
Abstract
Background
Type 2 diabetes (T2D) is a burgeoning epidemic in children and adolescents. Adult T2D doubles the risk of depression and mental health comorbidity, makes it more difficult to make the lifestyle, medication adherence and health behavior changes needed to optimize outcomes. There is limited research on the impact of depression and depressive symptoms on youth T2D.
Methods
A search of the literature in the last 10 years regarding youth with depression and T2D was conducted. Abstracts were screened by 2 randomly assigned authors for inclusion, and disagreement was resolved by a third author. Selected full-text articles were divided among all authors for review.
Results
13 publications from 8 studies (N=2244, age 6–17) were included. 6 of 13 publications utilized Treatment Options for Type 2 Diabetes in Youth (TODAY) study data. While studies included evaluation of depressive symptoms, most did not formally assess for major depressive disorder (MDD) and excluded participants with a previous diagnosis of MDD. Depressive symptoms were common in this population and were associated with negative T2D outcomes.
Conclusions
While there is a growing body of adult literature highlighting the extensive relationship between T2D and mental health, there is a dearth of data in youth. Future studies are needed that include, 1.) youth with diagnosed MDD, 2.) treatment studies of both T2D and MDD, 3.) larger, more racially diverse samples of youth with T2D, and 4.) studies that evaluate the impact of social determinants of health, including mental health comorbidity on outcomes of T2D.
Introduction
Rates of type 2 diabetes (T2D) in children and adolescents have been increasing across the globe over the last decade. 1 Recent research demonstrated a 4–7% annual increase in T2D rates in U.S. youth.2,3 As many as 5000 new cases of T2D are diagnosed in US youth each year, with a growing chronic disease burden. 1 Youth onset T2D is a burgeoning epidemic with serious long-term complications and health burden for the youth suffering with this disease.
The diagnosis of T2D in youth produces earlier and more severe complications than when T2D is diagnosed in adulthood, as well as compared with youth with type 1 diabetes. 4 The presence and severity of diabetes complications are evident earlier in youth onset T2D than would be predicted from established risk factors, including BMI, blood pressure, glucose control, and T2D illness duration.5,6
Youth with T2D have earlier and more profound complications not predicted by identified risk factors; therefore, there is a substantial need to ascertain strategies to identify youth at risk for these outcomes earlier and intervene aggressively. 7 Mental health comorbidity represents an understudied, but frequent and modifiable risk factor in youth with chronic illness, such as T2D. Youth with chronic illness are significantly more likely to develop depression and depressive symptoms than those without chronic illness.8,9 Youth who have mental health comorbidity have more health burden and disease complications across common childhood chronic medical illness. 10
In children with type 1 diabetes (T1D), a recent systematic review reported that greater than 30% of youth presented with depressive symptoms and these symptoms were frequently associated with poorer glycemic control. 11 Research also indicates that youth with T1D are at higher risk of suicide attempts and death by suicide than healthy youth. 12 However, there is very little research regarding youth with T2D and depression comorbidity.1,13 Thus, our team conducted a systematic literature review assessing the evidence base in youth with T2D and depression. This systematic review of the literature aimed to address the state of the science of mental health comorbidity in youth with T2D and address gaps in the literature for future research.
Methods
Information source and eligibility criteria
Our review was conducted based upon recommendations established by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses statement. 14 A search was conducted by a single author (MN), which included English-language articles published between February 28, 2010 and March 10, 2020 in peer-reviewed journals available on CINHL, Cochrane, Central, SCOPUS, and MEDLINE through PubMed. The search strategy included both free text and controlled vocabulary for the following terms: type 2 Diabetes Mellitus, Mental Disorders, Depression, Child, Adolescent, and Youth. A detailed description of the search strategy can be found in Supplemental Material Appendix I.
New research studies were included that evaluated children ages 10–17 who had been diagnosed with T2D and included data regarding glycemic control and complications of diabetes, as well as comorbid depressive disorders or depressive symptoms identified during clinical interaction (reported by patient, health care professional, or guardian). Studies that included youth ≥ 18 but reported < 18 data separately were included in our final analysis. Those studies that did not report <18 data separately were excluded. In addition, studies reporting only on individuals with type 1 diabetes or that included patients suffering from genetic syndromes known to cause co-occurring psychiatric and metabolic illness (i.e., Prader Willi Syndrome) were excluded. Review articles and editorials were also excluded.
Article selection
The title and abstract of each retrieved article were screened by the lead author (MM). Two authors (HH, EF) reviewed each of the full-text articles for inclusion and instances of disagreement were resolved by the lead author (MM). Figure 1 illustrates the process of article selection. See the appendix for details of the search strategy. Diagram of search strategy.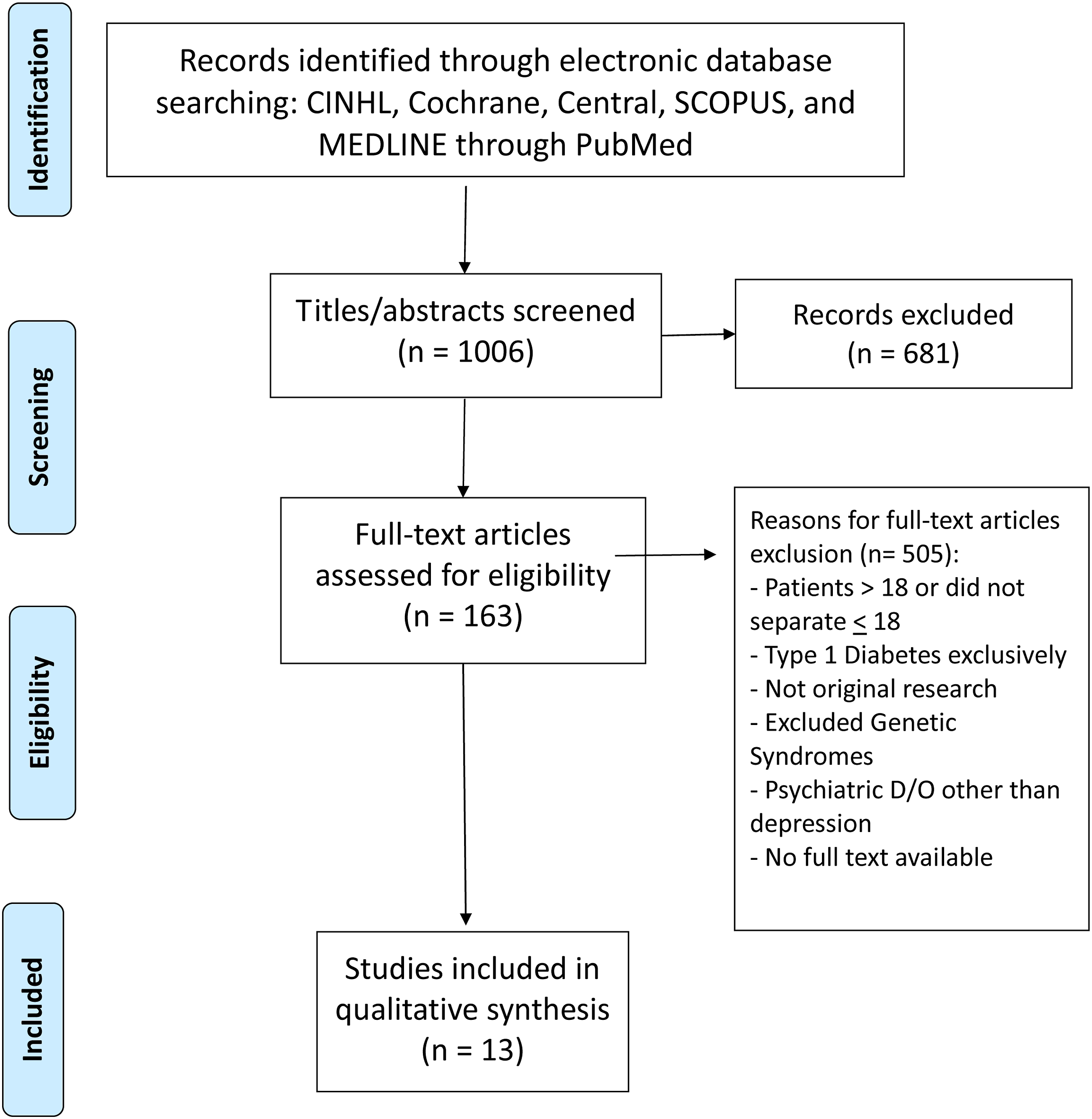
Results
Article selection
1006 articles were screened: 681 articles were excluded and 163 articles were selected for full-text review (Figure 1). Thirteen publications met final inclusion criteria.6,15-26
Characteristics of selected studies
Studies and sample
Summary of included articles.
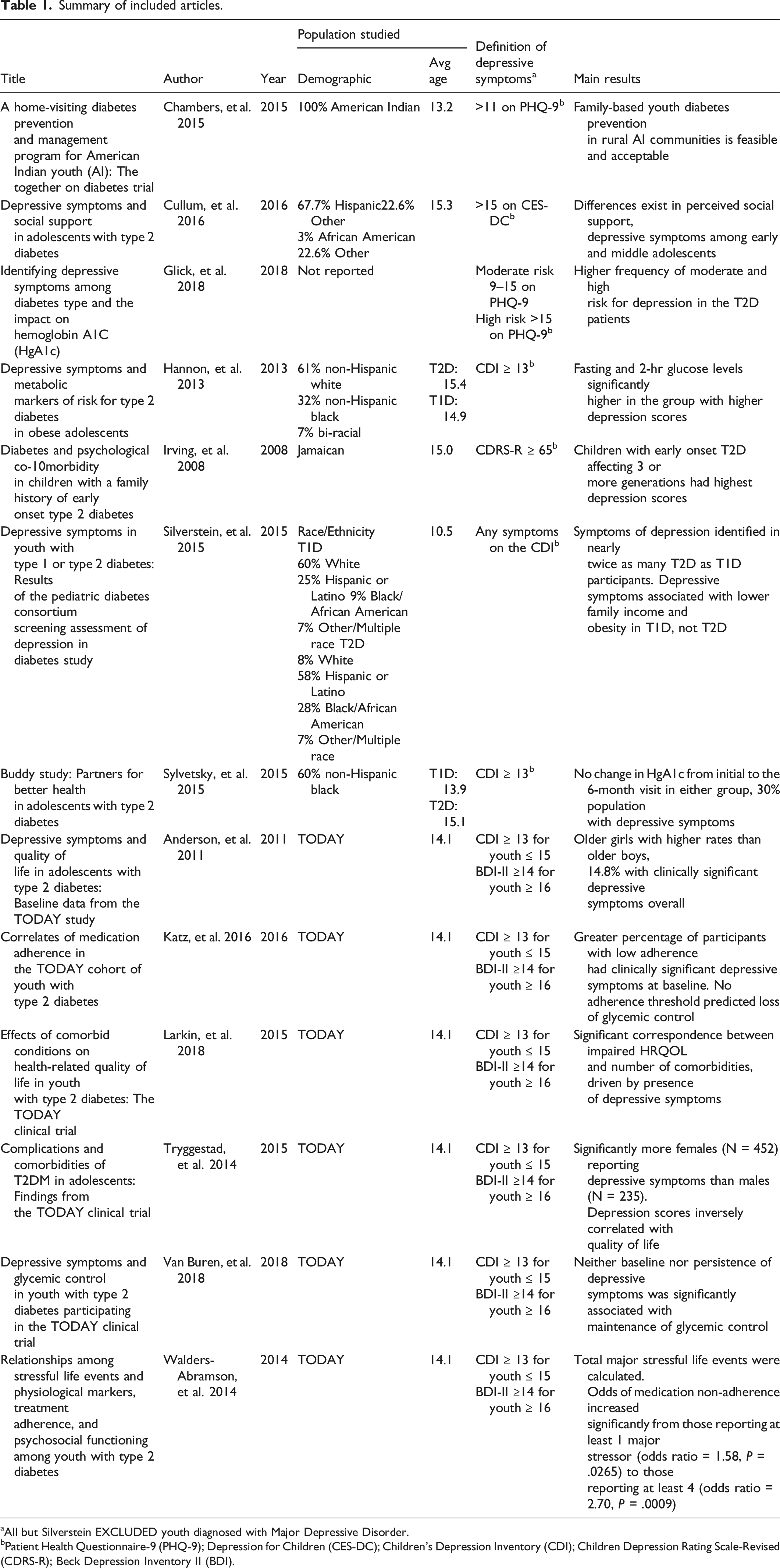
aAll but Silverstein EXCLUDED youth diagnosed with Major Depressive Disorder.
bPatient Health Questionnaire-9 (PHQ-9); Depression for Children (CES-DC); Children’s Depression Inventory (CDI); Children Depression Rating Scale-Revised (CDRS-R); Beck Depression Inventory II (BDI).
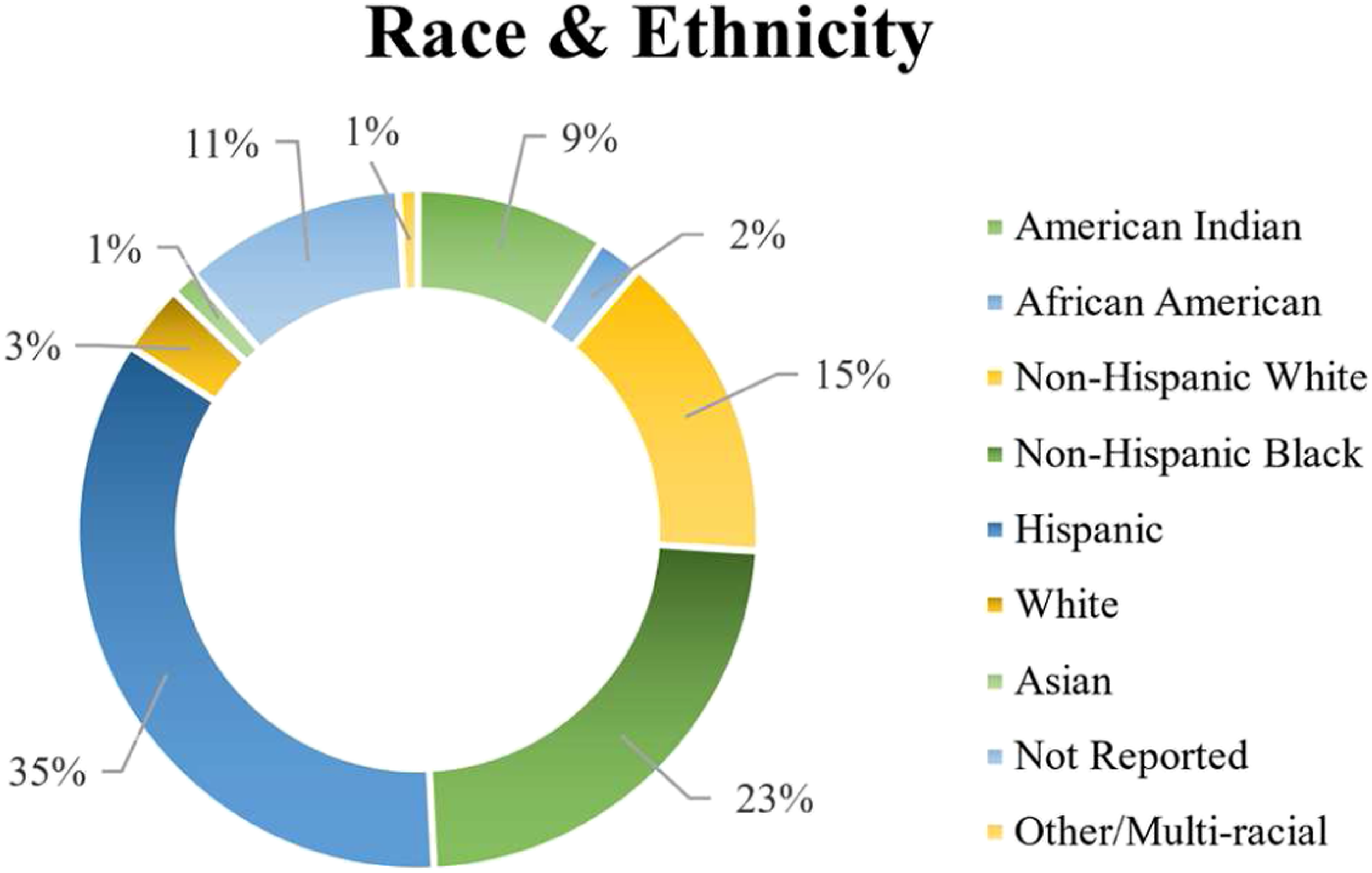
Race and ethnicity of included sample.
Key findings of systematic literature review examining depression among youth with T2D.
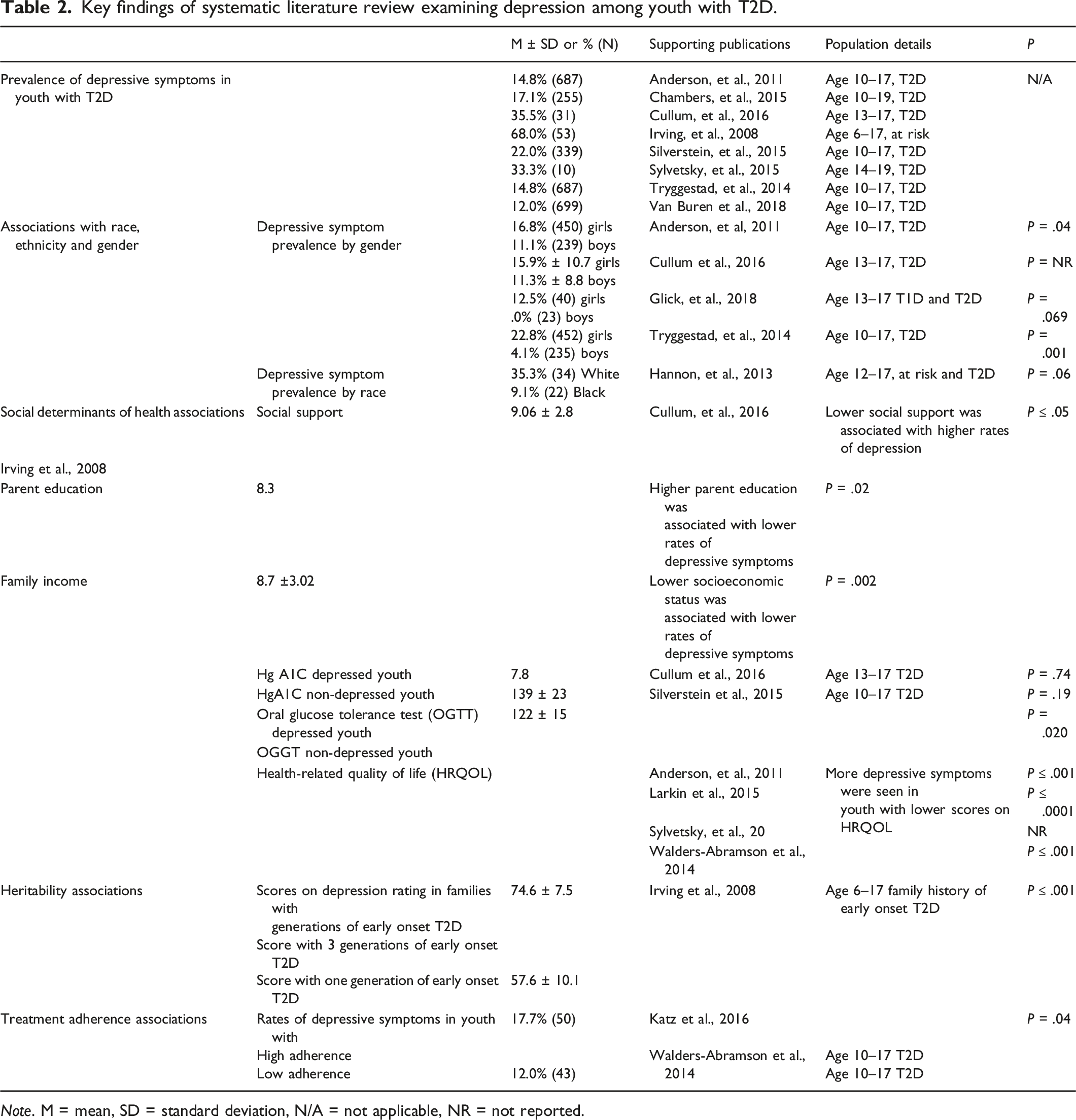
Note. M = mean, SD = standard deviation, N/A = not applicable, NR = not reported.
The majority of studies (8/13) excluded patients with prior diagnoses of psychiatric comorbidity. The TODAY cohort (6/13 included studies) excluded patients with a diagnosis of Major Depressive Disorder or those taking psychotropic medications at the time of enrollment. 15 2 additional studies excluded participants who met criteria for major depressive disorder or “other serious psychological disorders.”21,24 Ultimately, only 1 study included patients with a diagnosis of Major Depressive Disorder. 25
All studies evaluated depressive symptoms: 1 via the Centers for Epidemiological Studies—Depression for Children (CES-DC); 2 via the Patient Health Questionnaire-9 (PHQ-9); 9 by the Children’s Depression Inventory (CDI); and 6 by the Beck Depression Inventory II (BDI) In addition, 6 studies measured health-related quality of life using the Pediatric Quality of Life (PedsQL) scale. The frequency of these assessments are shown in Figure 3, and a description of the cut-offs used for each study are included in Table 1. Type of assessments used for depression.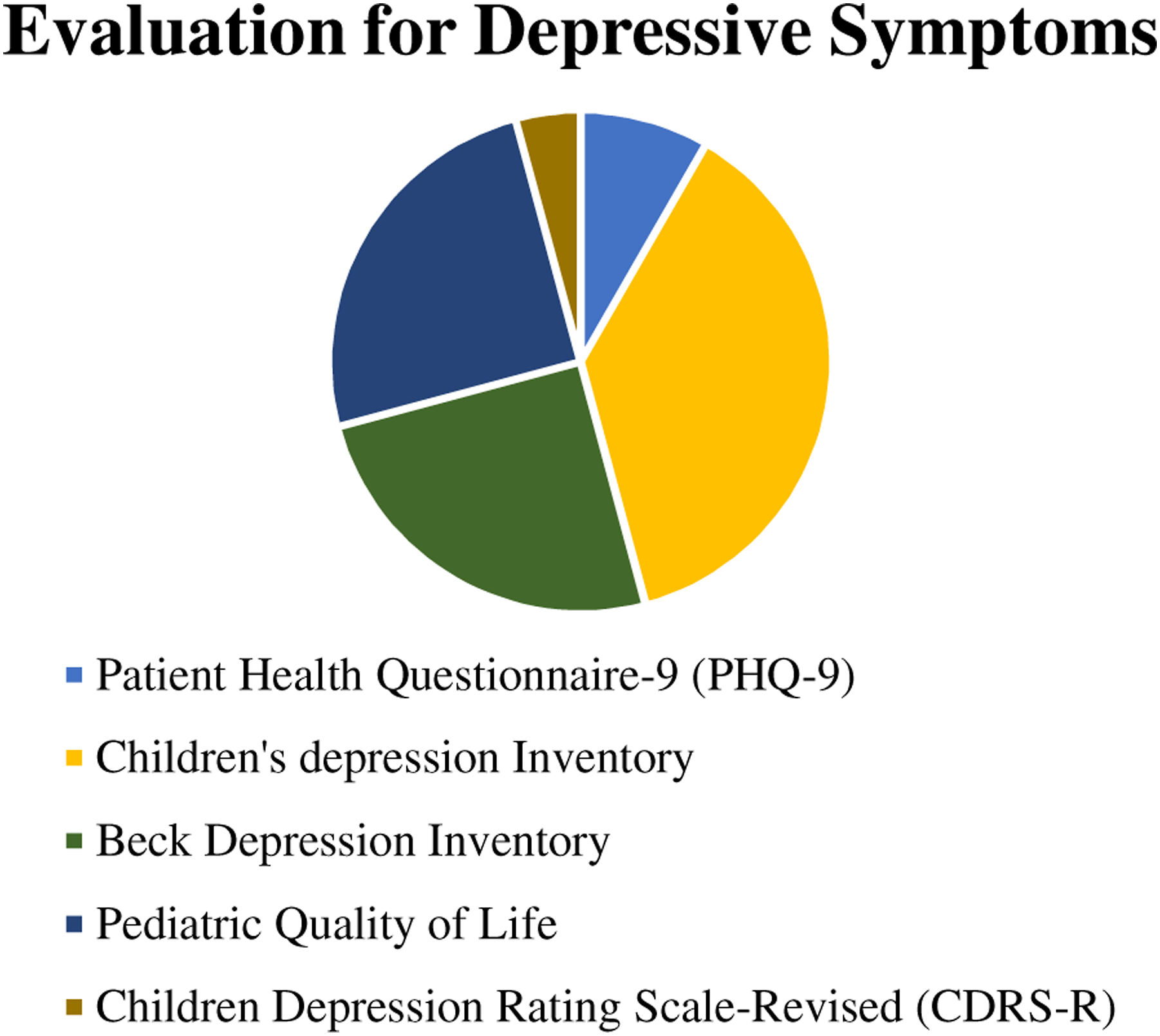
Notable among completed studies of the comorbidity of mental health and quality of life in youth with T2D was the TODAY clinical trial. Representing nearly half (6 of 13) of the studies identified in our search, the Treatment Options for Type 2 Diabetes in Adolescents and Youth (TODAY) study is the largest randomized study to assess the impact of early medical treatment for youth onset T2D on complications and comorbidities.
Summary of included TODAY publications
6 of the 13 included publications were results from The TODAY study, a multi-site randomized clinical trial funded by the National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK)that included 704 youth age 10–17 with T2D (M/F 246/458). 27 The TODAY study compared metformin monotherapy with 2 alternative approaches, 1 combining metformin with a second pharmacologic agent and 1 combining metformin with an intensive lifestyle intervention program and these approaches impact on glycemic control. During the course of the RCT, self-reported symptoms of depression and quality of life were collected.6,18
The TODAY related publications investigated correlates of depressive symptoms and T2D but excluded participants with Major Depressive Disorder or requiring psychotropic medication.6,15-17,28 Health-related quality of life (QOL) was inversely related to depressive symptoms. Older teen girls had the highest rates of clinically significant depressive symptoms. Depressive symptoms were also correlated with low adherence to diabetes treatment. The TODAY study also reported that an increased number of stressful life events were associated with elevated depressive symptoms, lower treatment adherence, psychosocial functioning, and impaired health-related QOL.6,15-19 The following is a brief summary of the results of each of the included TODAY publications. ANDERSON, 2011
15
Anderson et. al. reported on the baseline depressive symptoms and quality of life characteristics among a cohort of patients (n = 704) within the TODAY study. The authors reported that of those in the TODAY cohort, older girls displayed higher rates of clinically significant depressive symptoms than older boys and younger girls, acknowledging that girls comprised 65% of their sample with 61% being between aged 12–15 years. Older girls had more clinically significant depressive symptoms than either older boys or younger girls KATZ, 201616 Katz et. al. investigated predictors of medication adherence in the context of insulin action and glycemic control within the TODAY cohort (n = 699). Adherence to medication had a positive relationship with β-cell functioning and insulin sensitivity, but no relationship with insulinogenic sensitivity. Those with low medication adherence experienced more clinically significant depressive symptoms, with 12% as opposed to 18% of those with low medication adherence experiencing depressive symptoms (p=.04). Among all of the characteristics examined, the presence of baseline clinically significant depressive symptoms was correlated with low medication adherence. LARKIN, 2015
6
Larkin et al. evaluated health-related qualify of life (PedsQL) and comorbidities in a TODAY study cohort (n = 699). Hypertension, microalbuminuria, dyslipidemia and elevated depressive symptoms were comorbidities studied relative to health-related qualify of life (PedsQL). Among all comorbidities studied, only depressive symptoms predicted health-related qualify of life impairment in this sample.
6
TRYGGESTAD, 2015
17
Tryggestad and Willi examined the comorbidities and complications of T2D in adolescents (n = 699) enrolled in the TODAY study. The study noted that the complications and comorbidities of this sample are comparable to the adult population with T2D, but that the onset of these complications and comorbidities appear earlier in life. Consistent with other TODAY cohort studies, Triggestad et. al. reported 14.8% of youth with T2D had clinically significant depressive symptoms despite the exclusion of youth diagnosed with MDD or taking psychotropic medication at screening. VANBUREN, 2018
18
In a longitudinal analysis of 576 TODAY participants, Van Buren, et. al. showed that 69 (12%) had depressive symptoms at 1 of 3 study visits, 44 (7.6%) had depressive symptoms at 2 of 3, and 9 (1.6%) had depressive symptoms at all three visits. Of 493 participants without depressive symptoms at the initial screening, 39 (7.9%) subsequently developed clinically significant depressive symptoms at 6 and/or 24 months. WALDERS-ABRAMSON, 2014
19
Walders-Abramson looked at the relationships between T2D and stressful life events, treatment adherence, physiological markers, and psychosocial functioning among a cohort of TODAY participants (n = 497). The study concluded that an increased number of major stressors were related to odds of elevated depressive symptoms, lower treatment adherence, psychosocial functioning, and impaired health-related quality of life.
Other publications
CHAMBERS, 2015 20
This prospective interventional study of 225 American Indian youth (age 10–19) in 4 rural American Indian communities evaluated the “Together on Diabetes program,” a family-based, home-visiting diabetes prevention/management intervention, which included lifestyle education, psychosocial support, facilitated referrals, and community based healthy living engagement. 17% participants screened positive for depressive symptoms. Preliminary results suggest the intervention was feasible and well tolerated in American Indian youth with T2D.
CULLUM, 2016 21
In this cross-sectional study, Cullum et al. explored the relationships of perceived social support, body mass index (BMI), glycated hemoglobin A1c (HbA1c), months since diagnosis, and depressive symptoms in 31 youth (13–17 years) with T2D. Youth diagnosed with MDD or requiring psychotropic medication were excluded. Depressive symptoms were not significantly related to other variables; however, 35% of participants had clinically significant depressive symptoms during the study.
GLICK, 2018 22
In this observational study, Glick et al. assessed depressive symptoms in adolescents (13–17 years) with T1D (n = 467) or T2D (n = 63), excluding those with significant cognitive delay. This study assessed depression rates based on gender and diabetes type. Adolescents with T2D had higher depressive symptoms compared to those with T1D. HgA1c levels were higher in those at high risk vs low risk for depression, but there was no change in HgA1c levels 1-year later. The study also observed that girls with T2D had increased depressive symptoms compared to females with T1D. Girls also had increased depressive symptoms compared to boys.
HANNON, 2013 23
In this cross-sectional study, Hannon et al. studied depressive symptoms in 56 obese youth (age 12–17) at risk for early onset T2D. Authors found an association between greater depressive symptoms and increased fasting glucose levels and increased β-cell impairment.
IRVING, 2008 24
In this cross-sectional study, Irving et al. assessed 53 children (age 6–17) with family history of early onset T2D for risk of psychopathology. Participants were excluded if they had a diagnosed depressive disorder or other serious psychological disorder. Of the 53 children, 68% had depressive symptom scores indicating likely or very likely depressive disorder and 7.5% had T2D. Children with early onset T2D affecting ≥3 generations had the highest depressive symptom scores.
SILVERSTEIN, 2015 25
In this retrospective chart review, Silverstein et al. evaluated depressive symptoms (CDI) in youth (age 10–17) with T1D (N = 261) or T2D (N = 339) that were a part of the Pediatric Diabetes Consortium T1D and T2D registries. Symptoms of depression were seen in fewer (13%) of those with T1D compared to 22% of those with T2D (P = .007). Less than 20% of youth with depressive symptoms received treatment for those symptoms in the year when depressive symptoms were assessed.
SYLVETSKY, 2015 26
This prospective interventional study assessed the impact of social support via a volunteer partner intervention (The Buddy Study), on health and psychosocial outcomes in 10 adolescents (age 12–19) with T2D. Three participants reported depressive symptoms indicative of depression. The study was ended prematurely due to low enrollment, but baseline data showed health-related QOL was lower than scores in reported in youths without diabetes or in adolescents with T1D.
Key results from all included publications
There was a wide range of depressive symptoms reported across included studies, with rates ranging 14.8% to 68% across reports.17,18,21,24-26 Only 1 study reported a rate of depressive symptoms >30% with Irving et al. reporting symptoms at a rate of 68%. When the outlier is removed, the rate of depressive symptoms ranges from 14.8%–35.5%. No studies included clinical assessments of Major Depressive Disorder and all but 1 of the studies excluded youth with a diagnosis of Major Depressive Disorder that required treatment.
Girls with T2D reported greater rates of depressive symptoms than boys with T2D. There was a trend towards greater rates of depressive symptoms among White, non-Hispanic youth as compared to Black, non-Hispanic youth in those at high risk of T2D. In youth with T2D, psychosocial factors were inversely associated depressive symptoms, that is, youth with less psychosocial support showed more symptoms of depression.15,17,21-24
Families with several generations of early onset T2D also displayed higher rates of depressive symptoms in youth within those families at risk for T2D. In addition, there was a trend towards youth with T2D and depression having more difficulty with blood sugar control, but it did not reach statistical significance. There is an inverse association between health-related quality of life (HRQOL) and depressive symptoms or stressful life events in youth with T2D. In addition, non-adherence to T2D treatment was associated with higher rates of depressive symptoms.6,15,16,19,24,26
Discussion and conclusions
This systematic literature review that described the evidence base on comorbid depressive disorders in youth with T2D found a dearth of literature. There were a total of 13 reports derived from 8 studies and the total sample size was 2244 youth age 6–17. This limited literature likely does not represent the full range of youth with T2D. All but 1 of the included studies excluded youth with a diagnosis of Major Depressive Disorder and many excluded youth with any diagnosed psychiatric disorders limiting significantly the generalizability of the findings. Despite these exclusions, depressive symptoms were common in the included sample.
Many variables associated with an increased risk of depression in the general adolescent population also were associated with risk in the included review of adolescents with T2D. Girls with T2D reported higher symptoms as well as youth with less psychosocial support. However, depressive symptoms were higher in White, non-Hispanic youth as compared to Black, non-Hispanic youth with T2D. This is not consistent with youth without T2D but should be interpreted with caution because of the small number of Black, non-Hispanic youth studied and, again, because youth with MDD were excluded from most studies.15,17,18,21-26 The results suggest families with a history of T2D also showed higher rates of depressive symptoms. This is consistent with adult literature suggesting a link, metabolically, between mood disorders and diabetes risk. 29
There was a wide range of study design and heterogeneity in the definition of depressive symptoms within the included studies. The large prospective studies included were not designed to study the impact of depressive symptoms on T2D and, conversely, the handful of studies that did investigate the impact of depressive symptoms on T2D had small sample sizes and excluded youth diagnosed with MDD. The highly variable data of the identified studies suggests clear need for future studies of the relationship between depressive symptoms, extant diagnosis of T2D, and metabolic risk for development of T2D. Additionally, multiple studies suggested that unique populations, including those with comorbid depression, increased number of major stressors, decreased psychosocial support, multigenerational diagnosis of T2D, and socioeconomic disadvantages must be taken into account during these studies. Results suggestive of potential impact of race upon results indicate a need for further study in larger, more diverse samples. Finally, efforts to evaluate mechanistic pathways, as well as directionality of the association of depressive symptoms and T2D should be pursued in hopes that, by addressing whether treatment of depression in youth can fundamentally decrease long-term risk for T2D and diabetic complications for youth with T2D.
In addition, study design did not permit a clear understanding of how Major Depressive Disorder (MDD) may impact youth with T2D because individuals with a psychiatric diagnosis or in treatment for MDD were excluded from the majority of included studies. This represents a significant area of need for future research. Including youth with meet criteria for MDD and need treatment is an area where multidisciplinary research teams, including child psychiatry expertise, would benefit a vulnerable population. This would allow for studies on the impact of treatment of both T2D and MDD, an area where no research exists currently. In addition to excluding youth with MDD, the majority of the included studies were not designed to investigate the impact of depression on T2D outcomes or the inverse. Depressive symptoms, for the most part, were secondary analyses and thus limit definitive conclusions about the impact of MDD on T2D. Most importantly there were no studies designed to investigate the impact of the treatment of MDD on outcomes of T2D, allowing no conclusions to be drawn aside from a need for more research.
Ultimately, critical knowledge gaps remain in this growing health crisis. Rigorous research is need regarding the epidemiology of psychiatric illness and youth with T2D—although intuitively connected, rigorous research is needed to understand the rates of comorbidity, what populations are most at risk and how socioeconomic, gender and racial factors impact the interplay between psychiatric comorbidity and youth with T2D. In treatment studies of youth with T2D, there is a clear need to include those youth with active symptoms and diagnosable psychiatric illness. Research teams should include mental health providers to support those with psychiatric illness to determine if and how treatment of T2D impacts psychiatric illness. This approach has shown significant benefit in adults with comorbid psychiatric illness and T2D in treating T2D improving both glycemic measures and mood measures.30-32 The dearth of data in youth with T2D and psychiatric represents a missed opportunity for the current generation of children and adolescents and, consequently, a clear call for research in this doubly vulnerable population.
Supplemental Material
sj-pdf-1-ijp-10.1177_00912174211067335 – Supplemental Material for Mental health comorbidity and youth onset type 2 diabetes: A systematic review of the literature
Supplemental Material, sj-pdf-1-ijp-10.1177_00912174211067335 for Mental health comorbidity and youth onset type 2 diabetes: A systematic review of the literature by Molly McVoy , Heather Hardin , Erin Fulchiero , Kate Caforio, Farren Briggs, Mandy Neudecker, and Martha Sajatovic in The International Journal of Psychiatry in Medicine
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.