
Abstract
Objective
To examine the prevalence of depression, anxiety, attachment issues, and associated factors among pregnant women hospitalized on an antepartum unit.
Method
Ninety-eight women hospitalized on an antepartum unit reported demographic and social information and were evaluated with screening tools for depression, anxiety, and maternal–fetal attachment. Data were analyzed using descriptive statistics and logistical regression analysis.
Results
Over one third (36%) of participants screened at risk for depression. Almost half (47%) reported elevated state anxiety and over one third (37%) reported elevated trait anxiety. Depression and anxiety were frequently comorbid. Positive screens for depression and anxiety were associated with decreased maternal-fetal attachment. Those who screened at risk for depression and anxiety in this sample often had a personal or family history of depression or anxiety or a history of intimate partner victimization. Substance use was common among those with elevated anxiety. Only a minority (15%) of at-risk participants had been referred to mental health treatment.
Conclusions
Women hospitalized on antepartum units had an elevated risk of depression and anxiety. Depression and anxiety were strongly comorbid in this population. Screening efforts to increase detection of perinatal depression and anxiety are recommended on obstetrical antepartum units.
Keywords
Introduction
Antepartum depression is a condition with a prevalence of between 7% and 13%.1,2 The most significant risk factor is a personal history of depressive illness. Other known risk factors include a family history of depression, developmental trauma, age under 20 years, having more than three children, cigarette smoking, life stress, lack of social support, intimate partner violence victimization, lower income, and lower level of education.3–5 In addition to being a common disorder, antepartum depression is also increasingly recognized as having potential adverse effects on obstetrical and infant outcomes. Preterm delivery, low-birth weight, altered neonatal behavioral scores, and delayed development in offspring have all been associated with antepartum depression.6–8 A growing body of literature considering fetal neurodevelopment has illustrated an association between antepartum depression and altered development at its earliest stages. A recent systematic review concluded that untreated antepartum depression may be associated with fetal hyperactivity and irregular fetal heart rate, markers for alterations in neurodevelopment. 9 Antepartum depression is also associated with lower levels of maternal–fetal attachment,10–12 which has been associated with reduced investment in healthy parenting practices and an increased risk of disrupted maternal–child attachment patterns.
Although peripartum anxiety disorders have received comparatively less attention, recent findings indicate that anxiety is common during the peripartum period and highly comorbid with depression. Wisner et al. found that among postpartum women diagnosed with depression after a positive screen, almost two thirds had a comorbid anxiety disorder. 5 As comorbid anxiety disorders in the general population increase the probability of being refractory to depression treatment, 13 this high rate of comorbidity is concerning. Furthermore, as Yonkers et al. recently found that comorbid diagnoses of antepartum major depression and post-traumatic stress disorder increase risk for preterm delivery beyond what could be expected by either mood or anxiety symptoms alone, it is also possible that this comorbidity adds to the obstetrical and developmental risks in a synergistic manner. 14
Despite the prevalence and risks of antepartum depression and anxiety, studies based in obstetrical offices have shown that without universal screening, these conditions are often unrecognized.15,16 For this reason, in 2015, the American College of Obstetricians and Gynecologists recommended that obstetricians offer universal screening for depression and anxiety at least once during the peripartum period. 17
Studies on antepartum depression among high-risk obstetrical patients are sparse but do support a prevalence rate above that of the general obstetrics population. Two recent studies focused on women hospitalized for obstetrical risk found that 27% to 44% screened at risk for depression.18,19 Potential risk factors included a personal history of depression, interpersonal relationship dissatisfaction, low level of education, and older age.18,19 Although a past mental health diagnosis predicted depression symptoms (OR 4.54) in one study, it is notable that 21% of those who screened positive for depression had no history of previous mental health diagnoses. 18 In another study, a strong maternal–fetal attachment was associated with fewer depressive symptoms in women hospitalized for obstetrical risk. 19 The risks of untreated depression must be weighed against the risks of various forms of treatment. 20
The purposes of this study were to examine how commonly women hospitalized on an antepartum unit screened as being at risk for depression, experienced state or trait anxiety, and attachment issues; and to describe common characteristics among those women who screened positive. The hypotheses included that (1) the prevalence of depression and anxiety would be higher for women hospitalized on the antepartum unit than has been reported for the general pregnant population, (2) there would be a high level of comorbidity between depression and anxiety symptoms, and (3) both depression and anxiety symptoms would be associated with a lower level of reported maternal–fetal attachment.
Methods
Participants
After approval by the institutional review board of University Hospitals Cleveland Medical Center, eligible women admitted to University Hospitals MacDonald Women's Hospital antepartum unit were invited to participate. Data for this study were collected from January to November 2016. Of 166 women approached for study recruitment, 41 declined and 27 consented but did not complete the packet. The final study sample included 98 participants.
Inclusion/exclusion criteria
All English-speaking women over the age of 18 years hospitalized in the antepartum unit were eligible. Women hospitalized for intrauterine fetal demise were excluded due to concern that a measure might create additional distress. Those who were unable to communicate in English were excluded due to limitations of personnel. If hospitalized multiple times over the course of their pregnancy, subjects were recruited only once.
Measures
All of the women were evaluated with a set of screening tools that included the Edinburgh Postnatal Depression Scale (EPDS), The State-Trait Anxiety Inventory (STAI), and the Maternal Antepartum Attachment Scale (MAAS).
The EPDS is a 10-item self-report measure that is the most widely used screening tool for peripartum depression. The EPDS has been validated for use in both the antepartum and postpartum populations. The scale includes statements describing various symptoms of depression and anxiety that range from 0 (low) to 3 (high) in accordance with either severity or frequency. Total EPDS scores range from 0 to 30. 21 The EPDS has varying cut-off scores of either ≥10 or ≥12 in the peripartum depression literature. As a result of this discrepancy, both cut-off scores were used for data analysis.
The STAI is a two part 40-item scale that is used to assess both state and trait anxiety symptoms. Items are rated on a four-point scale with higher scores indicating greater anxiety. State anxiety (Y1) refers to the emotional response that arises in the face of threatening situations or events, and trait anxiety (Y2) refers to the individual differences in personality that account for that response to threatening events and situations. A STAI score
The MAAS is a 19-item scale that focuses on maternal attitudes and feelings of bonding and attachment toward the fetus. Scores range from 19 to 95, where higher scores indicate higher level of maternal–fetal attachment. 23 The MAAS has subscales of “Quality” and “Intensity.” The “Quality” subscale assesses for a mother’s strong internal representations and positive emotions toward the fetus, while the “Intensity” subscale assesses the amount of time the mother spends thinking about and talking to the fetus.
Additionally, each woman self-reported demographic characteristics including personal and family history of anxiety and depression, marital status, education level, support system, race, and whether or not their pregnancy was planned. Additional information obtained via medical records included pregnancy history, length of stay, admission purposes, and birth outcomes. Information on sociodemographic status was drawn by comparing the income level of the participants’ reported zip code to federal poverty level guidelines.
Procedures
Study investigators visited eligible participants in their hospital rooms on Mondays thru Fridays to introduce the research. After obtaining informed consent, each participant was given a packet of self-report measures. Research investigators completed medical chart review. Any participant who screened above 12 on the EPDS was offered a referral to a mental health provider and provided with educational resources.
Analysis
The data were analyzed using SPSS version 24. Descriptive statistics were computed, and cross-tabulation examined the relationships between depression, anxiety, and maternal–fetal attachment. Binomial logistic regression was used to determine whether positive screening on STAI and EPDS could be predicted. Variables were included in the logistic regression analysis based on whether or not they approached statistical significance in the univariate analysis and hypotheses based on clinical experience that suggested these factors helped differentiate those with depression and anxiety symptoms. We similarly used Pearson correlation for bivariate correlation of continuous variables. As the peripartum depression literature varies in the cut-off score used for the EPDS, with some studies using a cut-off of 10 and others a cut-off of 12, analysis was done during both ≥10 and ≥12 as a cut-off.
Results
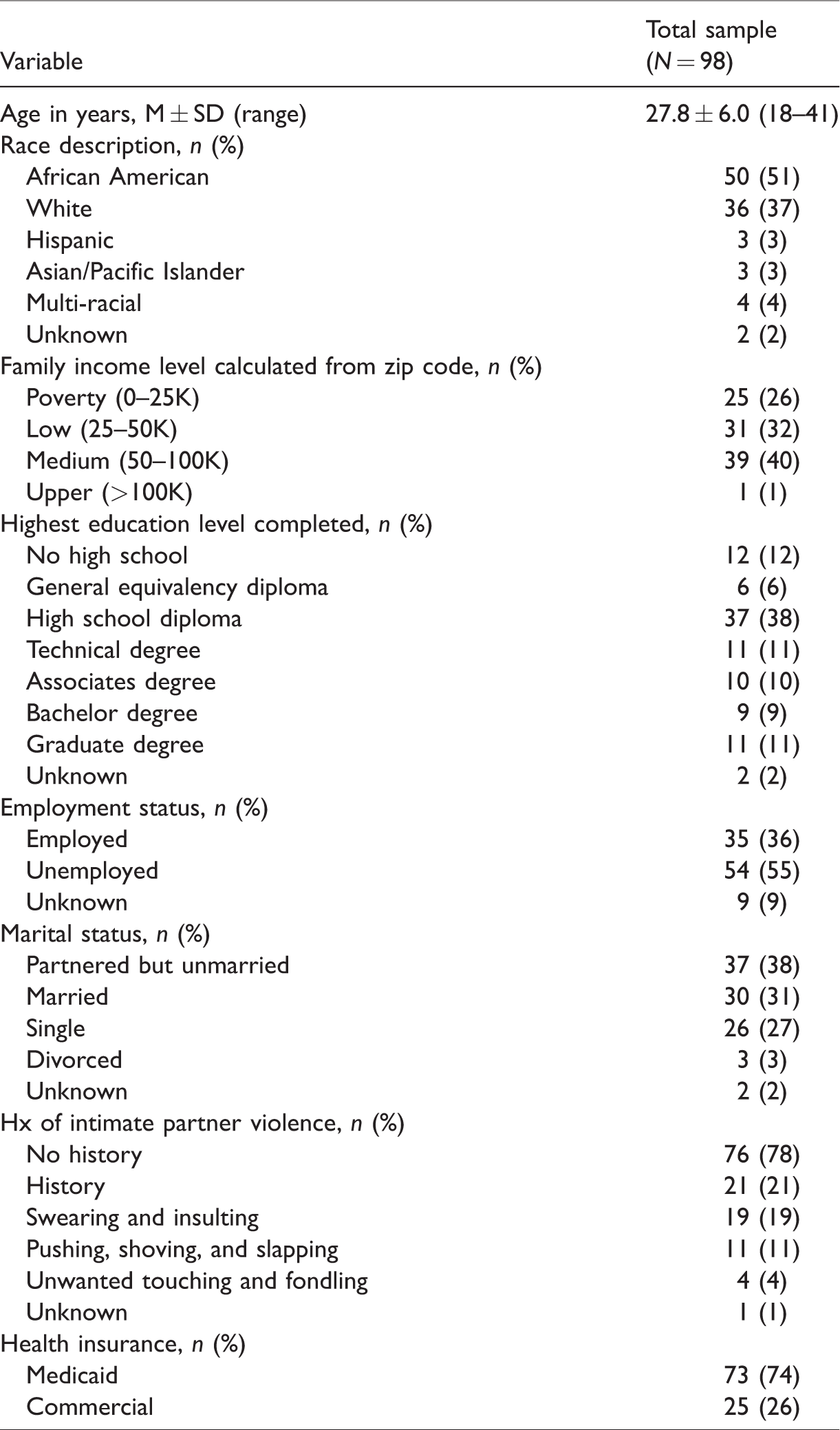
The study included 98 pregnant participants between the ages of 18 and 41 years (mean = 27.8, SD = 6.0; Table 1). There was a spread among income levels, which included poverty (26%), low income (32%), and medium income (40%). The majority of participants (51%) identified as African American. Most (55%) reported being unemployed at the time of admission. Over half (56%) reported an education level of high school diploma or less. Twenty-one percent of women enrolled reported experiencing some type of intimate partner violence, with the most commonly reported being a history of swearing or insults from their partners.
Sociodemographics of participants.
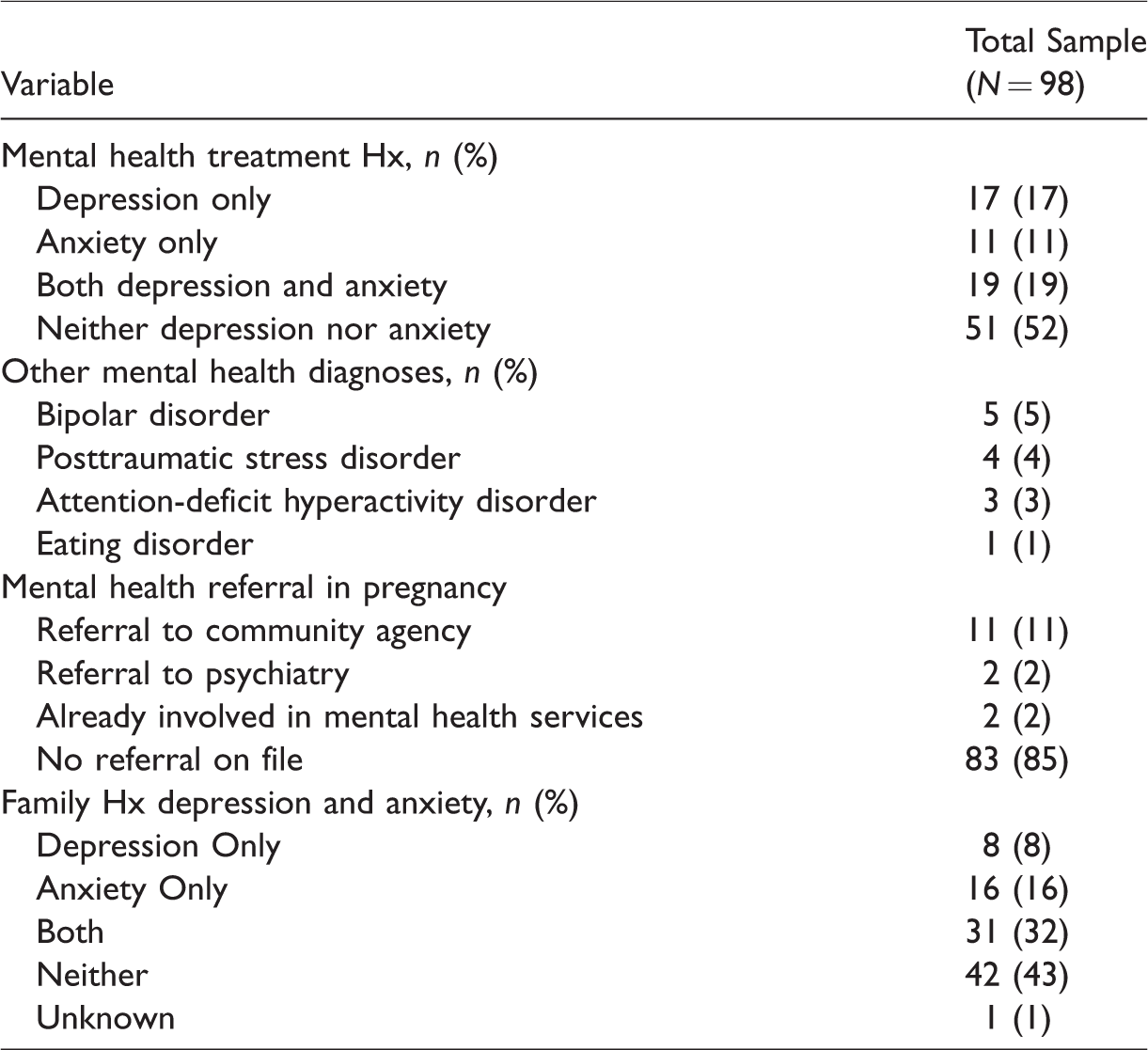
Although almost half (47%) reported having received treatment for anxiety or depression in the past, only 2% were currently enrolled in mental health services (Table 2). Most of the sample (56%) reported having a family history of either anxiety, depression, or both. A small minority (15%) of participants who screened positive for either depression or elevated anxiety had been referred for mental health treatment by their obstetrics team at the time of their research visit. Alcohol and tobacco use were uncommon in the sample, with only 2% and 5% reporting their uses, respectively.
Psychiatric history.
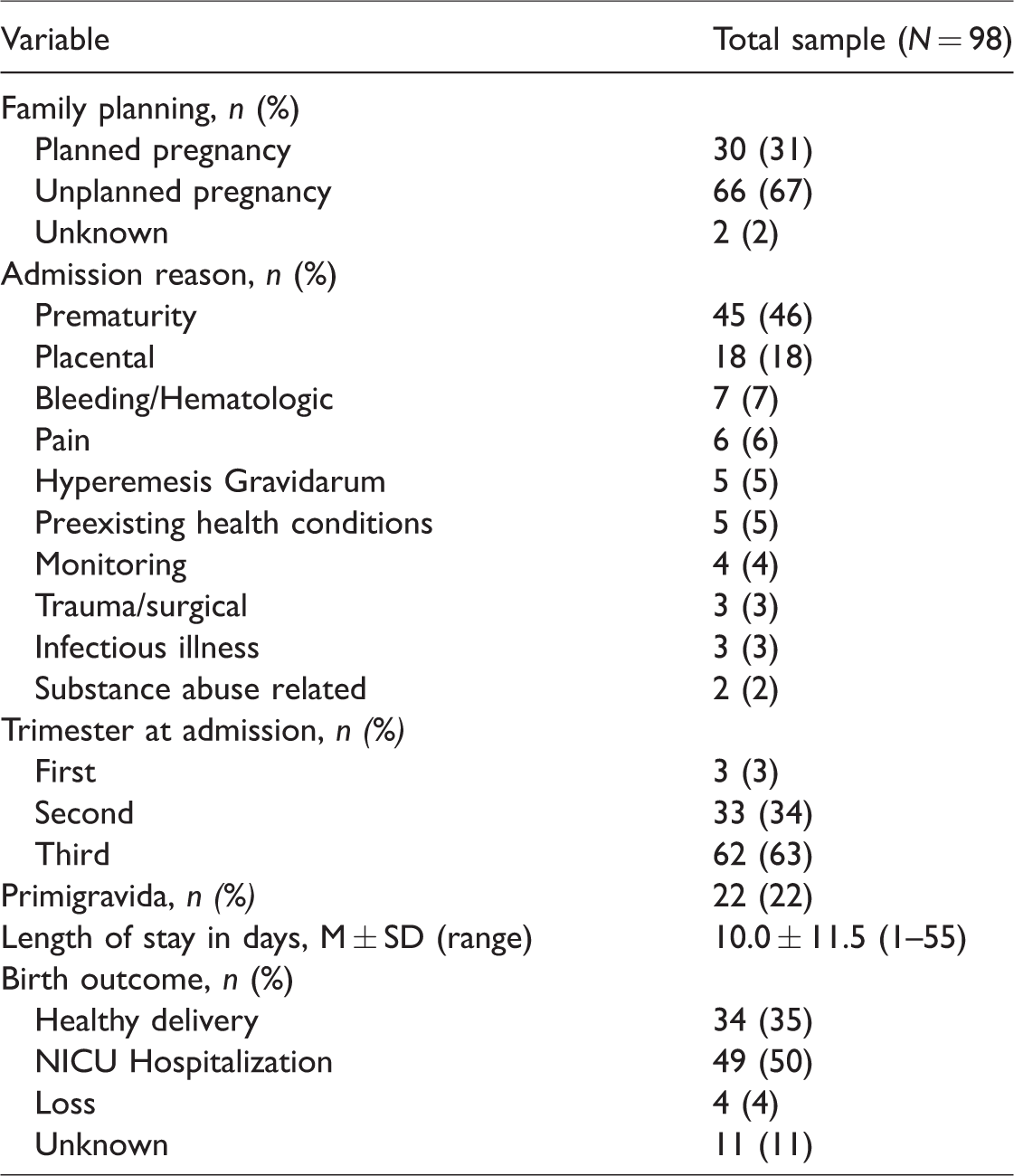
Two thirds (67%) of women reported their pregnancy as being unplanned (Table 3). The mean length of stay was 10 days. The most common reason for admission onto the antepartum floor was prematurity related (46%), followed by the placental category (18%) encompassing abruptions, previa, and pregnancy related hypertension. Less than one quarter of the women were primigravidas, and the majority were in their third trimester at the time of admission. Half of the infants (50%) delivered to participants were admitted to the neonatal intensive care unit post-delivery.
Pregnancy and medical history.
Over one third of the sample (36%) presented with an EPDS score
Screening outcomes.
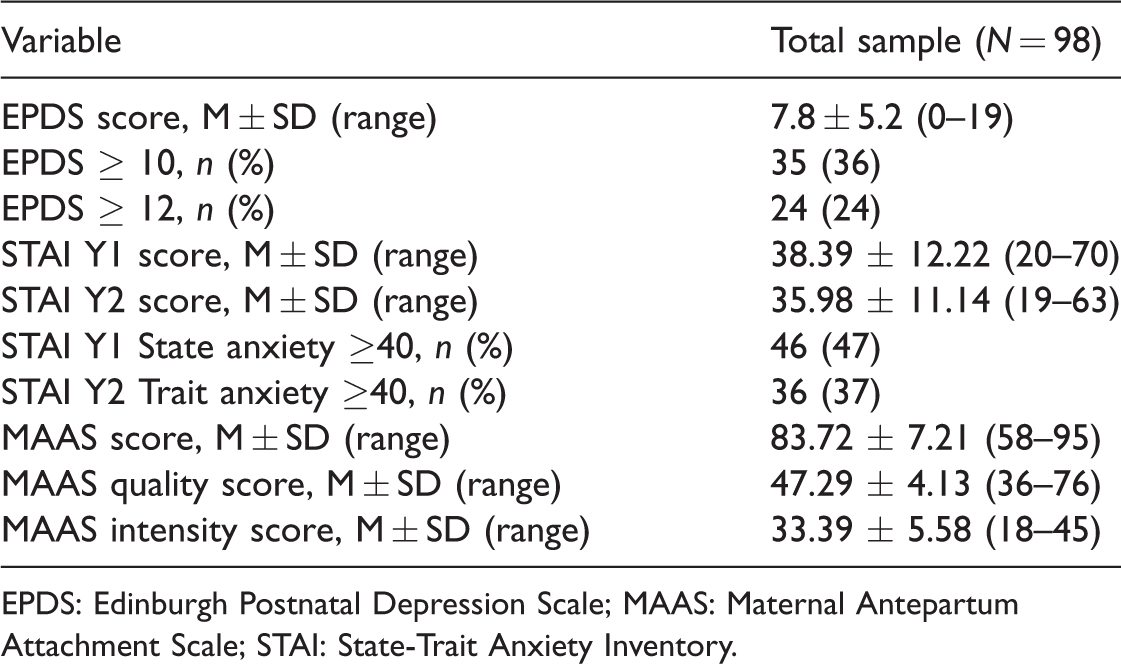
EPDS: Edinburgh Postnatal Depression Scale; MAAS: Maternal Antepartum Attachment Scale; STAI: State-Trait Anxiety Inventory.
Screening positive for depression at both cut-off points was significantly related to screening positive for state and trait anxiety. (p < 0.001 for each). As well, those who screened positive for state anxiety were significantly more likely to screen positive for trait anxiety (p < 0.001). The majority (89%) of those with EPDS
Pearson correlation coefficient calculation found that there was a positive correlation between the EPDS score and the STAI Y1 and STAI Y2 scores (r = 0.753, p < 0.001; r = 0.737, p < 0.001, respectively), meaning that participants with elevated depression risk were also more likely to have elevated anxiety. There was similarly a positive correlation between the two types of anxiety, STAI Y1 and Y2 scores (r = 0.820, p < 0.001). A weak negative correlation was found between the EPDS and MAAS Q scores (r = −0.315, p = 0.002). Similarly weak negative correlations were found between the STAI Y1/Y2 and the MAAS Q scores (r = −0.301, p = 0.003; r = −0.313, p = 0.002) and between the STAI Y1/Y2 and the overall MAAS score (r = −0.211, p = 0.044; r = −0.238, p = 0.025, respectively). This indicated that lower quality of attachment scores was related to higher levels of depression scores and both state and trait anxiety for participants.
Significant relationships were found between screening scores and certain participant characteristics. EPDS scores
Logistic regression analysis for state anxiety as the dependent variable (STAI Y1
Discussion
Of the 98 participants, over one third (36%) screened at risk for depression on the EPDS with a score
The prevalence of women who screened at risk for depression in this study (36% for EPDS ≥10 and 24% with EPDS ≥12) was well above the established prevalence estimates of antepartum depression in the general population (7% to 13%). This finding is consistent with previous research. In one recent study, 44.2% of hospitalized pregnant women scored ≥11 on the EPDS [19]. In another study, 27% of women on an antepartum unit scored ≥10 on the EPDS [18]. While there is some variability in rates and cut-off scores used, these data illustrate that women admitted for obstetrical risk are at increased risk for depression.
Elevated anxiety symptoms were commonly reported in our sample, with state anxiety (47%) more common than trait anxiety (37%). EPDS scores positively correlated with both state and trait anxiety scores, and nearly all participants with an EPDS score above threshold (95% of those ≥10 and 96% of those ≥12) also reported elevated anxiety. This finding adds to the existing literature by illustrating the very high comorbidity between depression and anxiety in women hospitalized for obstetrical risk. Notably, both state and trait anxiety did show a negative correlation with overall maternal antepartum attachment. This finding adds to the existing literature illustrating the risks of untreated perinatal anxiety disorders and the necessity of screening for anxiety disorders in obstetrics settings.
Of concern, only 15% of women who either screened positive for depression or endorsed significant anxiety were referred for mental health treatment at the time of their research visit. This finding is consistent with another recent study which found that while 27% and 13% of women on an antepartum unit screened at risk for depression and anxiety, only 5% received mental health treatment during pregnancy. 18 Together, these illustrate that as in the outpatient setting, inpatient obstetricians are unlikely to recognize symptoms of depression or anxiety without a structured screening protocol in place. Pregnant women face multiple potential barriers to self-reporting mental health symptoms including stigma, lack of awareness, lack of time, and childcare concerns.24,25 Furthermore, obstetrical inpatient providers are likely to experience the same provider-level barriers to mental health inquiries as have been reported in primary care settings such as lack of time, discomfort with mental health, and perceived lack of referral resources. 26 Various self-report scales, such as the EPDS and the Generalized Anxiety Disorder Scale, are readily available and can be completed by a patient in her hospital room in approximately 5 to 10 minutes. Although screening would be an important step in detecting depression and anxiety in women hospitalized on antepartum obstetrical units, it is also important to note that detection alone is not the goal. A screening protocol should be accompanied by referral processes for women who are identified.
This study has several strengths, including broad inclusion criteria and the differentiation between state and trait anxiety in the setting of acute inpatient care. The sample size of 98 is similar to or greater than comparable studies. The aforementioned Byatt et al.’s study 18 had a sample size of 62 and the Brandon et al.’s study 19 had a sample size of 129. Limitations should also be kept in mind while interpreting these results. Of the 166 women who were approached for study recruitment, 98 were enrolled and completed the study packet. Hypothetically, this sample may represent a distinct subgroup when compared to the larger group. Although mental health symptoms were detected with a screening measure and psychological inventory, resources did not allow for investigators to follow-up these measures with a diagnostic evaluation. Although the sample size was comparable to other studies on the mental health of high-risk obstetrics patients, it did not allow for certain higher level statistical analysis, such as odds ratio. Finally, as 2 of 10 questions on the EPDS are about anxiety, it is possible that utilization of the EPDS as a screening tool for depression may have influenced the high rate of comorbidity between depression and anxiety in this study.
Conclusions
Although peripartum depression and anxiety are common in the general obstetrics population, women hospitalized on obstetrical units are at elevated risk. Depression and anxiety are even more highly comorbid in this population and their presence correlates with disrupted antepartum attachment. As depression is a treatable illness with potential negative consequences, identification of depression in women already at increased risk for adverse obstetrical or developmental outcomes is an important consideration for care. Universal screening for both depression and anxiety is recommended on obstetrical inpatient units and should be paired with a clear referral protocol in order to link identified women to treatment.
Footnotes
Acknowledgments
The authors would like to acknowledge the Department of Obstetrics and Gynecology and particularly theUniversity Hospitals MacDonald Women's Hospital nursing staff for their help with this study.
declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.