
Abstract
Objective
Bullying is a common problem among children and adolescents. Previous studies have investigated the associations between involvement in bullying and various psychosocial and mental health outcomes thoroughly. However, only few studies have focused on the association between bullying and exposure to assaults. This study investigated whether the likelihood for severe assault exposure varies among three subgroups of bullying behavior: bullies/bully-victims, victims of bullying, and those not involved in bullying.
Method
The study population consisted of 508 adolescents (208 boys, 300 girls) aged between 13 and 17 years (mean age 15.5 years), admitted for psychiatric inpatient treatment between the years 2001–2006. Adolescents were interviewed at index hospitalization using semi-structured interview, K-SADS-PL, to assess DSM-IV based adolescent psychiatric disorders, and to obtain information on bullying behavior. Treatment episodes for assault incidents were obtained from the Finnish National Care Register for Health Care covering the entire-life of the study participants up to end of year 2016.
Results
14.4% (n = 73) of the study participants had experienced severe physical or sexual assault leading to hospital treatment during their lifetime. Results of Cox regression analysis showed that girl bullies/bully-victims had nearly threefold increased likelihood for later assault exposure.
Conclusions
Since bullying behavior in childhood and adolescence is a significant predictor for later exposure to severe assault in girls, it should be paid attention to and intervened as early as possible. Moreover, psychosocial risk factors should be taken into account considering those in hospital treatment for severe assault exposure.
Introduction
Bullying is defined as repeating aggressive behavior or intentional harm-doing by peers, and it involves an imbalance of power between the victim and the perpetrator.1,2 It can be divided into direct and indirect/relational bullying: direct bullying includes physical and verbal acts of aggression, such as hitting or name calling, whereas indirect bullying is characterized by social exclusion and rumor spreading.3,4
Bullying is a common problem among children and adolescents. According to a recent review by Moore et al., 5 the estimated prevalence of recurrent bullying victimization among adolescents ranges from 10% to 35%. In a sample of 2464 Norwegian adolescents aged 12 to 15 years, 10% reported being frequently bullied and 5% reported having been aggressive towards others during the last 6 months. 6 Similar results were obtained in a prospective study by Copeland et al. 7 From 1420 American adolescents, 26% reported being bullied at least once, and bullying others was reported by 10% of which half were bully-victims (i.e. participants who are at the same time bullies and victims). Further, bullying behavior was observed to be more common among victims of bullying (OR 2.9) compared to non-victims.
The effects of bullying have been studied extensively, and it is well established in previous studies that bullying is associated with wide range of long-lasting adverse health and psychosocial problems among both victims and bullies.5,8,9 According to the review by Moore et al., 5 exposure to bullying victimization in children and adolescents is causally associated with several adverse health outcomes, such as depression, anxiety, nonsuicidal self-injury and suicidality. However, evidence for the causal association between bullying victimization and substance use was controversial. Moreover, review and meta-analysis by Ttofi et al. 10 also shows that school bullying victimization is a major childhood risk factor for later depression even after controlling for major childhood risk factors.
Bullying victimization has also been shown to relate to different forms of maladjustment, such as low global and social self-esteem, and feelings of loneliness and dysphoria in a meta-analytic review by Hawker and Boulton. 9 According to a recent study by Antila et al., 11 bullying victimization in adolescence increased the risk for later personality disorder in females almost fourfold compared to adolescents not involved in bullying behaviour. In addition, Copeland et al. 7 reported that both victims and bully-victims had elevated rates of psychiatric disorders (e.g. anxiety, agoraphobia and panic disorder) in both childhood and young adulthood. It was also stated that the direct and long-lasting effects of being bullied were worst for the bully-victims.
Furthermore, bullying behavior has been shown to relate to externalizing disorders at adolescence. 12 After adjusting for family type, age and repeated grades at school, results showed that having an externalizing disorder (conduct disorder or substance-related disorder) increased the likelihood of being a bully or bully-victim among both the boys (OR 14) and the girls (OR 10). In addition to adolescent externalizing disorders, bullying behavior was also reported to increase the risk for antisocial personality disorder (OR 4.1) by Copeland et al., 7 which was observed by Sourander et al., 13 as well. Similarly, bullying perpetration in childhood or adolescence has been shown to strongly predict antisocial behavior, such as violence, aggressiveness, impulsivity and illegal drug use, later in life.14,15
Finally, involvement in bullying at school has been observed to be a significant predictor of violence later in life in another review by Ttofi et al. 16 After adjusting for covariates, bullying perpetration at school increased the risk of later aggression (e.g. fighting) and violence (e.g. criminal violence and violent offending) during following average of six years later in life (OR 2.0). For bullying victimization, the risk was markedly lower (OR 1.4) but still significant. Similarly, involvement in bullying has been shown to relate to several violence-related behaviors, such as weapon carrying and fighting-related injuries. 17
Previous studies have investigated the associations between involvement in bullying and various psychosocial and mental health outcomes thoroughly. However, only few studies have focused on the association between bullying and exposure to assaults, and in those studies, involvement in bullying and exposure to violence have occurred without any defined temporal aspect.18,19 Yet, exposure to assault causes severe and long-lasting problems to the victim, especially to those involved in bullying behavior already struggling with the related psychosocial difficulties. Since it is well known that bullying has a significant effect on adolescents’ mental well-being and other challenging outcomes, more information is needed on the risk factors that could be intervened preventively. Identifying and understanding these factors would allow designing target-group oriented instruments for preventing these detrimental long-term outcomes.
The aim of this study was to investigate, whether the likelihood for severe assault exposure varies between three subgroups of bullying behavior (i.e. bullies/bully-victims, victims of bullying, and those not involved in bullying). For this purpose, we had access to a large population-based data of former adolescent psychiatric inpatients from Northern Finland.
Method
Original study population
This study forms part of a clinical follow-up project, which investigates the associations between diverse psychosocial risk factors and severe psychiatric or substance use disorders. The study population consists of 508 adolescents (208 males, 40.9%; 300 females, 59.1%) who were admitted to psychiatric inpatient treatment at the Psychiatric Department of Oulu University Hospital in Finland due to acute psychiatric and substance use disorders between 1 April 2001 and 31 March 2006 (index hospitalization). Patients were 13–17 years old adolescents (mean age 15.5 years, SD 1.3) of which 98.3% were Caucasian. The catchment area of these hospitalizations includes regions of Oulu and Lapland covering 43% of Finland’s geographical area.
Participants with over 18 years of age (n = 1), with an organic brain disorder (n = 3), with an intellectual disability (n = 26), with an inpatient time too short to complete the necessary interviews (n = 22), or who did not give or whose guardian did not give a written informed consent to participate (n = 77) were not included in the study population. Of all eligible adolescents 83.7% participated to the study. The study protocol was approved by the Ethics Committee of Oulu University Hospital, Finland. Signed informed consent was obtained from both the adolescent and at least one parent (or guardian) before enrollment in the study.
Research instruments
The participants were interviewed by using the Schedule for Affective Disorder and Schizophrenia for School-Age Children - Present and Lifetime (K-SADS-PL) during hospitalization to assess DSM-IV psychiatric diagnoses. K-SADS-PL is a semi-structured interview that has shown high reliability and validity in obtaining DSM-IV diagnoses among adolescents.20–22 If data were missing or remained unreliable after interviewing the adolescent, the interview was complemented by interviewing the parents. The information of participants’ family type prior to hospitalization was also obtained from K-SADS-PL. Family type was categorized into four groups: (1) living with both biological parents; (2) single biological parent or shared custody; (3) child welfare placement and (4) other, including foster family, residential care or living alone.
Adolescents were also interviewed by using European Addiction Severity Index (EuropASI), which is a multidimensional instrument for assessing drug and alcohol dependence, with adequate reliability and validity. 23 It provided information about each participant’s school-related factors, such as use of special services or repeating a year at school, as well as their parents’ and siblings’ psychiatric problems and substance abuse. The K-SADS-PL interviews were conducted by the treating physician or by trained medical students under the surveillance of the treating physician, and the EuropASI interviews by trained nurses.
Assaulted study participants
The data regarding study participants’ lifetime hospital inpatient treatments, and outpatient treatments at specialized level since year 1998, were obtained from the National Care Register for Health Care (CRHC) provided by the Finnish National Institute for Health Welfare (THL). 24 It covers all mental and general hospitals, wards of local healthcare centers, military wards, prison hospitals and private hospitals. For this study, the register-based information for all study participants was available until the end of year 2016. However, the register does not cover the primary care outpatient visits or private sector receptions.
Assault cases were collected from the CRHC using ICD-10 classification codes R45.6, T74, X85-Y09, Y87.1, Z04.4–5 and Z61.4–6. They include all various types of physical and sexual assaults and incidents associated with them. With this selection criteria we considered that all the assault cases used in this study were definite. A total of 272 treatment episodes for assault were found until the end of year 2016. Nine of these episodes included two different diagnostic codes each, making the total number of diagnostic codes 281. From the original population of 508 adolescents, 73 had been assaulted (44 boys, 29 girls), of which 58 were physical (40 boys, 18 girls), and 15 were sexual assaults (4 boys, 11 girls). Two girls had been assaulted both physically and sexually, and they were counted as physical assault incidents.
Bullying behavior
Information on bullying behavior was obtained from two sections of the K-SADS-PL. In the non-structured part (School Adaptation and Social Relations) participants were asked whether they had been bullied or not, while data on the bullying of others were obtained from the conduct disorder criteria, where the adolescents were asked: “Has there ever been a time when any kids really got on your nerves? Did you sometimes do things to get back at them? Like what? Call them names? Threaten to beat them up? Push them? Trip them? Knock their books out of their hands? Come up from behind and slap them in the face? How often did you do these things?” Bullying was defined as present if an adolescent had threatened or intimidated another on three or more occasions.
The participants were categorized accordingly into the following four mutually exclusive subgroups of bullying behavior: (1) victims, n = 176, 34.6% (115 females, 38.3%; 61 males, 29.3%), (2) bullies, n = 72, 14.2% (30 females, 10.0%; 42 males, 20.2%), (3) bully-victims (i.e. those who were both bullies and victims), n = 28, 5.5% (14 females, 4.7%; 14 males, 6.7%) and (4) no bullying behavior (i.e. adolescents not involved in bullying behavior), n = 232, 45.7% (141 females, 47.0%; 91 males, 43.8%). In this study, subgroups (2) and (3) were compiled into one single subgroup of bullies/bully-victims.
Statistical methods
Statistical significances of group differences in categorical variables were analyzed using Pearson’s Chi-square or Fishers’ exact test. The association of gender and bullying status to age at first assault was examined using Cox regression analysis. All tests were two-sided and the limit for statistical significance was set at p < 0.05. All statistical tests were performed using IBM SPSS version 25.
Covariates used in Cox regression analysis included all background and clinical characteristics listed in Table 1 except for family type and conduct disorder, which were excluded due to multicollinearity.
Background and clinical characteristics of study participants according to bullying status and exposure to assault.
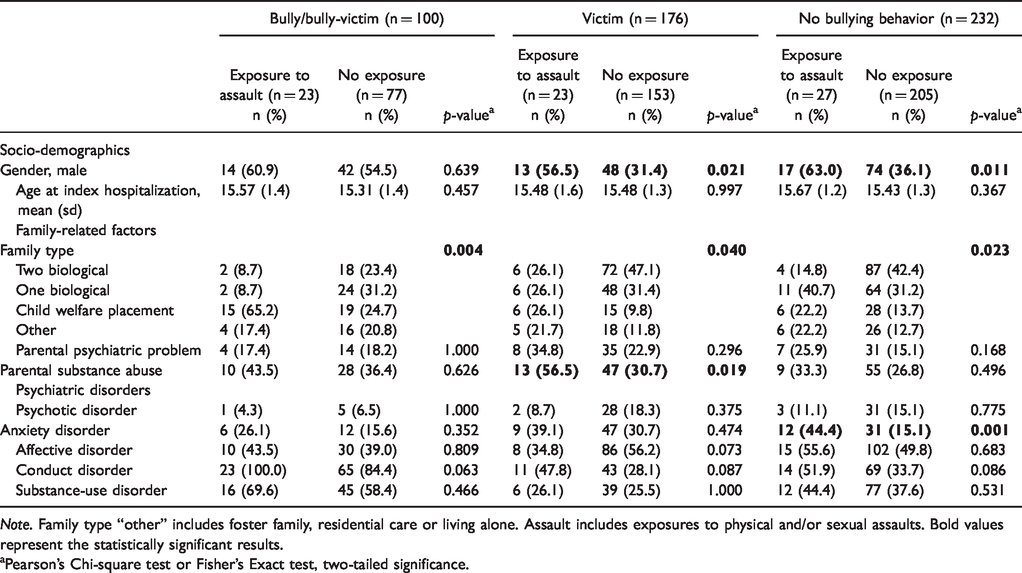
Note. Family type “other” includes foster family, residential care or living alone. Assault includes exposures to physical and/or sexual assaults. Bold values represent the statistically significant results.
aPearson’s Chi-square test or Fisher’s Exact test, two-tailed significance.
Results
Background and clinical characteristics at adolescence
The background and clinical characteristics of study participants at adolescence are presented in Table 1 according to the assault exposure and bullying status. Significantly greater proportion of assaulted study participants were males compared to those with no exposure to assault, among both victims of bullying (56.5% vs. 31.4%, p = 0.021), and those not involved in bullying behavior (63.0% vs. 36.1%, p = 0.011). Among victim group, parental substance abuse was more common among assaulted participants compared to those not assaulted (56.5% vs. 30.7%, p = 0.019). Also, participants exposed to assault were more likely to suffer from anxiety disorder (44.4% vs. 15.1%, p = 0.001) among group with no bullying behavior. Among all three groups, significantly greater proportion of assaulted participants were from child welfare placement, whereas participants with no assault exposure were more often from families with two biological parents.
Prevalence of hospital-treated assaults
As illustrated in Figure 1, exposure to assault was most common among adolescents from bully/bully-victim group, in which 25.0% of males (n = 14) and 20.5% of females (n = 9) had been assaulted. For victims of bullying, prevalences of exposure to assault were 21.3% (n = 13) for males and 8.7% (n = 10) for females, and for those not involved in bullying, 18.7% (n = 17) for males and 7.1% (n = 10) for females. Among males, there were no significant differences between the subgroups of bullying status (p = 0.661), whereas among females, assault exposure was significantly more common among bullies/bully-victims (p = 0.027).
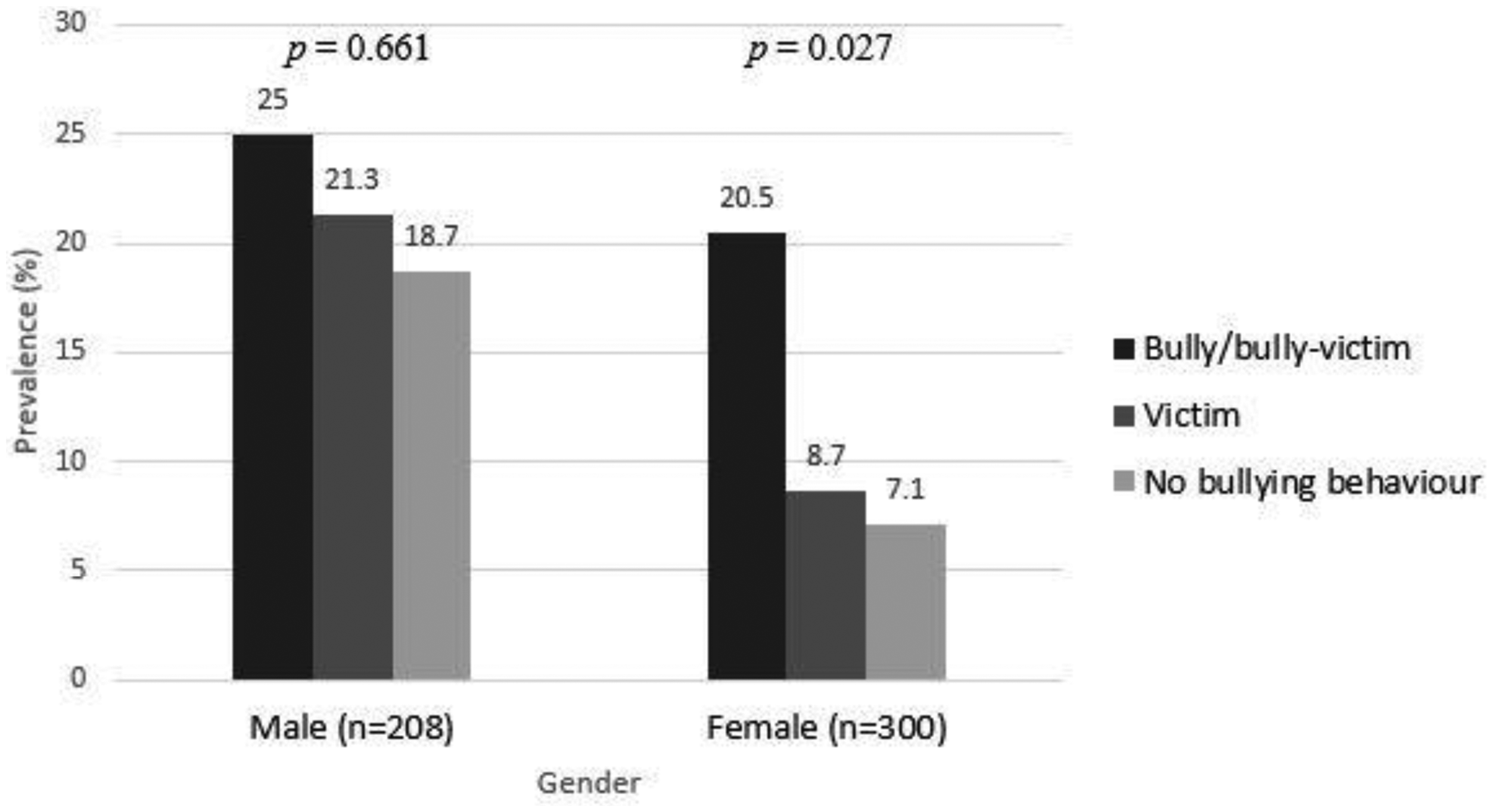
Prevalence of hospital-treated assaults (%) among study population by bullying status, according to gender.
Predictors for assault exposure
Results of Cox regression analysis are presented in Table 2. For males, the hazard ratio (HR) for hospital-treated assault was 0.94 for victims of bullying and 1.45 for bullies/bully-victims, with no significant difference compared to those not involved in bullying (p = 0.883, and p = 0.325, respectively). However, anxiety disorder in adolescence (HR = 5.32, p < 0.001) and parental psychiatric problems (HR = 2.45, p = 0.031) were significantly associated to assault exposure. Among females, belonging to the subgroup of bullies/bully-victims was associated with significantly increased hazard (HR = 2.76, p = 0.039) for assault exposure, while none of the covariates remained significant.
Adolescence-related predictors for assault exposure, by gender.
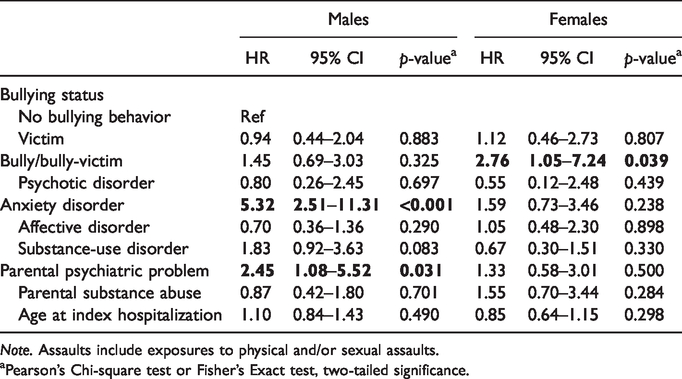
Note. Assaults include exposures to physical and/or sexual assaults.
aPearson’s Chi-square test or Fisher’s Exact test, two-tailed significance.
Cumulative incidents of assault exposure by age
Figure 2 shows the Kaplan-Meier analysis of cumulative incidents of assault exposure by age among the bullying status subgroups, for both males and females. Among assaulted males, 47% (n = 8) of those not involved in bullying behavior were assaulted before the age of 18 years, compared to 23% (n = 3) of victims of bullying and 29% (n = 4) of bullies/bully-victims. However, no significant difference between subgroups by bullying status was observed.
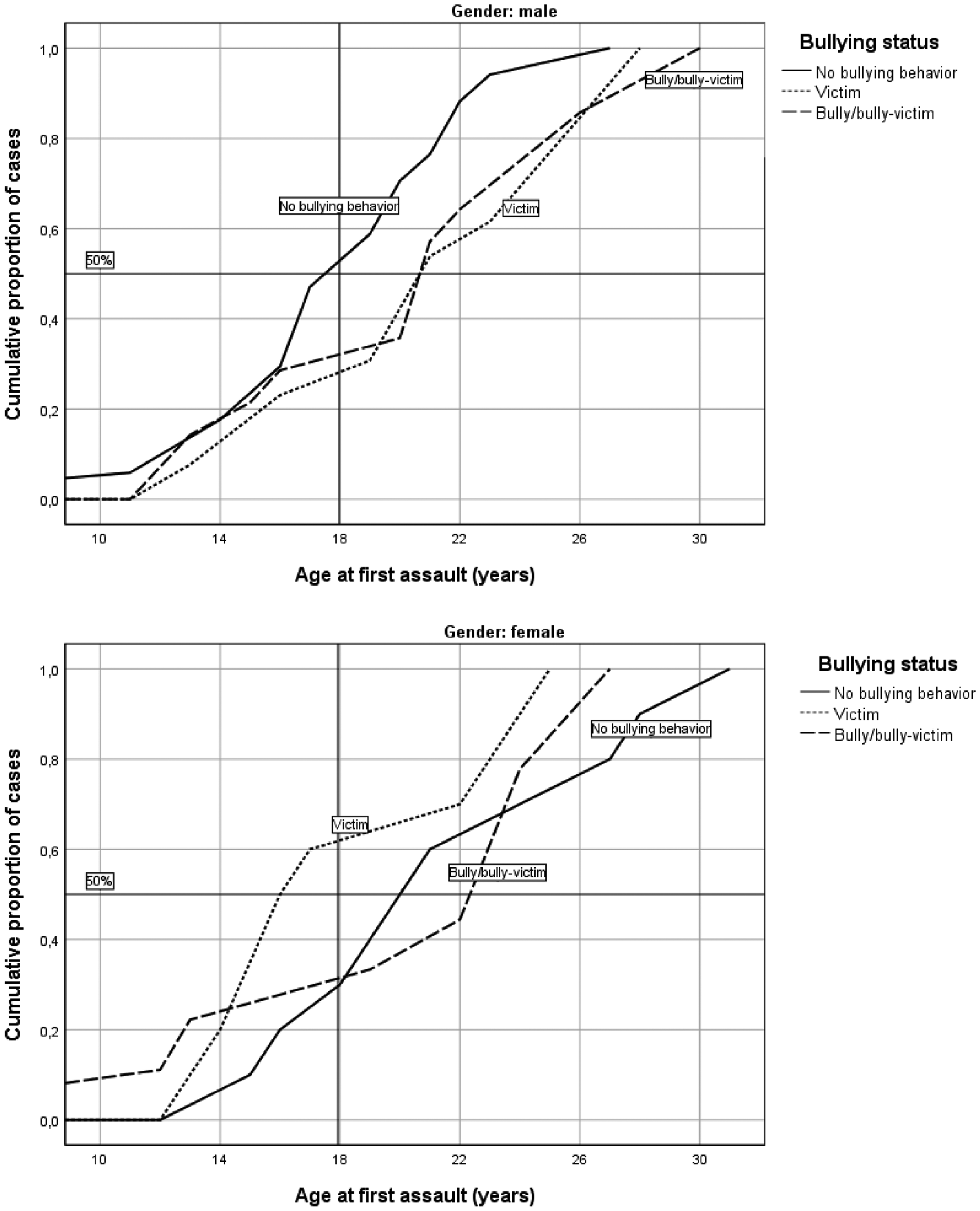
Cumulative incidents of assault exposure by age.
Among females, up to 60% (n = 6) of assault exposures among victims of bullying had occurred before the age of 18 years, compared to only 22% (n = 2) among bullies/bully-victims and 20% (n = 2) among those not involved in bullying. However, no significant difference between subgroups by bullying status was observed.
Discussion
The aim of this study was to investigate the differences in assault exposure, and the age at first assault, between three subgroups of bullying behavior (i.e. bullies/bully-victims, victims of bullying, and those not involved in bullying), among former adolescent psychiatric inpatients. The major finding was that girls who had been bullies or bully-victims in childhood and adolescence had a threefold higher likelihood for hospital-treated assault exposure up to adulthood, compared to those not involved in bullying behavior. To the best our knowledge, no previous studies have investigated the association between bullying behavior and later severe assault exposure leading to hospital treatment in young adulthood. However, involvement in bullying behavior has been shown to associate with several psychosocial and mental health outcomes that have further been shown to increase the risk for assault exposure. These outcomes, as discussed later, could be a possible link in explaining the bullying-associated risk for hospital-treated assault exposure in our clinical sample of psychiatric inpatients. The results of current study also showed that in males, anxiety disorder at adolescence, but not other psychiatric disorders, was associated with five times higher likelihood for assault exposure up to young adulthood, and this association did not depend on the type of bullying behavior. Also, in previous studies, anxiety symptoms have been found to associate with physical victimization in young adults, 25 and with risk for peer-victimization among adolescents. 26
The association between externalizing disorders and bullying behavior was examined in an earlier study, using the same database as the current study. 12 Results of logistic regression analyses showed that girls with externalizing disorder (i.e. conduct disorder or substance-related disorder) had a 10-fold increased likelihood of being a bully or bully-victim. Haller and Chassin 27 reported that females with externalizing symptoms during adolescence were significantly more likely to be exposed to assaultive violence (OR = 2.4). They also discussed that this association suggests that impulsive and risky behavior may place females at risk for being exposed to assaultive violence.
Furthermore, bullying behavior has been shown to associate with antisocial personality disorder (ASPD)7,13 and antisocial behavior (e.g. violence, aggressiveness, impulsivity and illegal drug use).14,15 Beaver et al. 28 investigated the association of psychopathic personality traits to victimization and exposure to violence by using Levenson Self-Report Psychopathy (LSRP) scale to measure psychopathic personality traits. Their results revealed a positive and statistically significant association between LSPR scores and the likelihood for being victimized. They also attempted to uncover some of the mediating mechanisms possibly accounting to the link between psychopathy and victimization, and the only significant mediating measure was the delinquent peers scale, which suggests that belonging to antisocial peer networks increases the risk of being victimized. Moreover, Gobin et al. 29 supposed that certain features of ASPD (e.g. sensation seeking, behavioral difficulties) could be possible factors in increasing the vulnerability to crime-related trauma exposure. Also, previous violence (e.g. involvement in fight or injuring another person) and substance use are known to be common among youth seeking emergency department (ED) care for assault injuries. 30
Lastly, bullying has been shown to predict criminal violence and violent offending later in life, 16 as well as weapon carrying and fighting related injuries. 17 A recent study by Carter et al. 31 investigated arrests among young adults seeking ED care treatment for either assault or non-violence reasons. According to results, youth with assault-related injuries were 47% more likely to be arrested during next 24 months after receiving treatment at ED compared to youth with injuries not related to violence. Further, a comprehensive study by Smith and Ecob 32 analyzed the causal links between victimization and offending in a cohort of 4300 adolescents. Their analysis confirmed a substantial correlation between victimization and offending over the same time period. In addition, they examined the relations of ten explanatory variables (e.g. impulsivity, conflict with parents, and risky spare-time activities) to both victimization and offending separately, of which seven were significantly related to both victimization and offending. These findings support the roles of lifestyle-routine activities, weak social bonds and a risk-taking or impulsive personality, but not the role of neighborhood-related characteristics, in explaining the association between victimization and offending.
Concerning the prevention of bullying among children and adolescents, KiVa is a Finnish evidence-based antibullying program for schools, implemented widely in schools throughout the country, but also being evaluated internationally. 33 It has been shown to significantly decrease both self- and peer-reported bullying and victimization in a large randomized controlled trial, 34 and also to reduce anxiety and depression. 35 Another applicable approach to intervene bullying and to prevent its unfavorable consequences is the Collective Impact (CI) approach, which in Finland includes the “Let's Talk about Children Service Model (LT-SM)”. It is a community-based service approach which aims to impact the need for support among children and adolescents by connecting relevant stakeholders, including healthcare and school health services, with families and their social networks to recognize and organize the support needed. 36
There are some limitations in this study. Firstly, the information on assault incidents treated in outpatient settings is not comprehensive, since the Finnish Care Register for Health Care (CRHC) only covers outpatient treatment in specialized level health care settings since year 1998. However, information on hospital discharges cover all inpatient care, whether they occurred in health centers, hospitals or other institutions providing inpatient care throughout the whole of Finland. Therefore, assault incidents of this study represent those severe enough to require inpatient care or assessment in specialized level outpatient clinics, thus the prevalence of hospital-treated assault incidents available for this study is an underestimate of all assault exposure cases. Secondly, the study population consisted of psychiatric inpatients and, therefore, the conclusions concerning the general population must be made with caution.
Thirdly, assaults that occurred prior to index hospitalization were included in the analyses, because the development of many psychiatric disorders begins during childhood but may not manifest until adolescence or adulthood. However, of all the assaults recorded in the study, the proportion of pre-index assaults was very small. We assume that this did not have an influence on our results and related conclusions, but it warrants consideration with respect to causality of the phenomena investigated in our study. Also, the role of adverse childhood experiences (e.g. abuse or maltreatment in childhood or witnessing family violence) was not investigated in this study. Moreover, the variable for bullying behavior was based solely on the questions concerning bullying behavior in the K-SADS-PL interview. The K-SADS-PL, however, did not contain any qualitative data on the bullying behavior (e.g. the type of bullying or its severity). Also, in our study the proportion of bully-victims accounted for only 5.5% of total study population, and therefore, it was not statistically feasible to study bully-victims as own group. Bully-victims were combined with bullies according to earlier finding that the overlap of bully-victims with victims of bullying is smaller than with bullies. 37 In future studies, however, bully-victims should be examined as a distinct subgroup in larger data settings. Lastly, the grade of severity of assault exposures was not examined. Further studies are therefore needed to investigate, whether the severity of assault exposures gradually develops, and whether the development eventually leads to fatal incidents of assault exposure.
The strength of this study is that, by including assault cases based on the information of the CRHC using ICD-10 diagnostic coding system, the observed assault cases are definitely concrete cases, which provides us a certain kind of authenticity compared to case definitions based on self-reports by study participants. 24 Further, our definition of adolescent psychiatric disorders is comprehensive and reliable because they were assessed using the K-SADS-PL interview, showing high psychometric properties for defining psychiatric disorders in adolescent populations.20–22
In conclusion, over half of the study participants with a history of hospital-treated psychiatric disorders at adolescence were involved in bullying behavior, thus the focus of our study is relevant. As our study showed, bullying behavior in childhood and adolescence is a significant predictor for later exposure to severe assault in girls, thus it should be paid attention to and intervened as early as possible. Moreover, psychosocial factors should be evaluated among those admitting to hospital due to severe assault exposure. Intervention programs and approaches may give tools to intervene in bullying and to reduce bullying-related psychosocial adversities,34,36 and we hope to see utilization of such methods to become more common in real practice in near future.
Footnotes
Ethical Approval and Informed Consent
The study protocol was approved by the Ethics Committee of Oulu University Hospital, Finland. Signed informed consent was obtained from both the adolescent and at least one parent (or guardian) before enrollment in the study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Päivikki and Sakari Sohlberg Foundation, Helsinki, Finland; the Iso-Mällinen Foundation, Tyrnävä, Finland; the Kerttu Saalasti Foundation, Nivala, Finland; and the Alma and K.A. Snellman Foundation, Oulu, Finland.