
Abstract
Objective
Computed tomography coronary angiography, a key method for obtaining coronary artery images, is widely used to screen for coronary artery diseases due to its noninvasive nature. In China, 64-slice computed tomography systems are now the most common models. As factors that directly affect computed tomography performance, heart rate and rhythm control are regulated by the autonomic nervous system and are highly related to the emotional state of the patient. The aim of this prospective study is to use a pre-computed tomography scan Self-Rating Anxiety Scale assessment to analyze the effects of tension and anxiety on computed tomography coronary angiography success.
Methods
Subjects aged 18–85 years who were planned to undergo computed tomography coronary angiography were enrolled; 1 to 2 h before the computed tomography scan, basic patient data (gender, age, heart rate at rest, and family history) and Self-Rating Anxiety Scale score were obtained. The same group of imaging department doctors, technicians, and nurses performed computed tomography coronary angiography for all the enrolled subjects and observed whether those subjects could finish the computed tomography coronary angiography scan and provide clear, diagnostically valuable images. Participants were divided into successful (obtained diagnostically useful coronary images) and unsuccessful groups. Basic data and Self-Rating Anxiety Scale scores were compared between the groups.
Results
The Self-Rating Anxiety Scale standard score of the successful group was lower than that of the unsuccessful group (P = 0.001). As the Self-Rating Anxiety Scale standard score rose, the success rate of computed tomography coronary angiography decreased.
Conclusions
The Self-Rating Anxiety Scale score has a negative relationship with computed tomography coronary angiography success.
Advances in knowledge
Anxiety can be a disadvantage in computed tomography coronary angiography examination. The pre-computed tomography coronary angiography scan Self-Rating Anxiety Scale score may be a useful tool for assessing whether a computed tomography coronary angiography scan will be successful or not.
Introduction
Coronary heart disease, which is a narrowing or blockage of the arteries and vessels that provide oxygen and nutrients to the heart, is caused by atherosclerosis, an accumulation of fatty material on the inner linings of arteries. Coronary heart disease is best diagnosed by “seeing” the arteries. Numerous techniques are available for visualizing arteries, including coronary angiography, 1 computed tomography (CT) coronary angiography (CTCA), 2 and magnetic resonance angiography. 3
CTCA is the easiest of these imaging methods to perform, and its success rate can be increased by using a CT machine with a sufficiently fast scan rate. CTCA might fail in many patients because of poor heart rate (HR) control, HR variability, coronary calcification, motion artifacts, or insufficient vessel opacification.4,5 However, the effect of anxiety in this context has not been previously studied.
Regardless of the scan speed of CTCA, good HR control can improve both the success rate and image quality of CTCA. 6 Stricter HR control is required for 64-slice CTCA than for newer and more advanced CT systems. Better HR control may be highly related to the emotional state of the examinee. In practice, anxiety is the most common situation that affects CTCA success. Therefore, the aim of this study was to establish the relationship between the CTCA success rate and anxiety.
Materials and methods
Study participants
A total of 378 patients (219 men, 57.94%) who were undergoing CCTA at our hospital from June 2011 to March 2013 were enrolled in this study. The mean age of study participants was 57.56 years (range, 30–86 years). Written informed consent was provided by every patient.
Inclusion criteria of the study were as follows: patients who (1) had a suspected diagnosis of coronary heart disease, (2) underwent coronary assessment after percutaneous intervention or coronary bypass surgery, and (3) agreed to participate in the study and signed an informed consent form. Exclusion criteria were as follows: patients who (1) had an iodine allergy, (2) severe hepatic or renal dysfunction, (3) thyroid dysfunction, (4) persistent atrial fibrillation, or (5) refused to participate.
HR control
All patients underwent electrocardiography (ECG) before the CT examination to exclude severe arrhythmias and to calculate the baseline HR and HR variability (HRV). When the HR was 65 bpm or less and the HRV was 3 bpm or less, CTCA was performed. Some patients, depending on the baseline HR and HRV, were administered metoprolol (≤200 mg) if their HR was >65 bpm to reach the target HR. Patients who had a higher HR or HRV were excluded. Blood pressure was monitored when metoprolol was administered to keep the blood pressure above 90/60 mm Hg. 7
Self-Rating Anxiety Scale
The Self-Rating Anxiety Scale (SAS) was designed by William WK Zung in 1971 to quantify a patient’s level of anxiety. The SAS scale is a 20-item self-reported assessment device. When answering each item, the person indicates the degree to which each statement applies. Each question is scored on a Likert-type scale of 1 to 4 (based on the following replies: “a little of the time,” “some of the time,” “a good part of the time,” and “most of the time”). The total score is obtained by summing the assessment of the 20 items. The total score multiplied by 1.25 gives the standard score. A standard cutoff score of 50 is usually used to diagnose anxiety. 8 In China, in accordance with the China Mental Health Center, the standard score ranges are 25–49 (normal range), 50–59 (mild anxiety), 60–69 (moderate anxiety), and ≥70 (severe anxiety).
CTCA imaging
CTCA was performed with a 64-MSCT scanner (Light Speed VCT; GE Healthcare, Milwaukee, WI, USA). A positive lateral scan was first performed to locate the heart and scanning area. For the coronary artery calcium score (CACS) scan, the following parameters were used: 120 kV tube voltage, 260–480 mA tube current, prospective ECG-gating axial scan, 75% R-R interval, 2.5 mm slice thickness, 2.5 mm slice increment, 25 cm × 25 cm visual field, 512 × 512 matrix, and a standard reconstruction algorithm.
By using the CACS images as a guide, the beginning of the left coronary artery was set as the first scanning plane. Contrast (20 ml) was injected through the ulnar vein with a high-pressure syringe at a speed of 5 ml/s. Single-level test bolus injection dynamic scanning was then performed with the following parameters: 120 kV tube voltage, 100 mA tube current, 5 mm slice thickness, 0.5 s scanning speed, and 1.5 s interscan delay. Two regions of interest were chosen at the base of the aorta and pulmonary conus, and a time–density curve was plotted to confirm the aortic and pulmonary artery peak times.
For the CTCA scanning, the following settings were used: 110–140 kV tube voltage, 210–770 mA tube current, retrospective ECG-gating scan, 0.625 mm slice thickness, 25 cm × 25 cm visual field, and a standard reconstruction algorithm. The scanning delay time was the aortic peak time plus 4 s. If the predicted HR was less than 65 bpm, single-sector scanning was used. If the HRV was less than 3 bpm and no motion artifacts were seen in the right coronary artery on CACS scanning, 75% R-R interim scanning or 35%–80% R-R interim scanning was used. If the HR was greater than 65 bpm, dual-sector scanning and 35%–80% R-R interim scanning were used.
All patients reached the target HR before the CT scan. Some patients showed HR and rhythm instability when at rest in the CT machine before scan commencement. If the heart beats were still unstable 10 min later, the scan was not initiated. In some patients, HR and rhythm instability occurred after the scan started, which caused an image rebuilding failure. If the final image quality was adequate for making a diagnosis, then the scan was defined as a success; otherwise, the scan was considered a failure.
Statistical analysis
All analyses were performed with SPSS for Windows (version 16.0; SPSS, Chicago, IL, USA) statistical software. Continuous data were presented as the mean ± standard deviation or, when appropriate, as the median and range. Comparisons between groups were analyzed for significance with a Student’s t test and chi-square test. Correlation was calculated with Pearson’s correlation coefficient. All tests were two sided. Significance was assumed at P < 0.05.
Results
Clinical observation and basic data
Basic information of enrolled patients.
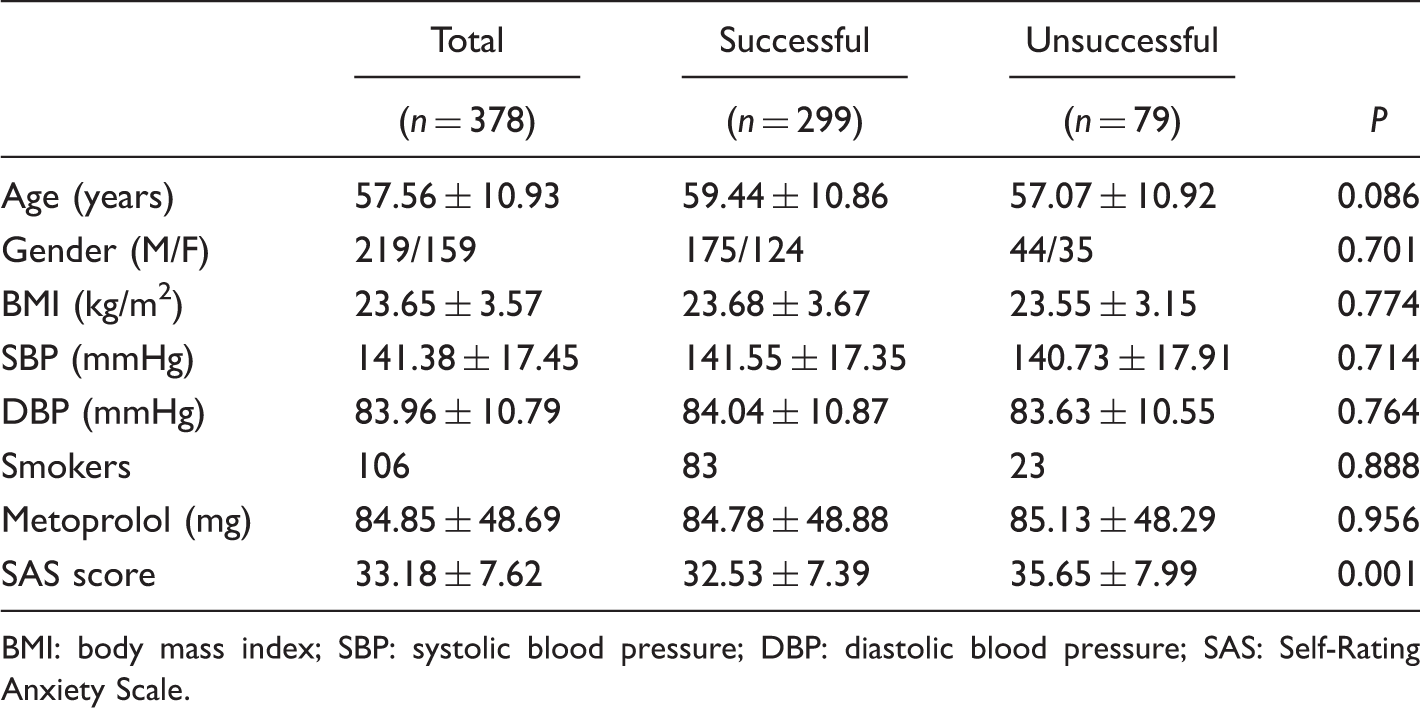
BMI: body mass index; SBP: systolic blood pressure; DBP: diastolic blood pressure; SAS: Self-Rating Anxiety Scale.
Before the CT scan, each patient was asked to complete a SAS questionnaire. A physician ensured that the patient’s HR was less than 65 bpm. The HRs of all 378 patients reached the target beats per minute. Of the 378 patients, 299 (79.10%) successfully completed the CCTA scan and clear diagnostic images were obtained. A total of 79 patients (20.90%) were not successfully imaged due to an increase in HR during the CT scan or poor-quality images.
There were no differences between the successful and unsuccessful groups for all factors recorded except the SAS score. The average standard SAS score for all enrolled patients was 33.18 ± 7.62. A total of 299 patients of the successful group had a lower SAS standard score (32.53 ± 7.39) than 79 patients of the unsuccessful group (35.65 ± 7.99, P = 0.001).
SAS standard score and CTCA scanning success rate
SAS standard score and CTCA success rate in different groups categorized by quartile of SAS score.
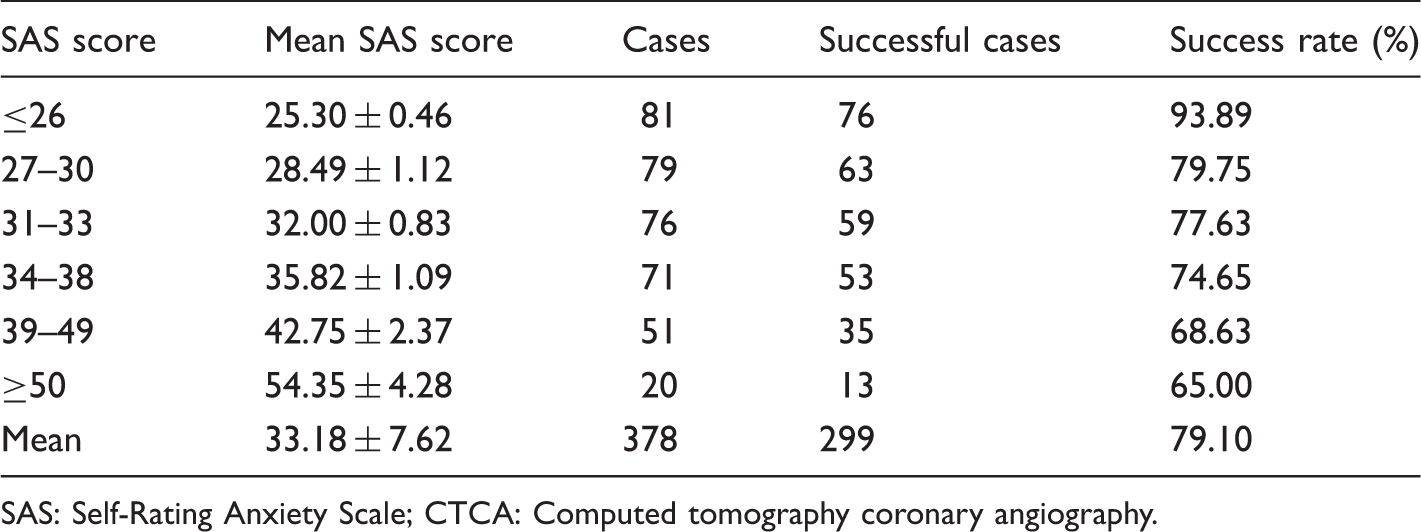
SAS: Self-Rating Anxiety Scale; CTCA: Computed tomography coronary angiography.
Discussion
Due to the sensitivity of CTCA to patient motion, in our hospital, we always try to lower patient HR to 55–65 bpm before beginning CT scanning. For some patients, although their HRs are well-controlled just before the CT examination, the scan ultimately fails due to premature beats or a sudden rise in the HR. Such conditions are usually caused by stress or anxiety. Thus, to determine the relationship between the CTCA success rate and anxiety, in the current study, we used the SAS scale to evaluate the anxiety of the patients before the CT scan.
The SAS standard scores of the 79 participants who failed the CTCA examination were higher than those of the 299 patients who successfully completed the CTCA scan and obtained diagnostically useful coronary images (P = 0.001). The SAS standard score was lower than 50 in most patients; only 20 patients showed a score higher than 50. According to the diagnosis cutoff value in China, these values indicate that most study participants would not be diagnosed with anxiety. However, the SAS score may still be used as a tool to evaluate the degree of anxiety.
Since the first clear coronary transverse slices obtained with CCTA were used to acquire coronary images in the 1990s, the technology has developed rapidly. It is now widely used worldwide in the screening and diagnosis of patients at high risk of coronary artery disease. As CT technology continues to develop, the scanning speed is increasing, with 128-, 256-, 320-slice, and even faster CT machines are now available.9–11 For CCTA, the most important factors are HR and rhythm control. The faster the CT scanning speed is, the less the HR and rhythm must be carefully controlled. Owing to scanning speed advances, CCTA can even be successfully performed in atrial fibrillation patients. 12 However, because 64-slice CT machines are the most common type in Chinese hospitals, 13 HR and rhythm control are still very important in China.
Anxiety is an emotional reaction triggered by uncertainty about something. When a patient agrees to undergo CTCA for the first time, he or she might feel a sense of unease or anxiety, leading to the concomitant activation of the autonomic nervous and endocrine systems, with complex and diverse consequences. Symptoms induced by anxiety may be highly related to the sympathetic nerve system. Noradrenaline, excreted by postganglionic fibers of the sympathetic nervous system, has positive chronotropic, dromotropic, and inotropic actions that make the heart beat stronger and faster, increasing both HR and blood pressure. 14 In addition to the cardiac system, other systems, such as the gastrointestinal and respiratory systems, may show related responses.
CT scans can be a source of stress, particularly for those who are undergoing the procedure for the first time. Although most people with suspected coronary artery disease due to chest discomfort are psychologically healthy, some may feel anxious about undergoing an unfamiliar examination. This uneasiness activates their sympathetic nervous system, altering their HR and rhythm and resulting in an unsuccessful CTCA scan. Some physicians have shown that antianxiety drugs administered before CTCA examination improved coronary image quality, 15 further indicating that anxiety negatively affects CTCA.
At our center, the HR was measured for patients requiring a CTCA scan, and β-blockers might be given several days before a scan. However, an increasing HR might be a manifestation of anxiety. Methods for reducing patient anxiety could include allowing patients to visit the CT room in advance of their scan, keeping the room warm during the scan, and having the staff maintain a positive manner. Medications might be helpful, with antianxiety agents being a better choice than β-blockers.
This study has some limitations. Better results could be obtained by setting a detailed standard for CTCA image quality and analyzing the relationship with anxiety. Furthermore, to prove the effect of anxiety in CTCA, anxiety release should be measured prospectively in a random group of subjects.
In conclusion, the SAS standard score had a negative correlation with the success rate of 64-slice CTCA. The CT scan procedure itself may be a source of stress and may adversely affect CTCA image quality.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.