
Abstract
Priapism is a rare but severe medical condition of sustained and painful erection of penis in the absence of any sexual stimulation, in which the penis does not return to a flaccid state. It is considered to be a medical emergency because without treatment it can lead to permanent damage and fibrosis of penis and in the long run to impotency. Albeit that there is no uniform consensus regarding the duration of sustained erection, an erection lasting more than 4 h is generally considered as an emergency which needs immediate medical attention and care. Priapism is commonly associated with iatrogenic, pharmacologic, underlying medical, or traumatic causes. In this report, we present the case of a 42-year-old African American man who developed priapism after three weeks of therapy with paroxetine which lasted for more than 96 h before coming to the attention of his health-care providers. This case is unique in that there are no reports in literature of an erection lasting for such a long duration following therapy with paroxetine. The objective of this report is to highlight the importance of recognizing the possibility of priapism with selective serotonin reuptake inhibitors in general and paroxetine in particular since this condition is not commonly seen in clinical practice to be associated with selective serotonin reuptake inhibitors and may go unrecognized. Also, potential biological mechanisms involved in the development of paroxetine-induced priapism are presented.
Introduction
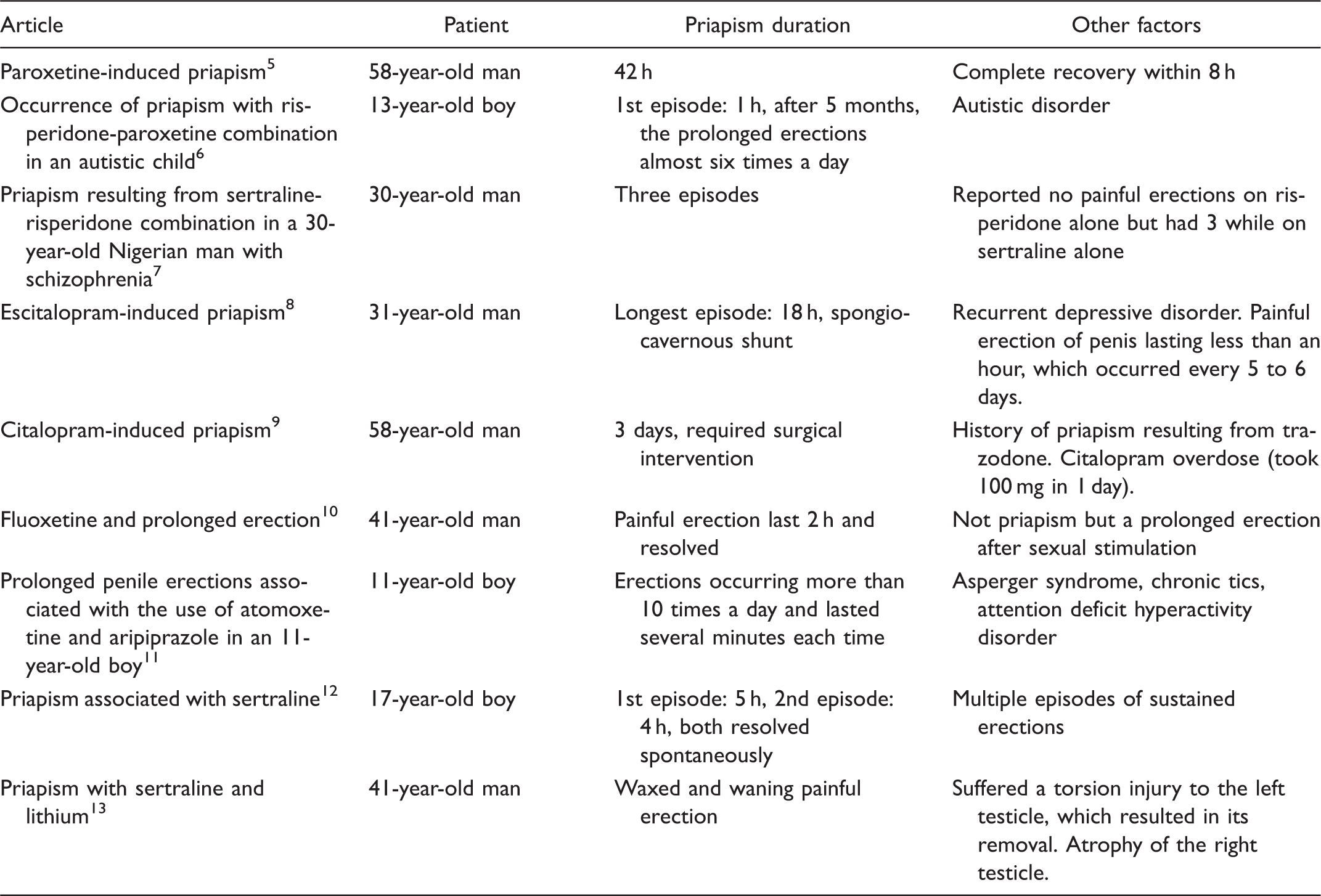
Literature review representing patient age, duration of priapism, and other factors associated in priapism.
Case presentation
Mr. R, a 42-year-old African American man was committed to a state psychiatric hospital by his mother for peeping into people’s windows, exposing himself and masturbating in public, and walking the streets at night. Mr. R had a long history of engaging in high-risk and inappropriate behaviors that were sexual in nature. A remark made by him at the time of his initial evaluation, “the devil enters my mind and makes me do stuff” exemplifies how he rationalized his behaviors and expressed his lack of control and helplessness over them. He did not have any history of psychotic symptoms including auditory or visual hallucinations or any paranoia and his thoughts and actions, outside of his behaviors, were based in reality. He admitted to being stressed due to his “bad habit,” but screening for symptoms of anxiety, depression, or mania did not reveal any other psychopathology. He wanted to quit engaging in his sexual fantasies publically but was too embarrassed to talk about it. He did not report any problems at work. He also denied any suicidal or homicidal ideations or plans. He endorsed drinking about a 12-pack beer per day but had not consumed any alcohol in the three weeks leading up to his hospitalization. He denied any other illicit drug use. He had a documented history of voyeurism since age 13. He also had a history of engaging in other sexually inappropriate behaviors like masturbating in public. In addition to alcohol dependence, he also had nicotine dependence (50–75 pack-years) and untreated hypertension.
In terms of his social history, he was raised by his mother along with two half-siblings. He had an 11th grade education and had dropped out of school in order to find work. He had no history of any physical, emotional, or sexual abuse as a child. His occupational pursuits included working as a landscaper and painter. He was single and had never been married. He lived with his mother and made about $200 per week. He had been arrested for trespassing and stalking in the past and was on probation.
Mental status examination revealed a 42-year-old well-built, well-nourished African-American man who appeared his stated age and did not demonstrate any impairments in his thought process, thought content, perception, and cognition although he had poor insight and judgment given his intentional indulgence in high-risk behaviors despite knowing the consequences.
Physical examination was unremarkable other than untreated hypertension and a body mass index of 32.6 indicative of obesity. His blood pressure ranged between 128–151 mm Hg (systolic) and 78–98 mm Hg (diastolic), and pulse between 66 and 94 beats per minute. His laboratory work was unremarkable except for high-normal potassium of 4.6 mEq/L and a slightly elevated red blood cell count of 5.97 million per microliter of blood. Although his urine drug screen was negative, blood alcohol concentration was not available which would have helped determine need for detoxification, given his heavy alcohol use. He however did not present with any withdrawal symptoms which were monitored as a part of routine admission protocol using Clinical Institute Withdrawal Assessment for alcohol. 18 Patient had a positive skin tuberculin test, but chest x-ray revealed no active tuberculosis (TB) and did not patient exhibited any clinical symptoms of TB. Given his high body mass index, a history of untreated hypertension and heavy drinking and smoking, he was considered at high risk for cardiovascular comorbidity.
Patient had an uneventful hospitalization over the course of 10 days, with no issues besides constipation for the first 3 days of hospitalization, which resolved on day 4 after 2 days of being given milk of magnesia. On day 12 of hospitalization, the patient informed his attending psychiatrist that he had an erection, and that it had been present for 4 days. The patient was assessed by the internist who determined that patient had a rigid, erect penis on physical examination. Patient was transferred to ED immediately after it was determined that he was suffering from priapism. Patient had been prescribed paroxetine, which he received since the first day of hospitalization and had been started on it in the community by his psychiatrist about three weeks prior to his hospitalization. Paroxetine was immediately discontinued on day 12 once it was thought to be a potential causative factor for his priapism. Other medications that were prescribed included trazodone which was prescribed on an as-needed (prn) basis for insomnia, although review of medication administration record (MAR) revealed that he had not received any doses of trazodone and isoniazid which was prescribed for TB prophylaxis. Trazodone as a prn medication was also discontinued.
In the ED, patient was found to have a rigid, erect penis with no plaques palpable along the shaft. He was alert and oriented. His corpora cavernosa was irrigated, but this did not cause the erection to subside. Urology was consulted who gave the patient four intracavernosal injections of 200 µg of phenylephrine and this made the erection subside transiently, but it recurred the next morning. The patient was then taken to the operation room on day 2 of medical hospitalization where he was found to have ischemic priapism. He underwent a bilateral corporotomy and irrigation with subsequent clot evacuation. A distal penile shunt was placed, after which the erection subsided and the patient maintained normal urinary function. He was discharged on postoperative day 4 following complete resolution of priapism without any recurrence. At outpatient follow-up 10 days later, patient continued to maintain detumescence without any intercurrent periods of sustained erections.
Discussion
Paroxetine is a drug that generally belongs to the class of SSRIs. At common therapeutic dosages, it mainly blocks the presynaptic reuptake of serotonin, thus increasing the levels of this neurotransmitter in the synaptic cleft. 19 It is used most commonly to treat major depression and certain anxiety disorders. Sexual side effects of SSRIs are known to be a source of noncompliance or discontinuation among patients. The knowledge that SSRIs might induce priapism is less documented. However, other antidepressants, such as trazodone or phenelzine, have been repeatedly associated with their potential to induce priapism.16,17
Although not extensively known, compared with SSRIs, antipsychotics such as risperidone have been more comprehensively reported to induce priapism. For example, in a PubMed search with the criteria “SSRI-induced priapism,” the second search result generated was “Olanzapine-associated priapism.” 20 Furthermore, a search for “Paroxetine-induced priapism” yielded three articles with two of the three articles including an antipsychotic plus paroxetine. 5 Overall, there are very few cases of priapism with paroxetine reported in the literature. In addition to the increased documented accounts of antipsychotic drugs inducing priapism, there is a clearer presumed mechanism for how these medications cause priapism as opposed to SSRIs like paroxetine. They are theorized to cause priapism by alpha-1 adrenergic blockade in the corpora cavernosa of the penis. This blockade leads to arteriodilation causing increased blood flow into the corpora cavernosa and additionally inhibits the sympathetic system in its role of inducing detumescence. The mechanism in which SSRIs induce priapism is hypothesized to involve action on 5-HT3 receptors, which may be involved in the generation of erections. Interestingly, the effect of paroxetine on nitric oxide synthase activity was studied in which it was concluded that paroxetine is a nitric oxide synthase inhibitor. 21 Thus, paroxetine may have role in preventing formation of nitric oxide, which is involved in the erectile process; yet, curiously, paroxetine is linked to the opposite effect of inducing priapism in users.
Priapism is considered a urologic emergency and should be promptly treated within 4 to 6 h of presentation. Failure to promptly treat the sustained erection can lead to gangrene, fibrosis and permanent penile dysfunction, and even penile amputation in the worst case scenario. 17 Our patient was prescribed paroxetine prior to his admission to a state hospital for voyeurism and public masturbation in order to reduce hypersexuality. The patient was prescribed trazodone as needed for insomnia; however, when his institutionalized MAR was reviewed, it confirmed that the patient was never given a dosage of the medication. No blood or urine sample analysis of active or excreted metabolites of trazodone was done, however, which may have helped determine conclusively whether trazodone was given. This may be one of the limitations of this report. According to the Naranjo scale, 22 the likelihood of an adverse drug reaction (ADR) was calculated to be 7, which equates to a probable ADR. This scale calculates the probability of ADR which can be definite, probable, possible, and doubtful depending on cut off scores. A score in the range of 5–8 is considered probable.
The duration of the patient’s priapism was more than 96 h. In examining the literature, most reported cases of patients with SSRI-induced priapism had durations between 2 and 42 h or episodes of priapism as opposed to continuous duration (Table 1). Additionally, in several of these cases, prolonged erections resolved spontaneously without intervention (Table 1). In comparison, our patient required a bilateral corporotomy and irrigation with subsequent clot evacuation. Additionally, our patient’s course of paroxetine was four weeks before the onset of sustained erection. Examination of literature revealed that in a couple of case reports, priapism occurred when patients were on a combination of medications, an adolescent who was on risperidone and paroxetine, 6 and a Nigerian man who experienced priapism while on sertraline and risperidone. 7 Our patient was not on a combination therapy that included an antipsychotic and was solely taking a SSRI which also makes our case unique from others.
There are various medical conditions that predispose an individual to priapism. Furthermore, Du Toit et al. 23 conclude that priapism can be related to hematologic and vascular abnormalities, spinal cord injury, neoplasms, and prostatitis. There are two subtypes of priapism, which includes ischemic and high flow. 23 The causes of low-flow priapism include injecting vasoactive drugs into the cavernosa, sildenafil, sickle cell disease, perineum or penile trauma, and solid tumors in the bladder or prostate. 24 Additionally, individuals with sickle cell disease have a high prevalence rate of priapism of around 42%. 25 The main cause of high-flow priapism is due to trauma to the penile, perineal, or pelvic region. 21 Our patient had no predisposing conditions that could have caused his priapism; thus, the only predisposing factor was the paroxetine he was prescribed. Another limitation of the case stems from the patient’s past history of voyeurism and long history of engaging in masturbation. It is not definitively known if the patient was engaging in excessive sexual stimulation while he was hospitalized which could have contributed to his prolonged erection. Other conditions that can be considered in the evaluation of priapism in our patient are alcohol dependence and drug abuse. The last drink he had was about three weeks prior to being hospitalized and he did not present with any withdrawal signs and symptoms. His urine drug screen was negative. Hence, alcohol and psychoactive drug use do not seem to be involved. Lastly, priapism as a manifestation of serotonin syndrome could not have been a possibility as serotonin syndrome is a clinical diagnosis, 26 and our patient had no clinical features of serotonin syndrome and his blood chemistry did not reflect any abnormalities, like increases in white blood cell count or creatine phophokinase, which may have pointed toward it.
In summary, the patient is a 42-year-old African American man with no significant medical history or predisposing conditions associated with priapism. The patient was prescribed paroxetine for hypersexuality who subsequently developed priapism. Paroxetine was the only known factor that could have led to his presentation of sustained erection. In view of the Naranjo scale score of 7, MAR review which indicated that no other medication could have possibly contributed to patient’s priapism, a cause-and-effect relationship between paroxetine intake and priapism onset and lack other causes which could have caused priapism, it was concluded that paroxetine was the probable cause of the patient’s priapism.
Conclusion
Although rare, it is important to inform about SSRIs’ potential to induce priapism. It should be recommended that physicians inform their patients about the possibility of priapism under SSRIs such as paroxetine. Untreated priapism can result in permanent dysfunction of the penis. Thus, patients should be aware of this complication, so if it were to occur, they will know to seek prompt medical attention for adequate care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.