
Abstract
Objectives
Depression is one of the common mental health problems noticed in immigrants because of the experiences related to their resettlement which is the case for Somali population. Depression increases mortality, morbidity, disability, and costs of health care which can be controlled by screening depression in the primary care setting using a culturally and linguistically congruent screening tool. The aim of the current study is to translate the English PHQ-9 into Somali language using evidence-based translational methodology and establish psychometric properties of the Somali PHQ-9.
Methods
The initial validation of the Somali PHQ-9 was studied by comparing the original and back translation versions using the comparability and interpretability tool in a sample of 56 monolingual health care professionals. The reliability and validity of the Somali version were established by psychometric analysis in a sample of 47 bilingual health-care workers.
Results
Cronbach’s alpha was 0.79 for the Somali version with the inter-item correlation mean of 0.33 and item-to-total correlation mean in the range of 0.40–0.80 (p < 0.01). Pearson correlation for the item-to-item correlation between English and Somali version was between 0.70 and 0.93 (p < 0.01) with the paired t-test showing no significant difference between the item means.
Conclusions
The Somali PHQ-9 showed a good reliability, homogeneity, and internal consistency. The construct validity for the Somali PHQ-9 was also established showing that the Somali PHQ-9 has similar reliability and validity like the other translated versions of PHQ-9.
Introduction
According to World Health Organization (WHO), more than 350 million persons suffer from depression at any point in time, and nearly 800,000 commit suicide every year. 1 Depression affects all dimensions of life like physical, personal, social, and spiritual. In addition, it also increases mortality. 2 Even though depression could affect the quality of life, appropriate treatment can significantly improve the prognosis of the problem.3,4 A primary care practice serves as the patient’s first point of entry into the health-care system and most often is the first place where depression is diagnosed. 5 Many studies have confirmed that depression is indeed a frequent mental health problem faced in primary care.6–9 Hence having a process to screen, diagnose, and appropriately manage depression in primary care is inevitable and also recommended by USPSTF. 10 According to USPSTF, the PHQ-9 is the most common tool used in primary care for depression screening.
Refugees and immigrants are a very unique population because of the limitations due to cultural practices such as language barriers, race, and ethnicity which would significantly affect the screening, diagnosis, and treatment of depression.9,11–13 Many studies found that mental health services were underutilized by immigrants and refugees, especially in the Somali population.12,13 The diagnosis and management of depression is crucial to this vulnerable population but is significantly affected by the lack of culturally and linguistically appropriate standardized screening tools.11–13 In these circumstances, well-established methodology that has been followed in the literature is to translate an existing reliable and validated depression screening tool in one language to the language of the population that has to be studied.
Most of the studies involving translation of health-care instruments were centered on Brislin’s
14
forward and back translation methodology.
14
Also, many health-care organizations formulated a set of guidelines that combined all the major concepts.15–17 Following different translation methodologies and guidelines, the PHQ-9 has been translated and validated in different languages.9,18–23 There were no studies reported on the development of reliable and validated depression screening tools in the Somali language. Creating one using an evidence-based translation methodology will be very valuable providing the much needed mental health services and furthering mental health research in the Somali population. Hence, the objectives of this study are:
to translate the English version of the PHQ-9 to Somali using evidence-based translation methodology to study the reliability and validity of the translated Somali PHQ-9.
Methods
The study utilized a broadly acknowledged cross-cultural translation methodology16,24,25 which included three phases. Phase 1 started with the formation of an expert committee as recommended by WHO’s process of translation and adaptation of instrument. 17 It included four bilingual health-care professionals of which two were physicians, one was a nurse practitioner, and one was a medical assistant. The English language instrument was translated into the Somali language by three different bicultural translators. All the three translations were revised and reviewed by the committee to end up with one prefinal Somali version of the PHQ-9.
Phase 2 included the back translation into the original English language by an independent bilingual translator. 14 Following this, the initial validation of the preliminary Somali version of the instrument was carried out by comparing the original and the back-translated versions of the instruments by studying the interpretability and comparability of each item in the instrument using the tool developed by Sperber. 25 The questionnaire was answered by 54 monolingual volunteer study participants who were native English-speaking health-care professionals. The participants included 36 Doctorate of Nursing Practice students and 18 case managers who were registered nurses, social workers, and licensed psychologists. Based on the results, the items with discrepancies were revisited and revised.
Phase 3 involved the psychometric testing of the prefinal version of the Somali instrument to study the cultural and linguistic equivalence of the translated instrument.
Sample
The sample size for the psychometric analysis depends on the number of items in the instrument, and it is recommended to have at least five samples per item.26–28 Based on the recommendation, convenience samples of 47 bilingual voluntary participants were chosen as there were nine items in the PHQ-9 that were scored. The participants included registered interpreters and bilingual health-care professionals. The study was approved by the institutional review board of Frontier Nursing University.
Data collection
The data were collected during a period of 60 days at Gargar clinic in Minneapolis where a majority of Somali immigrants live in U.S. The participants were given both English and the Somali versions of PHQ-9. The order of questionnaire administration was random, to remove any bias toward one version of the questionnaire. Any missing data was replaced by the mean for that item.
Reliability and internal homogeneity
The psychometric analysis was carried out using SPSS software version 22. Since all the nine items of the Somali version of PHQ-9 are related to the evaluation of depression, the reliability was studied using Cronbach’s alpha and also by analyzing the internal consistency and homogeneity. The construct validity was studied using Pearson’s correlation between the item pairs in both versions. In addition, the paired t-tests were also studied to analyze the difference between the means of each item in translated Somali version compared to the means of each item of the original English version.
Results
Interpretability and comparability results
The original English and back-translated Somali versions were tested using a sample of size n = 54. The comparability of language and similarity of interpretation of the item pairs were analyzed separately. Both comparability and interpretability scales have scores that range from a minimum of 1 to a maximum of 7. 25 In general, for a given item, the value of mean >3 necessitates a revision of that item. In the case of the interpretability scale, if the item mean >2.5, then the item is likewise included for possible revision. 25
Interpretability and comparability survey results.
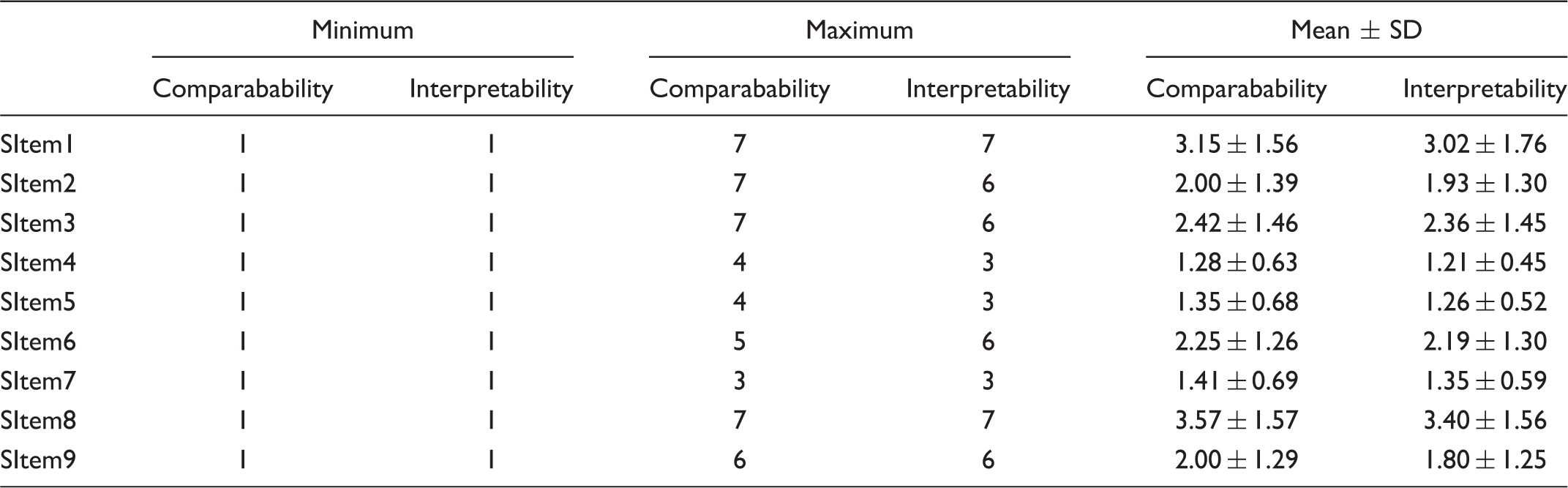
n = 54; SD: standard deviation.
Descriptive results
The total PHQ-9 score ranges from 0–27. The cutoff scores for different stages of depression were recommended by Kroenke, Spitzer, and Williams. 30 In the current study with 47 bilingual participants, based on the results of the validated English version, it was found that 6.4% and 19.2% had moderate and mild depression levels, respectively. Compared to all the items, item 3 about sleep, item 4 regarding tiredness and energy, and item 5 regarding eating dominated the total score for many participants. On analyzing the depression levels for the patients who scored more in items 3, 4, and 5, it was found that out of 40.42% of participants who scored >0 for item 3, 34.04% were in the mild category and 6.38% were in the moderate category. In the case of item 4, 51.06% scored >0 of which 44.68% were in the mild category while 6.38% were in the moderate category. For item 5, 38.29% scored >0 in which 31.91% were in the mild, and 6.38% were in moderate categories, respectively.
Reliability results
Mean, Cronbach’s alpha, items mean, and inter-item correlation mean for English and Somali versions of PHQ-9.

n = 47; SD: standard deviation.
The acceptable value of Cronbach’s alpha is reported to be in the range of 0.70–0.8024,26, and hence both English and Somali versions are both reasonably reliable.
Inter-item correlation—English version.
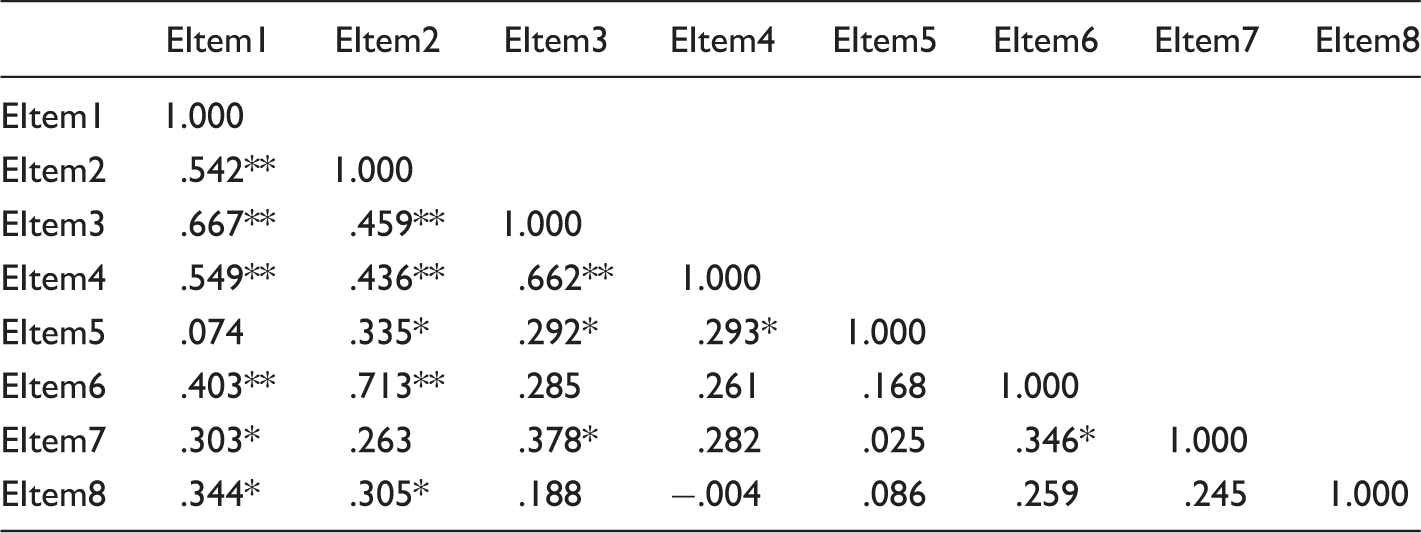
p < 0.01, *p < 0.05.
Inter-item correlation—Somali version.
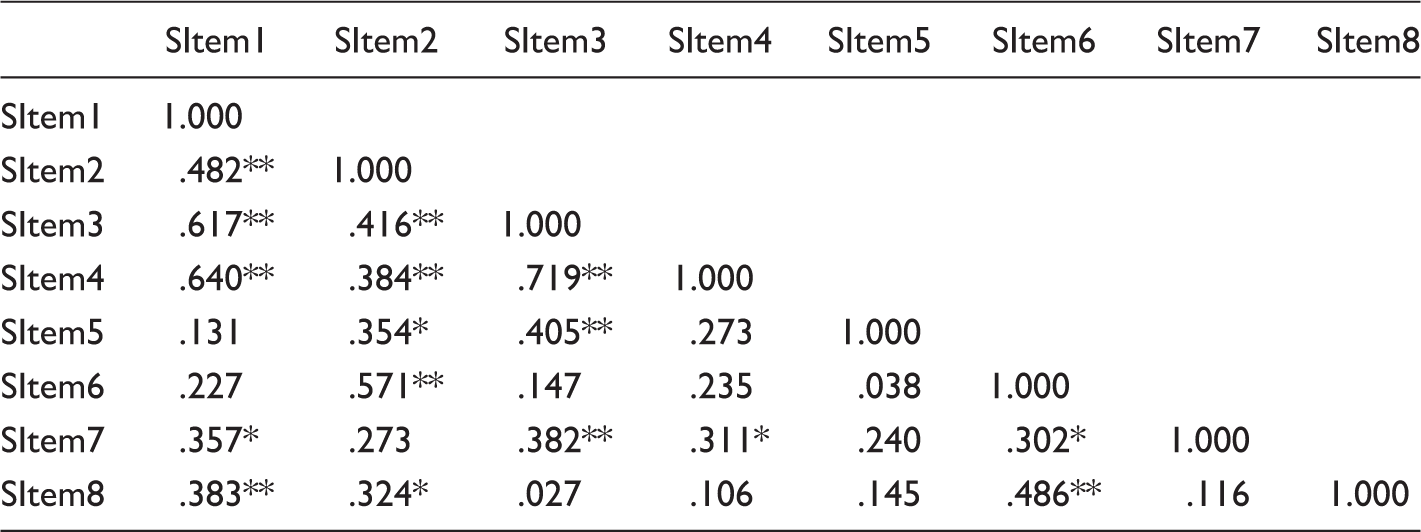
p < 0.01, *p < 0.05.
Item to total correlations mean.
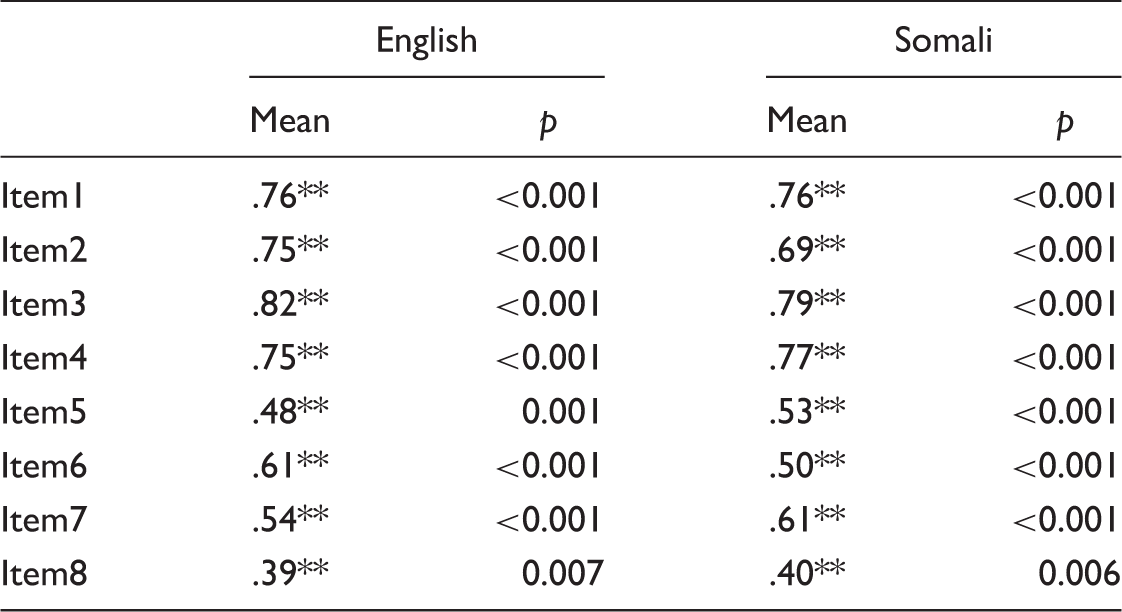
n = 47; ** p < 0.01.
Validity results
English and Somali items correlation.
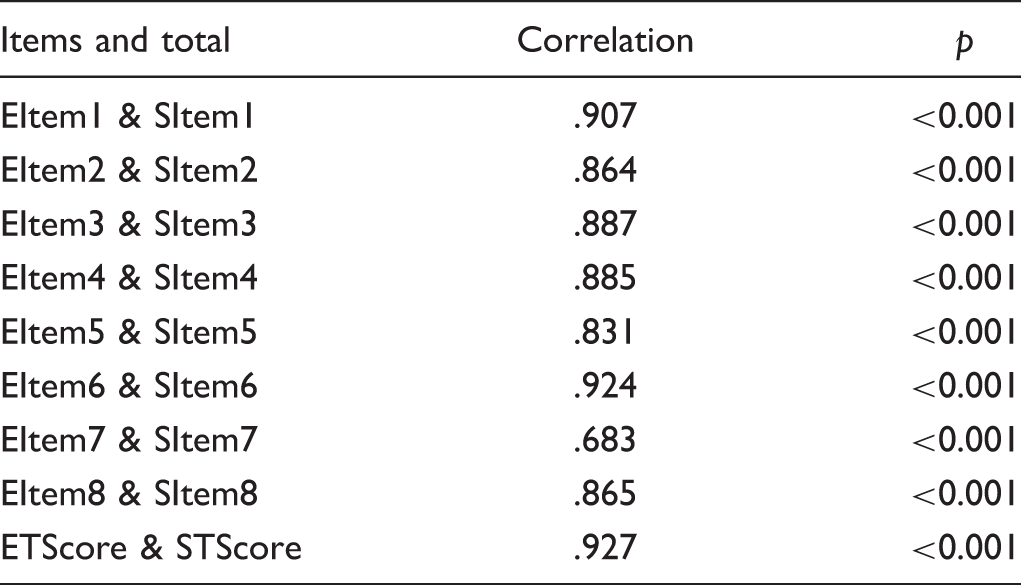
n = 47.
All the items had a strong correlation >0.83 except item 7 which had a moderate correlation of 0.68. 24
Also, the items mean was tested for the differences using paired t-test. The null hypothesis was that the item means of both Somali and English versions did not have any difference.
Item means comparison (paired t-test) between English and Somali versions.
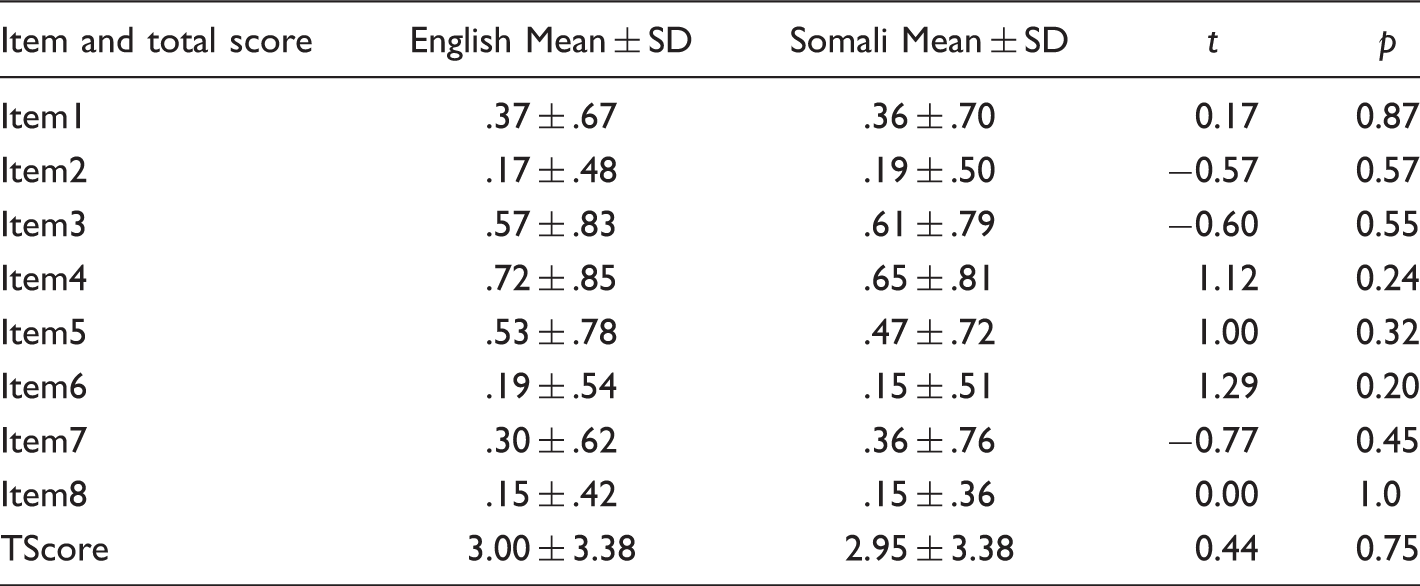
TScore: total score; SD: standard deviation.
Discussion
A self-administered Somali PHQ-9 is crucial in screening depression in the primary care practice with Somali patients. It will eliminate the interpreter bias and protect patient privacy. Further, it will also significantly reduce the time and personnel needed to complete the depression screening as recommended by USPSTF 10 to improve depression identification in primary care setting. The results obtained by utilizing the Somali PHQ-9 score at the primary care level would help in initiating the conversation with the patient about the effects of untreated depression. The results would help in diagnosing depression and delivering the appropriate evidence-based depression care and thereby increases the utilization of mental health services by this population. Further, the PHQ-9 score would also serve as a baseline to assess the prognosis in Somali patients.
Elements of different evidence-based cross-cultural translation methodologies were combined to develop an elaborate design which incorporated the translation, back translation, and bilingual testing processes. The current study included a unique step in the translation methodology by adopting the interpretability and comparability tool developed by Sperber 25 to study the initial validation of the translated version. It also used the expert committee consensus approach at all stages of the translation process as recommended by WHO 17 followed by the detailed psychometric analysis to study the validity and reliability of the translated instrument.
The current study demonstrated that the developed Somali PHQ-9 has a significant reliability of Cronbach’s alpha = 0.79. Similar reliability results were observed by other translated versions of PHQ-9 like Swahili, Thai, and Haitian Creole PHQ-9.20,21,23 The reliability is slightly lower than the Korean, Chinese, and Sinhala PHQ-9.9,19,22 However, it was found that the Somali and English version had similar reliability in the studied population endorsing the accuracy of the translation.
The construct validity analysis showed a strong association between Somali and the original English version and no significant mean differences were found between the scores for all the items included in the analysis. This clearly showed that the Somali version is valid and reliable. To the author’s knowledge, this is the first of its kind to investigate the reliability and validity of the Somali version of PHQ-9.
Although the study did not focus on depression prevalence in the sample population, the administration of the validated English version for the psychometric testing had some interesting observations. The prevalence of depression was found to be 25.6% in which 19.2% had mild depression in the bilingual sample population. Similar results were reported by Shim, Baltrus, Ye, and Rust, 4 where the depression prevalence was 20.1 in adults aged 18 and older, and a greater number had mild depression symptoms. The depression prevalence in the studied Somali population is slightly lower than the depression prevalence rate (38.3%) noted among the Somali refugees at Melkadida camp, South East Ethiopia. 29 The lower prevalence may be because the studied population was successfully resettled in the US. In addition, it was also found that more than 30% of the sample population who had mild depression, scored >0 on questions regarding sleep, energy, and appetite which has been observed earlier. 21 According to Kroenke, 30 around 33% of somatic symptoms are not explained medically. Also, it was found that depression anxiety and somatization are frequently observed to overlap in the primary care population. 31 This shows that somatization is a prominent component which has to be studied in the Somali population and is left for the future research.
Limitations
The study sample size was small and was in a selected bilingual interpreters and health-care providers and hence cannot be generalized to the whole Somali population. Several studies have demonstrated20,21,23 that the reliability of the same tool can differ based on age, socio-economic status, literacy, and comorbidities. There was no baseline demographic data collected in this study, and hence the specificity and the sensitivity of the tool cannot be established. This study was limited in information related to qualitative nature of PHQ-9.
Compared to the translation methodologies for conceptual equivalence that uses both qualitative and quantitative approaches, 32 the current study is limited to the quantitative methodologies. Since the participants were aware that the focus of the study was to test the reliability and validity of the translated PHQ-9, they might have under-reported depression symptoms, and hence the prevalence of depression observed may not reflect the actual prevalence. Because of concurrent administration of English and Somali version, the sample might have been biased towards one language even though a random sequence of administration was followed in the current study.
Conclusions
Thousands of vulnerable Somali refugees and immigrants who are displaced because of civil war and effects of drought are resettled elsewhere in English-speaking countries. The lived experiences of civil war and life in refugee camps made this population vulnerable to depression. Many from this community receive care from primary care clinics. Pertinent to this establishing a process of effective depression screening which is culturally and linguistically appropriate is a definite need. In the current study, a Somali PHQ-9 was developed by translating and culturally adapting the English PHQ-9 using evidence-based translation methodologies. The psychometric study showed that the Somali PHQ-9 has significant reliability and validity. The translated tool, when used in primary care, could increase the identification of depression. The tool can be self-administered and so would provide privacy to the patients, eliminate the fear of stigma, and would be easier and time effective than using the current method of using an interpreter to administer the English PHQ-9. The Somali PHQ-9 has a wide scope of administering to a larger population which could help study the epidemiological data related to depression in Somali population and design personalized depression care delivery.
Footnotes
Acknowledgments
The authors wish to thank the expert committee members Dr Nimo Abdi, Dr Layla Warsame, and Ms Hayat Ahmed for their valuable discussions.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.