
Abstract
Introduction
Balint group discussions provide learning opportunities for many of the competencies and milestones put forward by the Accreditation Council for Graduate Medical Education. The current literature is mixed concerning the effect of Balint groups on communication skills and professionalism.
Aim
To map the content of the Balint discussion to the competencies and milestones put forward by the Accreditation Council for Graduate Medical Education.
Results
Only four narratives were submitted. Additional cases were recruited through literature review of published Balint discussion cases. A total of 25 cases were rated by the committee. There was agreement between three out of four raters on at least one core milestone in every case. The most frequent milestones were C1 (develops meaningful therapeutic relationships with patients and families), C2 (communicated effectively with patients, families, and public), Prof1 (completes a process of professionalization), and Prof3 (demonstrates humanism and cultural proficiency). Balint groups provided a learning opportunity for a subset of milestones in at least 36% of the cases.
Conclusion
This pilot research suggests that Balint groups and the discussions of complex and challenging cases provide learning opportunities for multiple family medicine milestones, mainly communication skills and professionalism. Further research is needed to refine the methodology and the rating system.
Introduction
Balint groups are regular seminar-based discussions of the patient–doctor relationship performed in many residency programs. Balint groups are usually comprised of 6–10 residents that are led by one or two facilitators. One resident would present a case without preparation for 5–10 min. Usually they are asked to present a case that troubles them. The resident presents the case briefly and group members are allowed to ask for clarifying questions for 5 or so minutes. Then the presenter will sit back and listen to the conversation. The group will take the case and the conversation will focus on the patient–doctor relationship minimizing the discussion of medical management. The leaders help the group to explore the emotions and thoughts of the physician and patient. The leaders will facilitate the discussion so that it addresses the physician’s and patient’s perspectives, their treatment alliance, and the role of the physician.
The current literature is scarce and mixed concerning the effect of Balint groups on communication skills, empathy, behavioral medicine, and professionalism.1–4 In a recent literature review about research in Balint groups, Van Roy et al. found that methodological shortcomings exist in the published literature. These include small samples, lack of control groups in quantitative studies, and lack of a systematic approach in qualitative studies. 5 However, analysis of Balint sessions revealed the following themes: building professional identity, cooperation with other medical professionals, managing difficult human relationships, incurable patients, privacy and profession, role confusion, and value conflict. 6 In a recent survey of US Family Medicine residency programs, the objective of Balint training was considered mainly to understand the patient as a person and help physicians resolve professional role conflict. 7
In 2014, the Accreditation Council for Graduate Medical Education (ACGME) completed a multiyear development and review process for their Next Accreditation System which culminated in the release of competency milestones to be used for evaluation of resident physician progress in all residency programs. Balint group leaders intuited that the discussions in Balint groups provide a learning opportunity for many of the competencies and milestones put forward by the ACGME. The aim of this study was to develop a research protocol to map the content of Balint group discussions to the ACGME competencies through the use of narratives that summarized the discussion rated by an expert panel.
Methodology
Phase 1
In February 2015, the research team of five Balint leaders was formed. The research team members submitted narratives of 18 case discussions of their own Balint groups. Each member reviewed the cases and identified from the Family Medicine Milestone Project milestones the ones that were relevant to the narrative. The process was repeated and refined repeatedly over one year with discussion among the research team members about how they chose one subcompetency over the other to refine the process. The team agreed on the following:
The narrative should include a description of the presented case and issues discussed. It was agreed that the parameters of the narrative should be kept open and unstructured to avoid bias. The list of the subcompetencies and levels is extensive and sometimes not clearly defined. It was difficult to pinpoint a detailed behavior from a general description of the discussion, so a final list of the general subcompetencies was chosen to pick from (see Appendix 1). Each member would rate the narrative as a learning opportunity for specific subcompetencies. Each member would choose the top 3 most salient subcompetencies.
The analysis of the ratings of the cases showed that there was agreement on at least one “core” subcompetency in every case. The top 3 subcompetencies agreed on by the majority were in the communication and professionalism competency areas: C1, C2, and Prof3. To further guard against bias, the research team invited a nonmember who was familiar with milestones and competencies and was not a Balint leader to rate the narratives. His ratings were in concordance with the research team.
Phase 2
Phase 2 established the methodology protocol. In April 2016, phase 2 was planned to recruit narratives from a list of the American Balint Society (ABS) credentialed Balint leaders. An invitation was sent through the Credentialed Leaders Listserve of the ABS to ask the credentialed Balint leaders to volunteer and submit narratives about Balint groups that they have led, or were leading, with residents. They were not informed about the study objectives to avoid bias in the cases they selected to submit. Their participation was anonymous. The participants were asked to submit up to 10 narratives of 250 words. They were given an example of a narrative that described the details of the presented case and issues discussed (Box 1).
Examples of narratives.
Issues addressed: discussed how being afraid distracted the doctor from helping that man; some even did not want to take care of him again because of fear; discussed how to gain trust of the patient in order to help him; felt empathy with the patient’s struggle and the inability to go to a rehabilitation center as no one will remain to take care of his family.
Issues addressed: exploring patient autonomy and self-determination versus a physician’s beliefs; balancing the personal feelings with the professional desire to support patient’s autonomy and assisting patient in making an informed decision; supporting the physician’s feelings with respect to the internal values conflict she experienced; communication skills related to providing educational information about abortion, family planning, that is consistent with current state law.
Rating of the narratives
A committee of four experts was formed. Three of the experts were both Balint leaders and members of their clinical competency committees (CCC). One of the experts was a member of his CCC but without any Balint experience. They reviewed the narratives individually and chose from a list of subcompetencies (Appendix 1) where the group discussion best corresponded with a learning opportunity for that subcompetency.
Sample size
We hypothesized that at least one subcompetency would be recurrent in 75% of the cases. With 95% confidence interval and 15% desired precision, a sample size of 33 was needed. Therefore, we attempted to solicit at least 35 narratives.
Data analysis
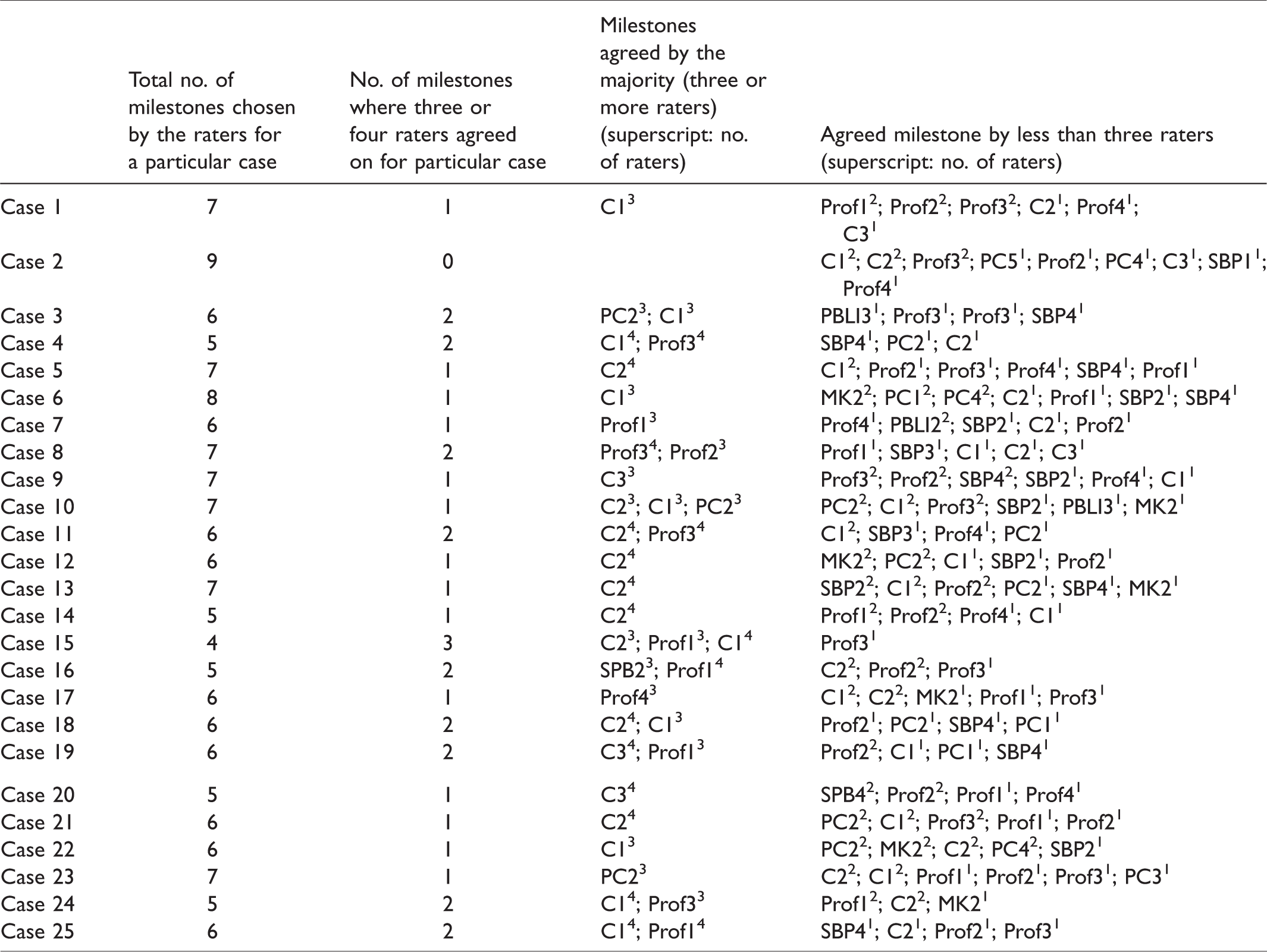
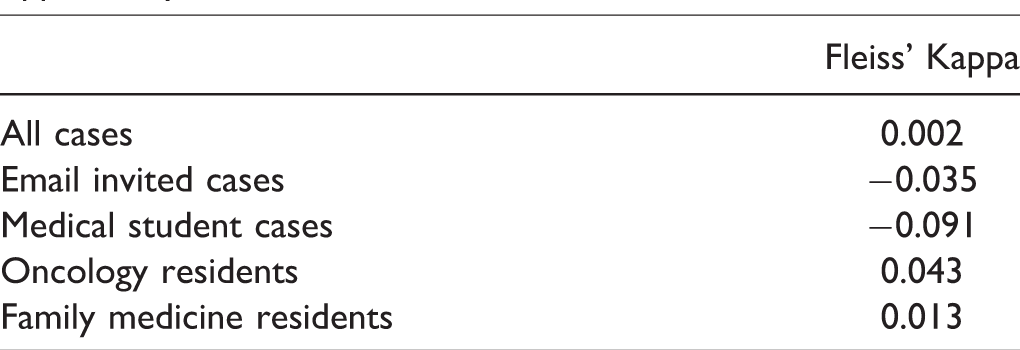
For each narrative, the subcompetencies where three or four of the raters agreed on were captured. Frequencies of the above subcompetencies were calculated. Fleiss Kappa for multiple coders was calculated to measure the interrater reliability among all cases.
Results
Only four narratives were submitted from credentialed Balint leaders. Therefore, a literature review was conducted and three articles were found that published Balint discussion cases.6,8,9 The setting of the cases differed among the three different articles: medical students, family medicine residents, and oncology residents. A total of 25 cases were rated by the committee.
On average, each case was considered to provide learning opportunities for six subcompetencies. There was agreement between three out of four raters on at least one core subcompetency in every case (range 1–3) (see Table 1). The most frequent subcompetencies were C1 (develops meaningful therapeutic relationships with patients and families), C2 (communicated effectively with patients, families, and public), Prof1 (completes a process of professionalization), and Prof3 (demonstrates humanism and cultural proficiency) (see Table 2). Balint groups provided a learning opportunity for a subset of subcompetencies in at least 36% of the cases.
Distribution of milestones for each narratives.
Frequency of specific milestones agreed upon by three or four of the raters.
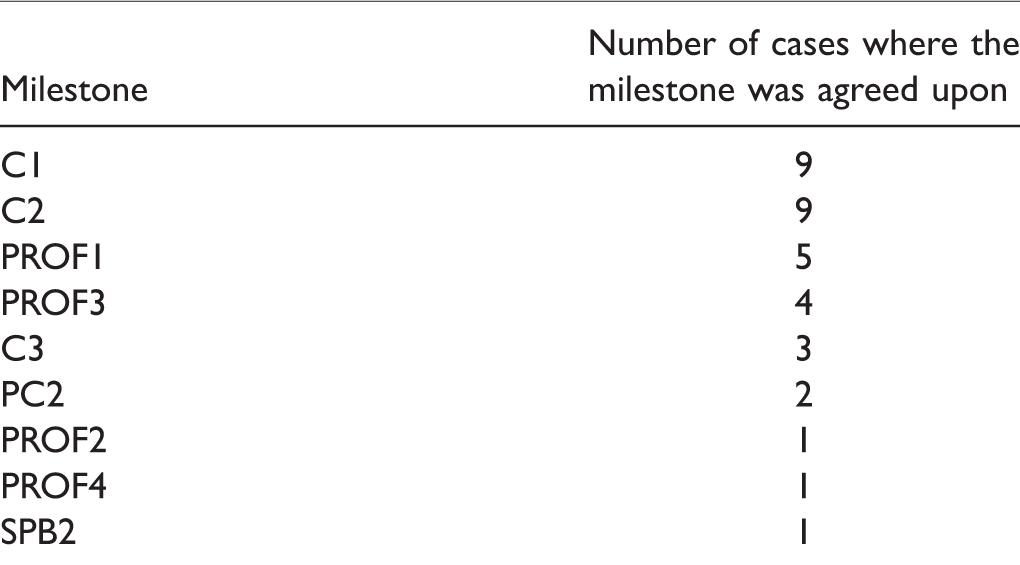
Table 3 shows the interrater reliability among the four raters for all the cases. There was slight agreement between the raters for all the cases. There was mild discrepancy in the interrater agreement among the different sources of the cases. The level of pairwise agreement with the Balint naive rater was the same as with the credentialed leaders.
Interrater reliability among the four experts on choice of milestone for which the Balint seminar provides a learning opportunity.
Discussion
This pilot study showed that Balint groups provide a competency-based learning opportunity for communication skills and professionalism as they are detailed in the ACGME Family Medicine Milestones. Of the cases reviewed for this study, two-fifths demonstrated support for communication skills and one-fifth for professionalism competencies. There were 10 cases that demonstrated other competencies such as system-based learning, and medical knowledge and patient care competencies as agreed upon by two raters.
Teaching professionalism to residents relies mainly on role model and hidden curriculum. 10 Other methods of teaching professionalism include short didactic lectures spread over 6 h/year.11,12 Similarly, most family medicine residency programs use lectures and experiential methods to teach communication skills mixed with direct observation and small group work. 13 The authors suggested that family medicine residencies should seek to establish more learning opportunities to teach communications. Balint group case discussions provide a variety of practice for these skills. Teaching communication skills and professionalism is most beneficial when it occurs longitudinally and involves multiple teaching methods in multiple settings (outpatient clinic, hospital, and community). Balint groups help programs accomplish these aims since cases can be presented from a variety of settings and the training can begin in the first months of residency and run throughout. The frequency of biweekly Balint groups allows for more time allotted for residents to learn professionalism and communication skills during their residency. That Balint groups can provide learners with the opportunity for experiential learning for multiple competencies might encourage some family medicine programs that the benefits of Balint groups outweigh the high demand for resources, mainly Balint leaders and allotment of time for frequent meetings.
Limitations
The raters did not attend the Balint group sessions and relied on a brief description of the cases presented and issues discussed. This, alongside with the small sample size, could have contributed to the low interrater reliability coefficients. While this was a pilot investigation where exploration of suitable rating methodologies was considered part of the research process, the lack of a defined rating system for cases or a uniform type of case submission guideline may have contributed to lower interrater agreement than we expected. Finally, from its inception, the ACGME describes the milestones as “living document” which lends to its flexibility and adaptability, the broad language and uneven clarity of some of the milestones that make up the subcompetencies compounded the difficulty of rating Balint case descriptions.
This work relied on Balint leader description of the learning opportunity. Testing the validity of the research methodology could be enhanced by rating an audio recording of the discussion. We used multiple raters with diverse cases discussion to empower the validity of the results. Further steps will attempt to increase the number of cases.
Black box warning
This study focused on Balint leader perceptions and on learning opportunities rather than mastery, in part because of the importance of protecting Balint group self-disclosures from being used in evaluations of resident performance. Given the learning opportunities, our fear is that it might be tempting to use Balint discussions to evaluate resident’s understanding and implementation of milestones. It is the strong opinion of the authors that the effectiveness of Balint groups depends on safety afforded by confidentiality. Balint group members have to be free to admit their misgivings, confusion, and feelings of incompetence in order for the group to facilitate learning and growth. Any evaluation of residents in Balint group other than attendance would undermine the process significantly.
Conclusions
This pilot research suggests that Balint groups and the discussions of complex and challenging cases provide learning opportunity for multiple family medicine subcompetencies, mainly communication skills and professionalism. This work is preliminary yet it represents an important initial attempt to link Balint group work and Balint case content with the FM milestones. Refinement of the methodology and rating system for examining these connections can help underscore the value of Balint to residency training as well as interdisciplinary team-based care across multiple settings.
Appendix 1. List of the competencies and its subcompetencies as provided by the ACGME
Patient Care (PC)
PC-1. Cares for Acutely Ill or Injured Patients in Urgent and Emergent Situations and in All Settings PC-2. Cares for Patients With Chronic Conditions PC-3. Partners With the Patient, Family, and Community to Improve Health Through Disease Prevention and Health Promotion PC-4. Partners With the Patient to Address Issues of Ongoing Signs, Symptoms, or Health Concerns That Remain Over Time Without Clear Diagnosis Despite Evaluation and Treatment, in a Patient-Centered, Cost-Effective Manner PC-5. Performs Specialty-Appropriate Procedures to Meet the Health Care Needs of Individual Patients, Families, and Communities, and Is Knowledgeable About Procedures Performed by Other Specialists to Guide Their Patients’ Care
Medical Knowledge (MK)
MK-1. Demonstrates MK of Sufficient Breadth and Depth to Practice Family Medicine MK-2. Applies Critical Thinking Skills in Patient Care
Systems-Based Practice (SBP)
SBP-1. Provides Cost-Conscious Medical Care SBP-2. Emphasizes Patient Safety SBP-3. Is an Advocate for Individual and Community Health SBP-4. Coordinates Team-Based Care
Practice-Based Learning and Improvement (PBLI)
PBLI-1. Locates, Appraises, and Assimilates Evidence From Scientific Studies Related to the Patients’ Health Problems PBLI-2. Demonstrates Self-Directed Learning PBLI-3. Improves Systems in Which the Physician Provides Care
Professionalism (PROF)
PROF-1. Completes the Process of Professionalization PROF-2. Demonstrates Professional Conduct and Accountability PROF-3. Demonstrates Humanism and Cultural Proficiency PROF-4. Maintains Emotional, Physical, and Mental Health, and Pursues Continual Personal and Professional Growth
Interpersonal and Communication Skills (C)
C-1. Develops Meaningful, Therapeutic Relationships With Patients and Families C-2. Communicates Effectively With Patients, Families, and the Public C-3. Develops Relationships and Effectively Communicates With Physicians, Other Health Professionals, and Health Care Teams C-4. Uses Technology to Optimize Communication
Footnotes
Acknowledgment
The authors wish to thank Dr Mark Corey for his valuable help in matching the narratives to the subcompetencies.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.