involvement by the wife than the husband have been associated with abuse. In addition, the couples’ involvement in more conservative, “fundamentalist” faith traditions was also associated with IPV,3–7 although IPV can be linked to a lack of religious practice as well.8,9 However, Brinkerhoff et al. 10 found no association with religious denomination and a weak curvilinear relationship with church attendance. Such findings of violence and church attendance correlation may reflect different attitudes about the sanctification or importance of marriage. 11 Discordance in religious denomination, church attendance, and religious beliefs and practices may be symptomatic of a larger disparity in values between spouses. 12
Are religious or spiritual factors related to outcomes in violence? Religiousness has been linked to a variety of outcomes in family violence, including dysfunctional thoughts and behaviors,13,14 perceived strength, 15 self-esteem, 16 and depression and suicidality.17,18 Religious coping is a common approach to stressful life events,19,20 but a history of abuse correlates with reliance upon self rather than collaboration with God. 21 Abusive experiences in childhood have been linked to seeking spiritual support as an adult. 22 Does religious coping or use of religious resources help victims of abuse? Webb and Whitmer 21 found that self-worth was inversely related to the use of self-reliance, but positively associated with collaboration with God. In addition, Ryan 23 found that seeking personal spirituality helped in the recovery from childhood sexual abuse.
The purpose of this study was to assess the relative impact of spiritual symptoms and religious coping on attitudinal/behavioral and clinical outcomes among women in violent relationships while controlling for demographics, and violence characteristics and dynamics.
Methods
Sample
The methods used have been reported previously; 24 this study was approved by the Institutional Review Board at the University of Texas Health Science Center at San Antonio. In this study, women with a recent history of husband-to-wife abuse were recruited from six primary care clinics in San Antonio, TX. Adult (18–64 years old), nonpregnant women seen without their husbands present at the time of the visit were asked to complete a six-item brief Conflict Tactics Scale 25 in the examination room while they waited to see their physician. If they had experienced violence from their partner in the past 30 days, they next responded to a Danger Assessment Screen. Women in severely dangerous relationships were excluded from the study. All women with a positive screen for partner violence, whether they participated in the study or not, were referred to the Family Justice Center, a city-supported victim assistance program located in one of our downtown clinical buildings.
Procedure
Once enrolled, the 200 subjects completed a baseline interview eliciting data on demographics, relationship and violence history, and mental disorders as well as both attitudinal/behavioral and clinical outcomes. Subjects were instructed to complete a daily assessment of husband and wife violence for 12 weeks using the Interactive Verbal Response via telephone. At the completion of the study, researchers contacted each participant to determine whether she had sought professional help concerning the violence or left the relationship.
Measurement
The baseline assessment included basic information about the relationship (duration of the relationship, duration of the marriage, duration of abuse) and three religious/spiritual variables. (1) The number of visits to a religious/spiritual counselor (i.e. clergy, folk-healer, or spiritualist) during the prior two months was assessed using the Health Care Utilization form. 26 (2) Religious coping was measured using the COPE instrument. 27 (3) The severity of spiritual symptoms (i.e., lack of reason for living, lack of sense of purpose, lack of harmony and peace, lack of feelings of productivity, and lack of self-comfort) was assessed using the Biopsychosociospiritual Inventory (BioPSSI) with higher scores indicating more spiritual problems. 28
Previous work showed that IPV could impact subjects’ health, attitudes, and/or behaviors. Hence, we assessed both attitudes and behaviors (hope, coping strategies, appraisal, and support) as well as clinical outcomes (health care utilization, functional status, symptom levels, and readiness for change) at the beginning and end of the study period. Hope was assessed using the 12-item Herth Hope Scale. 29 Coping strategies were assessed with the 53-item COPE, which has 12 subscales measuring active versus avoidant coping mechanisms. Five scales measure problem-focused coping, four scales measure emotion-focused coping, and three scales measure maladaptive coping. Because the COPE can assess situational and dispositional coping, it could be sensitive to change. 27 Appraisal was assessed using the Appraisal Dimension Scales. This 24-item instrument assesses six dimensions of appraisal (control, salience, novelty, duration, causality, and predictability). Appraisals were directed at the primary stressor (violence). 30 Finally, family support and stress were assessed using the 22-item Duke Social Support & Stress Scale. 31
Clinical outcomes included the following: Health care utilization was assessed using a 10-item health care utilization instrument which documents the number of visits to general medical (emergency departments, minor emergency rooms, clinics, and medical physician offices) and mental health (psychiatrists, psychologists, social workers, and therapists) settings in the previous two months; 26 previous studies suggest that depressed patients accurately recall two-month utilization. 32 Functional status was measured using the Medical Outcomes Study Short Form-36 (MOS SF-36). The SF-36 consists of 36 items forming eight subscales and was used to assess functional status and quality of life. 33 Symptomatology was evaluated using the BioPSSI. This 29-item instrument assesses physical, psychological, social, and spiritual symptoms. 28 Finally, readiness for change was assessed using questions based on the Transtheoretical Model of Change. This model states that behavior change moves through five stages: precontemplation, contemplation, preparation, action, and maintenance. 34 Subjects were asked to report their plans to (1) seek help for their domestic violence and (2) leave the relationship using a 5-point scale from I am not interested to I am trying to leave (get help) now. 35
Analysis
Three measures of violence severity were computed. First, the frequency of husband-perpetrated violence was used. Second, the mean level of episode severity for husbands was calculated across all days in which any violence occurred. Finally, the overall level of violence burden for husbands was calculated as the mean daily violence across all days reported.
Assessment of violence dynamics
To quantitatively assess violence dynamics, time series data must be complete. Daily reports were made on a mean of 63.2 (±15.9 SD) days with 50% of subjects reporting on 80% of days or more; missing data were imputed using the n-step procedure in the TISEAN software package 36 to maintain any nonlinear characteristics. The n-step approach to imputation has been shown to least distort nonlinear characteristics of time series when compared to traditional methods. 37 Unlike other approaches to handling missing data, n-step successfully corrected for 25–60% missing data if such data were missing at random and 15–40% if missing data followed a power distribution in chaotic time series, and 40% and 25%, respectively, in periodic time series. 38 When the initial data points in the time series were insufficient to apply n-step (generally n ≤ 4), the mode of the time series was inserted until the time series was long enough to use n-step.
Three types of complexity measurements are available, and we used one example of each type. 39 Nonlinearity suggests either chaotic or random dynamics. Algorithmic complexity (a measure of the amount of information needed to describe the data) was measured by LZ complexity. 40 Regularity (or the lack of it) was measured by approximate entropy (ApEn). 41 Finally, sensitivity to initial conditions (speed with which two adjacent points diverge over time) was measured with the largest Lyapunov’s exponent. 42 Using the time series of the daily assessments of level of husband-to-wife violence, we calculated LZ complexity and Lyapunov exponents using the Chaos Data Analyzer software for each subject’s time series. We calculated ApEn using the ApEn module in OCTAVE. Stable estimates require as few as 50 data points for ApEn43–45 and 30 data points for LZ complexity; 46 Lyapunov exponents are resistant to the effects of missing data if nonlinearly imputed data (≤15%) were used in datasets with underlying periodic or chaotic dynamics. 38
Relationship between violence, religion/spirituality, and outcomes
Outcome factors.
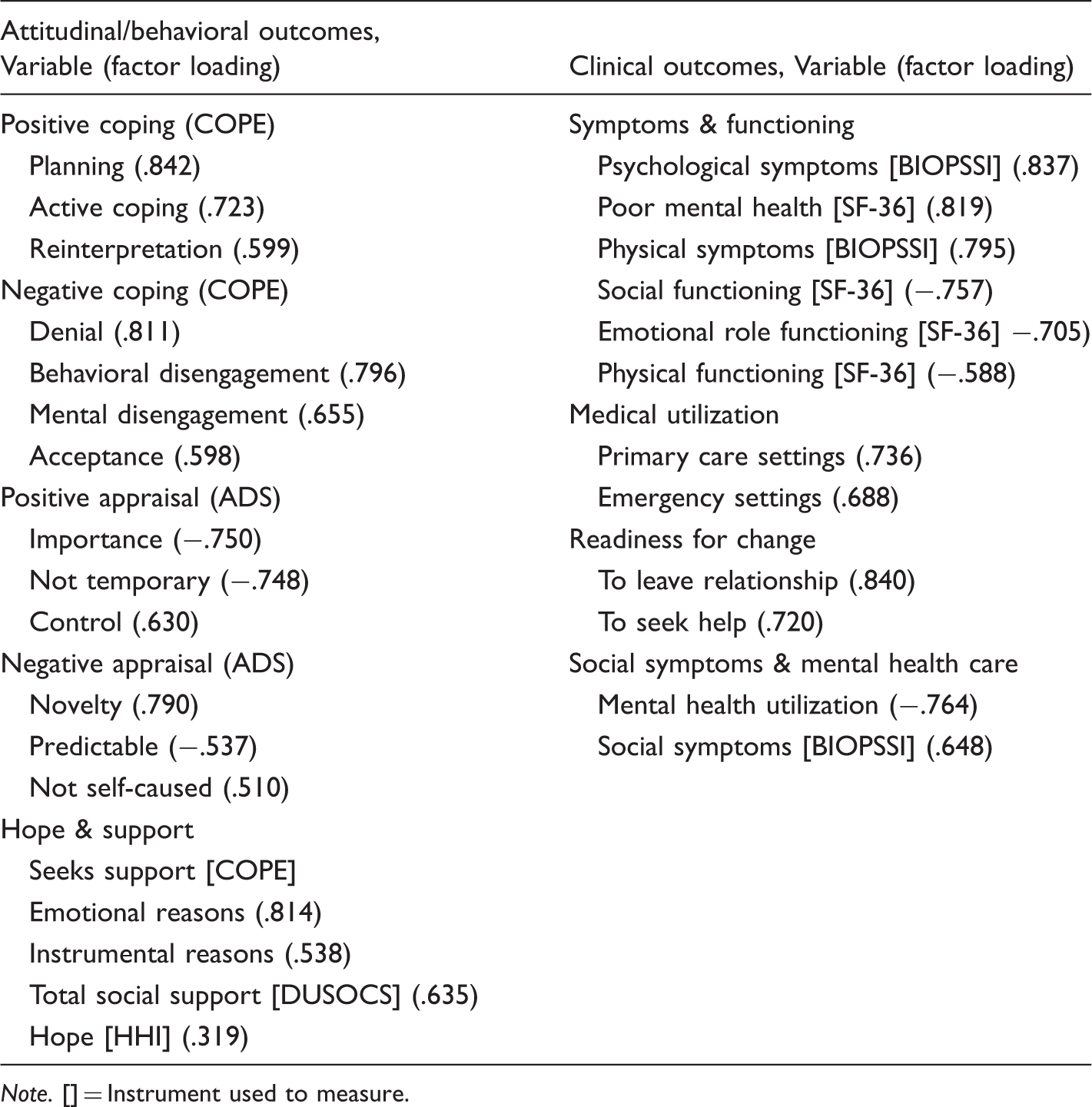
Note. [] = Instrument used to measure.
Results
Demographic information (n = 200).
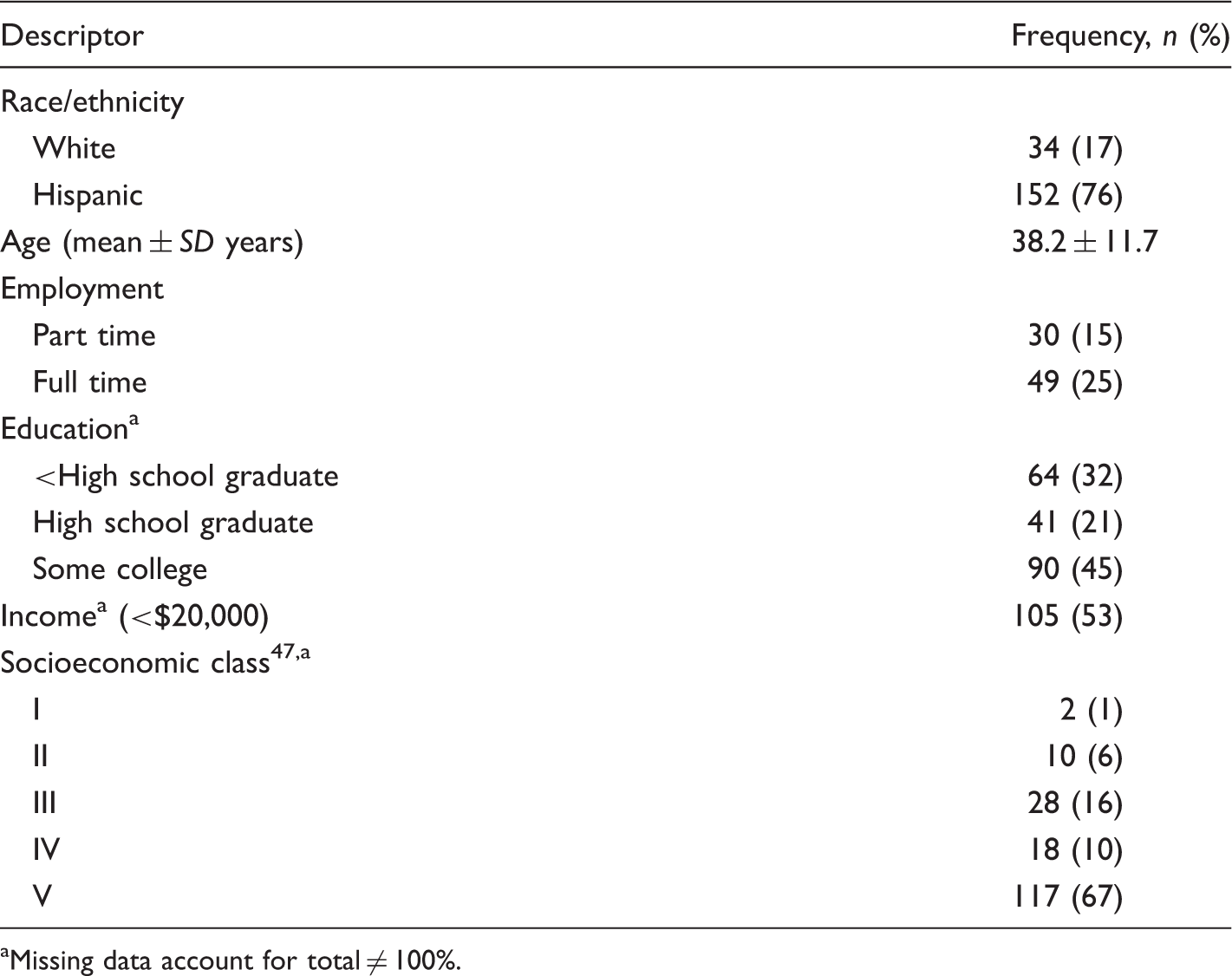
Missing data account for total ≠ 100%.
Predicting attitudinal/behavioral outcomes [beta (p)].
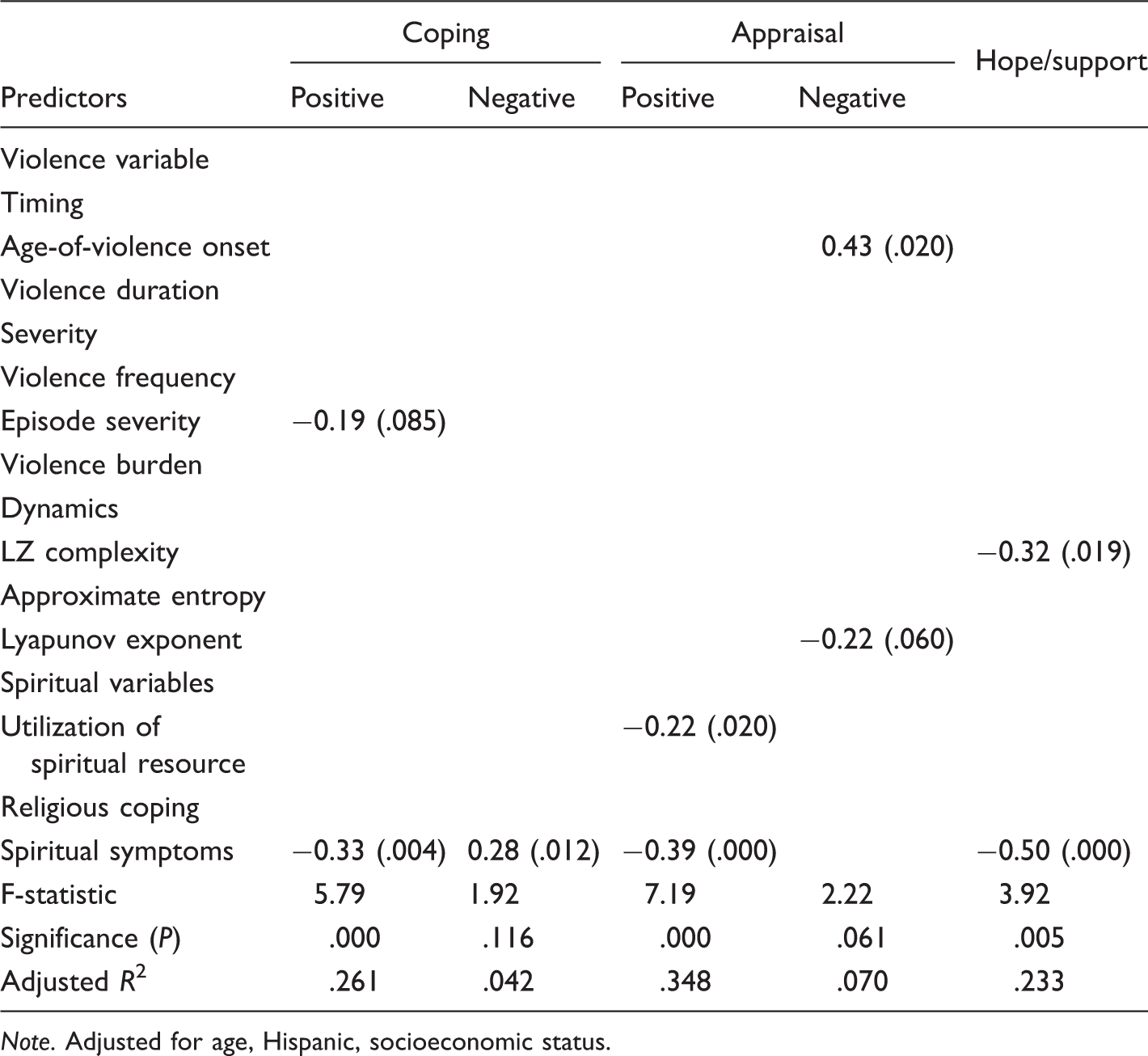
Note. Adjusted for age, Hispanic, socioeconomic status.
Predicting clinical outcomes [beta (p)].
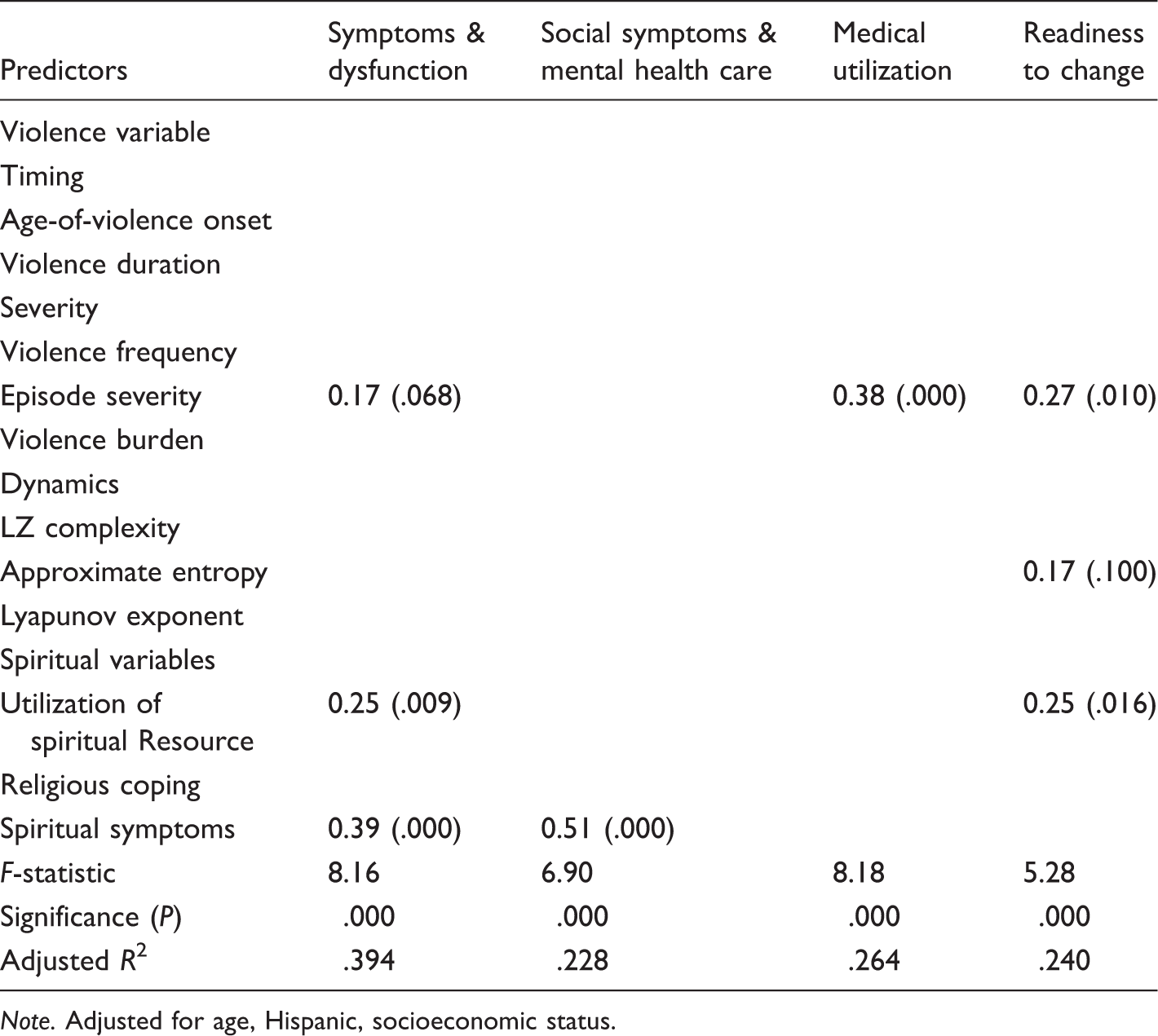
Note. Adjusted for age, Hispanic, socioeconomic status.
Predicting action taken [beta (p)].
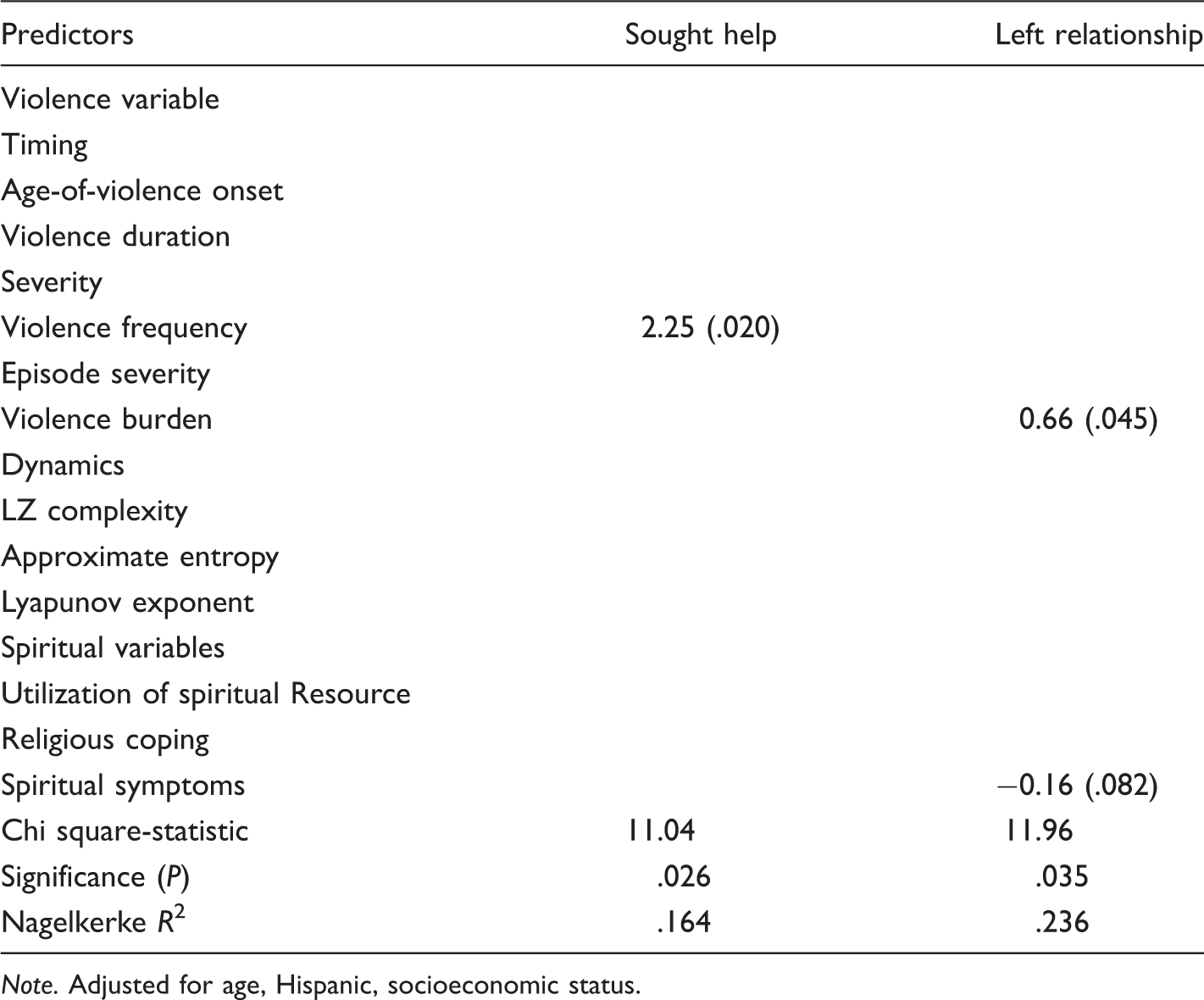
Note. Adjusted for age, Hispanic, socioeconomic status.
Discussion
After controlling for duration, severity and dynamics of the violence, the use of spiritual resources, and the level of spiritual symptoms were associated with most of the attitudinal/behavioral and clinical outcomes, while low religious coping was only associated with leaving the relationship. Unlike our prior study, 48 a history of a church wedding was unrelated to leaving in the current study.
The level of spiritual symptoms and concerns had a significant effect on all of the attitudinal/behavioral outcomes except negative coping, even when controlling for violence severity and relationship characteristics. As spiritual symptoms worsened, positive coping, appraisal, and hope/support decreased, and symptoms/dysfunction and social symptoms worsened. Few studies have looked at spiritual symptoms. Katerndahl 49 reported an impact of spiritual symptoms on increased utilization of general and mental health settings as well as poorer quality-of-life measures in a general primary care population. In a prior analysis of these data, 50 women in violent relationships decreased rather than increased their mental health care utilization in response to spiritual symptoms, possibly due to the inverse relationship between hope and mental health utilization previously observed in IPV. However, women in that analysis also noted similar associations between spiritual symptoms and dysfunction as those in the current analysis.
Previous research suggests potential contradictory effects of spiritual resource use. Religious communities can provide support, improve quality of life, and assist healing,2,51 and church attendance and religious involvement are linked to increased self-efficacy, 52 improved social support, and decreased psychiatric symptoms. 53 However, religious resources can have negative effects as well, perpetuating silence about the abuse 54 and alienating victims. 55 In fact, involvement of church leaders and clergy can also be problematic. While clergy can promote self-esteem 52 and safety, 56 use of these social resources can also serve to maintain the violence56–59 and inhibit healing. 60 This may explain why women are often dissatisfied with the faith-based IPV resources they use. 61 However, in this study, associations with the use of spiritual resources were not contradictory; such use was inversely related to positive appraisal, but positively to both symptoms/dysfunction and readiness to change. Thus, women in violent relationships seek spiritual resources when experiencing high levels of symptomatology and dysfunction, lacking positive appraisals, and considering taking action.
Actually taking action (leaving the relationship) was uniquely and inversely related to religious coping. Religion, in general, is used as a coping strategy in IPV and can be transformative, empowering them to change.62,63 Prior studies in primary care populations suggest that religious coping is associated with social support and health status 2 and, among victims of violence, religious coping can diminish psychiatric symptoms64–66 and promote well being.64,67 However, it can also serve as a barrier to safety.68,69 In this study, religious coping was inversely related to leaving the relationship only, possibly confirming its role as a motivation to stay in the relationship.
This study has several implications. First, independent of the duration, severity and dynamics of the violence, religious and spiritual factors are important to our understanding of outcomes; we need to attend to them when we are dealing with victims of IPV. Second, the level of spiritual symptoms (i.e. lack of purpose or peace) is consistently and inversely related to positive outcomes. Perhaps interventions targeting these symptoms need to be developed for victims of violence.
This study also has limitations. First, the associations found in this study are only associations and cannot be used to determine causality. In addition, the population in this study was predominantly low income and Hispanic; previous studies found that the effect of religious involvement on IPV varied with ethnicity. 70 African Americans, for example, use religious coping more than other groups after sexual assault64 and partner violence, 71 and prefer spiritual sources over medical ones for IPV. 72 In these samples, church attendance led to reduced IPV frequency. 70 Thus, the results of this study may not apply to other populations.
In conclusion, even after adjusting for violence severity, duration and dynamics, religious and spiritual factors were associated with most outcomes. Spiritual symptoms had a consistently negative effect on outcomes while use of spiritual resources had variable effects. Religious coping was only associated with remaining in the relationship.
Footnotes
Acknowledgments
We wish to thank Stephanie Mitchell, Kelli Giacomini, Robert Mesec, and Wilson Pace for their invaluable assistance.
Conflict of interest
None declared.
Funding
This study was funded through a grant from the National Science Foundation (#0826812). Automated data collection was provided by the University of Colorado, Department of Family Medicine Information Services group.