
Abstract
Risk factors for attention deficit hyperactivity disorder (ADHD), psychiatric, and classroom academic/behavioral problems were examined in 929 students grades 1–6 in Jeddah, Saudi Arabia. Teachers identified ADHD by completing the Vanderbilt ADHD scale. Compared to controls without ADHD, students with ADHD were more likely to have early parental loss, head trauma, motor/language delay, family psychiatric problems, and high family stress. Among those with ADHD, risk factors for psychiatric comorbidity were older age, family psychiatric history, and motor/language delay. Risk factors for impaired academic/behavioral performance were high family stress, family psychiatric problems, and chronic illness. Identifying risk factors for ADHD and common comorbidities associated with this disorder may help parents, teachers and clinicians detect this condition, increasing effective management.
Keywords
Introduction
Attention deficit hyperactivity disorder (ADHD) is one of the most common neurobehavioral conditions in children, with a worldwide prevalence of 5–8%. 1 Children with ADHD have fewer friends, are more likely to drop out of school, engage in antisocial activities, and have higher rates of comorbid psychiatric disorder, emergency room visits, acute hospitalizations, and higher total medical costs compared to those without ADHD. 2
Few studies have systematically examined risk factors for ADHD among community-dwelling primary school children in the Kingdom of Saudi Arabia (KSA). This is particularly true when children being seen in psychiatric settings are excluded. An extensive review of the literature uncovered only five published studies on ADHD in primary school students in KSA.3–7 Prevalence rates ranged from 2.7% to 16.4%, averaging about 9%, with male gender and younger age being the most consistent risk factors. Only two studies examined an extensive array of risk factors.7,8 Likewise, only one examined psychiatric comorbidity, impaired academic performance, and classroom behavioral problems. 8 While teachers in Saudi Arabia are aware of ADHD, their knowledge about the disorder and its treatment is limited. Likewise, under diagnosis and under treatment of ADHD by clinicians in KSA is known to be a problem, partly due to families' reluctance to seek treatment from ADHD specialists for fear of labeling and stigma. 8
Given the relatively high prevalence of ADHD in this part of the world, under recognition, and under treatment, we examined demographic, family, and medical risk factors for ADHD among students in public primary schools in Jeddah.
Methods
A random sample of six public primary schools (three all female, three all male) was identified, followed by a random sample of 6 classes from each of grades 1–6 (class sizes ranging from 25 to 35). There is no reason to suspect that the randomly selected 6 classes from each of grades 1 through 6 at each school were different from the general population of schools selected (i.e., they were not specifically chosen because they contained students with academic or behavioral problems). Between April and December of 2016, medical interns and 6th year medical students approached the primary teacher in each class and asked him/her to complete a questionnaire on each student. All 36 teachers approached agreed to participate and gave written informed consent, although no written consent was obtained from parents since the study had been approved by the Saudi Ministry of Education. In order to identify risk factors, mothers of students with ADHD (n = 46) were asked to complete a questionnaire, all of whom agreed to participate and gave written informed consent. The same number of mothers of students without ADHD (n = 46) were asked to complete the questionnaire. These were a consecutive series of mothers of students who scored below the ADHD diagnostic threshold; controls were not selected by teachers nor did they volunteer prior to being approached. Of the control mothers approached, 39 (85%) agreed to participate, gave written informed consent, and completed the questionnaire. The study was approved by the King Abdulaziz University Institutional Review Board after permission was obtained from the Saudi Ministry of Education.
Questionnaire
The Vanderbilt ADHD Diagnostic Teacher Rating Scale (VADTRS) was completed by teachers to identify students with ADHD. 9 This screening measure has excellent construct and convergent validity and acceptable scale reliabilities in community samples of children, and is one of the most common tools in the world to identify ADHD. 10 The VADTRS directly follows DSM-IV-TR criteria, takes about 10 minutes to complete, and an Arabic version of the scale exists. 8 The VADTRS identifies students who meet criteria for ADHD. In addition, this measure determines any psychiatric comorbidity or classroom academic/behavioral comorbidity that may accompany ADHD. Of the 43 questions, 18 items are used to identify ADHD and subtypes (hyperactive, inattentive, and combined types), 17 items to assess psychiatric comorbidity, and eight items to assess impaired classroom academics and behavior. Overall rates of ADHD were arrived at by summing inattentive, hyperactive, and combined types.
Psychiatric comorbidity on the Vanderbilt scale is assessed by items 19–35; items 19–28 assess oppositional defiant disorder/conduct disorder (ODD/CD); and items 29–35 measure anxiety/depression. Impaired academic performance is determined if the child is rated problematic on one or more of three academic performance items (reading, mathematics, written expression), and impaired behavioral performance is determined by one or more problem areas involving relationships with peers, following directions/rules, disrupting class, assignment completion, or organizational skills.
Risk factors
Students’ mothers were asked questions about demographic, family, and medical characteristics.
Demographic
Assessed where the student's age, grade, gender, order of birth, number of siblings, and monthly family income (<5000 SR, 5000–8000 SR, >8000 SR).
Family factors
Presence (1) or absence (0) of family history of psychiatric illness, early parental loss, and family stress was determined.
Medical factors
Mothers were asked about the presence of any complications during pregnancy, labor or delivery, or the neonatal period. They were also asked if the student had experienced any chronic childhood illnesses and if there was a history of childhood head trauma. Finally, the presence motor or language delay was also determined.
Risk factors vs. comorbid conditions
The risk factors for ADHD and for the comorbid psychiatric conditions/classroom problems that may occur in those with ADHD should be distinguished. 11 Risk factors include characteristics that make it more likely for a child to develop ADHD, whereas comorbid conditions may or may not occur in children with ADHD.
Statistical analyses
Cases and controls were compared using chi-square test for categorical and the Student's t-test for continuous variables. Stepwise logistic regression was used to identify independent risk factors for ADHD. Model 1 included demographic factors only; Model 2 included any demographics significant at p < 0.15 from Model 1 plus the addition of family factors; and Model 3 included any demographic or family factors from Model 1 and 2 significant at p < 0.15 plus medical factors. The final model included only variables significant at p < 0.10 in previous models. The same procedure was followed when constructing multivariate logistic models predicting risk factors for comorbid psychiatric problems and classroom problems. All statistical analyses were performed using SAS (version 9.4; SAS Institute Inc., Cary, NC).
Results
Teachers completed the VADTRS on 89% of male and 80% of female students, screening a total of 929 students. Of the 929, 46 students met criteria for ADHD (cases). The mothers of 39 students without ADHD were also interviewed to assess risk factors (controls).
Risk factors for ADHD
The average age of those with ADHD was 8.8 years (SD = 1.8), similar to that of controls (9.2 years, SD = 1.5) (Table 1). Average grade level in both groups was 3rd. Gender distribution, number of firstborn children, and siblings was similar in both groups. Cases were more likely to have experienced early parental loss (31.0% vs. 7.7%, p = 0.009), to have a family psychiatric history (28.6% vs. 0.0%, p = 0.0003), and especially, be in families experiencing high stress (57.1% vs. 7.7%, p < 0.0001). There were no significant differences between cases and controls on pregnancy, labor, or neonatal complications. Childhood head trauma was more common in cases by five-fold (28.6% vs. 5.1%, p = 0.005), as was motor/language delay (42.9% vs. 7.7%, p = 0.0003).
Comparison of risk factors between students with ADHD and controls.
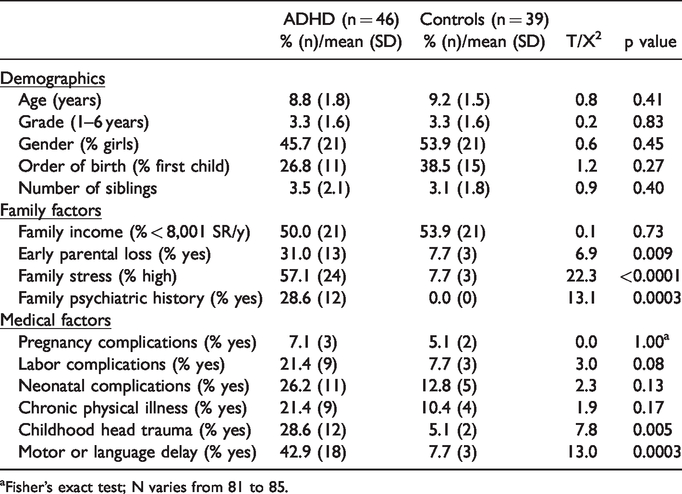
aFisher’s exact test; N varies from 81 to 85.
In multivariate analyses, no demographic factor was associated with ADHD. Among family factors, only high family stress was associated with risk (B = 2.94, SE= 0.75, p < 0.0001). Among medical factors, after including high family stress in the model, only the presence of motor/language delay was a significant predictor (B = 2.17, SE = 0.86, p = 0.01). Cases with high family stress were nearly nine times more likely to have ADHD than controls (OR= 8.99, 95% CI= 2.00–40.41, p = 0.004). Likewise, cases with motor/language delay were also nearly nine times more likely than controls to have ADHD (OR= 8.91, 95% CI = 2.10–37.87, p = 0.003).
Risk factors for comorbid psychiatric and classroom problems
A total of 30 of 46 students with ADHD screened positive for comorbid psychiatric problems. Similarly, 32 had classroom problems (Table 2). Almost all (93.5%) had one or the other. Comorbid psychiatric problems were more common in those who were older (9.3 vs. 8.0 years, p = 0.02), male (63.3% vs. 37.5%, p = 0.09), had a family history of psychiatric problems (38.5 vs. 12.5, p = 0.07), or had motor or language delay (53.9% vs. 25.0%, p = 0.07). Classroom academic and behavioral problems were especially prevalent in students with high family stress (67.7% vs. 27.3%, p = 0.02), although interestingly, were less common among those with a family history of psychiatric problems (19.4% vs. 54.6%, p = 0.03).
Comparison of ADHD students with and without psychiatric and classroom comorbidity.
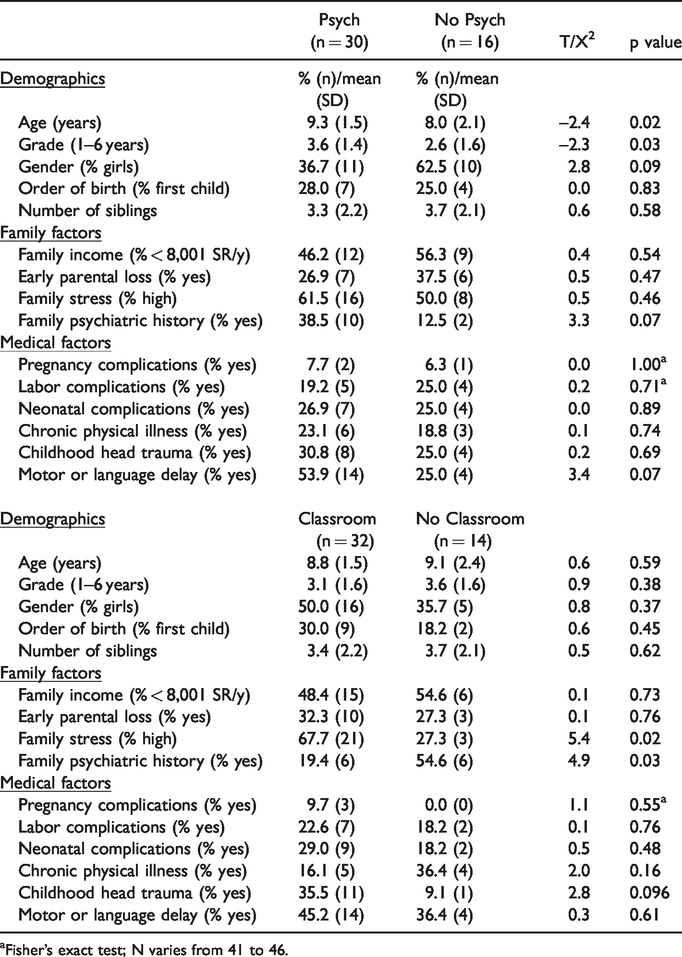
aFisher's exact test; N varies from 41 to 46.
Multivariate analyses for comorbid psychiatric problems revealed that among family factors, only family psychiatric history was significant (B = 1.96, SE = 0.96; OR = 7.1, 95% CI = 1.07–46.71, p = 0.04). Among medical factors, only motor/language delay (B = 2.38, 1.06; OR = 10.76, 95% CI = 1.35–85.93, p = 0.03) differentiated cases from controls. With both family psychiatric history and motor/language delay in the final model, family psychiatric history (B = 1.46, SE = 0.88; OR = 4.30, 95% CI = 0.76–24.18, p = 0.098) and motor/language delay (B = 1.24, SE = 0.72; OR = 3.44, 95% CI = 0.84–14.21, p = 0.09) only marginally increased the likelihood of comorbid psychiatric problems.
In multivariate analyses examining comorbid classroom problems, among family factors, only family stress was a significant positive predictor (B = 1.84, SE = 0.90; OR = 6.29, 95% CI = 1.08–36.50, p = 0.04). Among medical factors, childhood chronic illness was the only factor approaching significance and it was a negative predictor (B=-2.14, SE = 1.18; OR = 0.11, 95% CI = 0.01–1.08, p = 0.06). In the final model, family stress was the only significant predictor, increasing the likelihood of comorbid academic problems over 7-fold (OR = 7.25, 95% CI = 1.18–44.6, p = 0.03), while history of family psychiatric problems (OR = 0.23, 95% CI = 0.04–1.18, p = 0.08) and childhood chronic illness (OR = 0.19, 95% CI 0.03–1.31, p = 0.09) marginally reduced risk.
Discussion
This is one of the first studies to identify risk factors for ADHD, comorbid psychiatric and classroom problems among primary school students in Jeddah, a city of more than 3.5 million in Western Saudi Arabia. Among only a half-dozen reports on ADHD in KSA, this study provides one of the most detailed looks at risk factors, including some risk factors yet to be examined in this country.
In the only other study to examine ADHD risk factors among primary school students in Jeddah city, Homidi et al. screened 2,770 students aged 6–12 years. 4 ADHD was more common in younger children (ages 6–9) and in male students (7.4% vs. 4.2% in females), the only risk factors examined. In a 2007 study that used the Vanderbilt scales to screen 708 students ages 7–9 in the Asir province near Yemen, Alqahtani also found a higher prevalence of ADHD in boys than girls. 3 Although the effects of age and other risk factors were not described in that article, a second article from this study 8 reported that grade, social class (income), and parent education were unrelated to ADHD, similar to our findings. Alqahtani also reported a high prevalence of ODD/CD, depression, anxiety, and classroom academic and behavior problems in those with ADHD, which is consistent with the present findings. 12
In another study from southwestern KSA, Taleb and Farheen screened 200 primary school children (100 boys and 100 girls) ages 6–9+ in Jinzan. 5 No significant differences in ADHD rates were found based on gender, age, order of birth, father education, or number in family. Only having an illiterate mother increased risk. In a fourth Saudi study, Al Hamed et al. surveyed 1287 male students ages 6–13 at public and private primary schools in Dammam, eastern KSA. 7 They also found that younger students were more likely to screen positive for ADHD. The hyperactivity ADHD subtype was more common in children from single parent households, perhaps reflecting more family stress. ADHD was not associated with duration of pregnancy, type of delivery, place of delivery, or birth weight. Finally, in the last and most recent of the five Saudi studies, researchers surveyed 646 boys and girls in grades 1–3 in Riyadh, finding that ADHD was associated with low maternal education, gender (male), and younger age. 6 Like most studies above, they did not examine comorbid psychiatric problems, academic, or behavioral problems.
Although there are several differences between ours and others' findings (as well as similarities), to our knowledge this is the first study to examine family stress, motor/language delay, and childhood head trauma as ADHD risk factors in Saudi Arabia, all of which were associated with higher rates of ADHD.
Limitations
This study has several limitations that may affect the generalizability of the findings to primary school students in Jeddah. First, the number of cases identified with ADHD was relatively small, as were the number of controls to whom cases were compared, thus limiting statistical power to detect only moderate to large differences. a a Second, the 39 controls without ADHD were a consecutive sample selected from among the 877 students with subthreshold VADTRS scores (a convenience sample). Furthermore, no information on demographic characteristics or other risk factors (e.g., gender, age, grade, family stress, head trauma) was obtained on the other 838 participants with subthreshold VADTRS scores for comparison with controls, leaving open the possibility that controls may not have been representative of students without ADHD. Third, information was not collected on all primary public school students in Jeddah or on all students attending the selected schools for comparison with students screened for ADHD in the present study; thus, it is possible that participants may have differed from these larger groups. Finally, Jeddah is a relatively cosmopolitan city that is unlike more conservative regions of Saudi Arabia, which may have affected both ADHD prevalence and risk factors. Despite these limitations, the present study also has a number of strengths, including the random selection of public schools/classes, high response rate by teachers and mothers, use of the Vanderbilt ADHD teacher rating scale (one of the most common ADHD screening measures in the world 10 ) and use of multivariate statistical techniques to identify independent risk factors for ADHD and comorbid problems.
Conclusion
To our knowledge, this is one of the first studies to comprehensively examine risk factors for ADHD, psychiatric comorbidity, and classroom behavior among primary school students in Saudi Arabia. We found that high family stress was one of the strongest risk factors for ADHD. In addition, motor/language delay, early parental loss, family psychiatric history, and early childhood head trauma may also signal increased ADHD risk. Among those with ADHD, the presence of motor/language delay or a family psychiatric history may increase the risk of psychiatric comorbidity, while family stress and psychiatric history my increase risk of classroom academic and behavioral problems. The identification of risk factors for ADHD and associated comorbid psychiatric and classroom problems is necessary for its detection, management, prevention, and allocation of mental health resources in the city of Jeddah and Saudi Arabia more generally.
Footnotes
Authors’ note
All authors served in the design, conception, drafting of the manuscript, or acquisition of the data, and served in the final approval of the version being submitted.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Deanship of Scientific Research (DSR), King Abdulaziz University, Jeddah, under grant no. G-1436–248-461. The authors, therefore, acknowledge with thanks the DSR technical and financial support.