
Abstract
Objective
We explored whether a patient’s psychosocial background before allogeneic hematopoietic stem cell transplantation (allo-HSCT) could predict the occurrence of psychiatric symptoms during treatment and after hospital discharge.
Method
Logistic regression analysis was performed using INTERMED, a scale that comprehensively evaluates psychological factors such as psychiatric history, current mental status, and coping skills, and social factors such as social participation status, relationships with others, and living environment, which were used as independent variables. The Center for Epidemiologic Studies Depression Scale was used to measure depression, while the Profile of Mood States was used to measure anxiety and other symptoms. Both measures were used as dependent variables and were administered upon clean room admission, during clean room stay, at clean room discharge, and at 3, 6, and 12 months after hospital discharge.
Results
Participants included 70 patients (45 males and 25 females, mean age 53.3 ± 12.3 years). Thirty-eight patients participated in the program for the entire period, up to 12 months after hospital discharge. The total score on the Japanese version of the INTERMED and psychological factor scores assessed at baseline were significant predictors of depressed mood on discharge; however, there were no significant predictors of scores on the Profile of Mood States.
Conclusions
A comprehensive pretransplant evaluation of psychosocial background can help predict the appearance of psychiatric symptoms after allo-HSCT. In patients who are expected to develop psychiatric symptoms after allo-HSCT, it is important to consider early intervention by a specialist and close monitoring by a medical team.
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is a treatment for hematological diseases that are difficult to cure with chemotherapy alone. Improved results with allo-HSCT have enabled long-term survival. 1 However, long-term chemotherapy from the start of treatment to allo-HSCT, high-dose chemotherapy, total-body irradiation before allo-HSCT, and graft-versus-host disease, which is an adverse effect of allo-HSCT, can cause side effects such as fever, nausea, fatigue, and anorexia. In addition, high-dose anticancer therapy administered before transplantation reduces the hematopoietic function of white blood cells and neutrophils in the bone marrow, making patients less resistant to bacteria and viruses and more susceptible to infection. Bacterial and viral infections during treatment can directly result in death; therefore, optimal precautions must be taken. During treatment, patients spend most of their time in a sterile private room called the “clean room”. Clean rooms are equipped with specialized ventilation systems that ensure air purity, remove microorganisms and dust, and prevent bacterial and viral infections. To prevent infection, only medical personnel are allowed to enter clean rooms, and family members can only engage with patients through windows. In addition, patients living in clean rooms are prone to mental health problems owing to living in a specialized environment and under specialized rules, such as strict hygiene to prevent infection; patients can only eat certain foods; there are restrictions on what can be brought in; and patients frequently wash their hands and shower on their own. Therefore, mental isolation caused by prolonged hospitalization in the specialized environment of a clean room, various restrictions aimed at preventing infection, and limited family visits can be significant burdens on mental health. During hospitalization for allo-HSCT, it has been reported that 40% of patients present with psychiatric symptoms, such as adjustment and mood disorders.1-3 A comparison of psychiatric symptoms before and after hospitalization demonstrated that depressive mood, anxiety, insomnia, and poor concentration peaked around the day of allo-HSCT,4-6 indicating a significant mental burden during hospitalization. These symptoms improve over time; however, some persist upon hospital discharge. 7 Research has shown that psychiatric symptoms may persist for several years if the activities of daily living, which deteriorated during hospitalization, do not improve or if the symptoms of chronic graft-versus-host disease continue to interfere with daily life.8-10 Although psychosocial background is thought to influence the onset and long-term persistence of psychiatric symptoms, the relationship between psychosocial background and psychiatric symptoms in allo-HSCT recipients has not been well studied. Studies have reported that the presence of multiple psychosocial risk factors in recipients before organ transplant results in a decreased quality of life and prolonged residual anxiety and depression after organ transplant, suggesting that psychosocial background is a predictor of the development of psychiatric symptoms. 11 Patients hospitalized for respiratory diseases have been found to have more anxiety and depressive moods during hospitalization if their total INTERMED score was 20 or higher. 12 Therefore, depending on the course of treatment, allo-HSCT recipients are expected to have their quality of life affected by psychiatric symptoms and mental burden not only during hospitalization but also after hospital discharge. We hypothesized that by identifying the risk factors that are likely to induce psychiatric symptoms before allo-HSCT, preventive measures could be taken at an early stage to prevent the aggravation of psychiatric symptoms. This study aimed to prospectively determine the predictors of psychiatric symptoms during hospitalization and after hospital discharge using psychosocial background before allo-HSCT.
Method
Patients
Patients who had been hospitalized for allo-HSCT at the Department of Hematology/Oncology, Kurashiki Central Hospital, or the Department of Hematology, Tokai University Hospital, between April 1, 2017, and March 31, 2019, and who had received a direct explanation from a physician and signed a consent form in their own handwriting, were included in this study.
The exclusion criteria were as follows: patients with symptoms of impaired consciousness or dementia; those with worsening physical symptoms that made evaluation by questionnaire or interview difficult; those with speech, hearing, or visual impairment that affected their understanding of the evaluation procedures; those with psychiatric disorders other than depression; and those who were not first-time transplant recipients with a hematopoietic cell transplantation-specific comorbidity index score of 5 or higher. The hematopoietic cell transplantation-specific comorbidity index predicts the risk of complications and death following hematopoietic cell transplantation. At 2 years post-transplantation, treatment-related mortality is projected to be 14%, 21%, and 41% for a score of 0, 1-2, and 3 and above, respectively. In this study, we used this scale as an exclusion criterion because a score of 5 or higher indicated that the patient was in poor general health before transplantation; therefore, it would be difficult to participate in the study or be followed up for 12 months thereafter. 13
Data collection
Data on age, sex, hematological disorder, length of clean room stay, length of hospital stay, history of psychiatric consultation, ongoing psychiatric treatment, history of psychiatric treatment, history of psychotropic medications, period of education, occupation, marital status, and presence or absence of a period of education were collected.
Outcomes
INTERMED, a scale that comprehensively evaluates psychological factors, such as psychiatric history, current mental status, and coping skills, as well as social factors, such as social participation status, relationships with others, and living environment, was used to assess psychosocial risk and the urgency of the need for medical services. It was created in Europe as a tool to assess the risks and needs related to healthcare from multiple perspectives; the version used in this study has been translated into Japanese.
14
It consists of four major categories (physical, psychological, social, and healthcare) and comprises 20 questions. INTERMED is based on information in the medical record, information known to the health care providers directly involved in treatment and care, or interviews with the patient if any information is missing in the assessments of INTERMED. Scores are determined based on health care providers’ assessments obtained through conferences and meetings with the health care providers. Therefore, it differs from the common method of performing psychological tests, in which the patient provides their own answers. The evaluation was conducted at three time points (past [history], present [present illness], and future [prognosis]). For each question, a score of 0 (no vulnerability/risk, no need for therapeutic intervention/care), 1 (mild vulnerability/risk, careful observation, and preventive intervention/care should be provided), 2 (moderate vulnerability/risk, therapeutic intervention/care should be provided), or 3 (high vulnerability/risk, immediate intensive therapeutic intervention, and multidisciplinary care should be provided) was assigned, with a severity rating by the healthcare professional. No cutoff values were set; the higher the total score of the 20 questions, the more complex the intervention (Figure 1).
15
INTERMED domains and variables.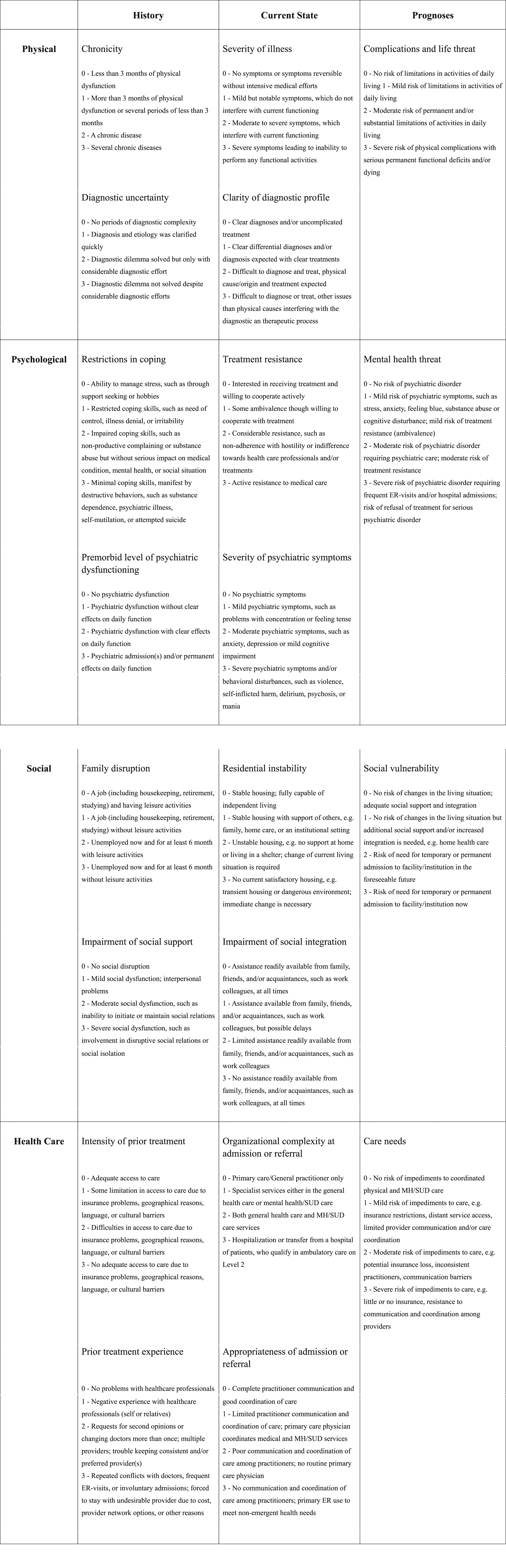
The Center for Epidemiology Studies Depression Scale (CES-D), a self-assessment scale developed by the U.S. National Institute of Mental Health, was used to assess depressive mood. The number of applicable days was checked on a 4-point scale for 20 questions about mental state in the past week as follows: 0 days, 0 points; 1-2 days, 1 point; 3-4 days, 2 points; and 5-7 days, 3 points. The higher the total score, the stronger the indication of increased depressive moods; a cutoff value of ≥16 was considered a clinically depressive mood.
The Japanese version of the Profile of Mood States (POMS) was used to assess anxiety and other mental states. Patients answer 30 questions in six categories (tension-anxiety, depression-dejection, anger-hostility, vigor, fatigue, and confusion) on a 5-point scale from “not at all” (0 points) to “very much” (4 points). Total mood disturbance was used to assess the overall mood. Lower scores indicated a better mood, except for “vigor,” where higher scores indicated a better mood.
The INTERMED results were evaluated at a multidisciplinary conference upon admission. POMS and CES-D were administered by a clinical psychologist at the following six time points: after admission to the hospital and before admission to the clean room (hereafter referred to as “before clean room admission”), 14 to 21 days from the date of implantation (hereafter referred to as “during clean room stay”), within 7 days from the time of leaving the clean room (hereinafter referred to as “after clean room discharge”), three months after hospital discharge, 6 months after hospital discharge, and 12 months after hospital discharge. The psychological test was not administered if the patient was in poor general health and unable to answer the psychological test independently, or if the physician in charge deemed it difficult to administer the psychological test.
Statistical analysis
At each time point during and after allo-HSCT (T2, T3, T4, T5, and T6), logistic regression analysis was performed to determine whether INTERMED before allo-HSCT (at T1) can predict depressive and overall mood, which were assessed using CES-D and POMS. The cutoff value for the CES-D was set at 16 points; therefore, a score of ≤15 and ≥16 was defined as no depression and depression, respectively. Each item on the POMS is a categorical variable, with a total score of <60 and ≥60 defined as good and bad mood, respectively. A receiver operating characteristic (ROC) curve was created using the four major INTERMED categories (physical factors, psychological factors, social factors, and healthcare), and the total INTERMED score as continuous variables, and the area under the ROC curve (AUC) and its confidence interval were calculated. The lower limit of the confidence interval (>.5) was considered predictable. The cutoff value for INTERMED was set to maximize the sum of sensitivity and specificity. The goodness of fit for the logistic regression was determined by performing the Hosmer-Lemeshow test. SAS 9.4 (SAS Institute Inc., Cary, NC, USA) was used for the statistical analysis. The significance level, set at 5%, and 95% confidence intervals (CIs), were calculated.
Results
Patient background
Patient background.
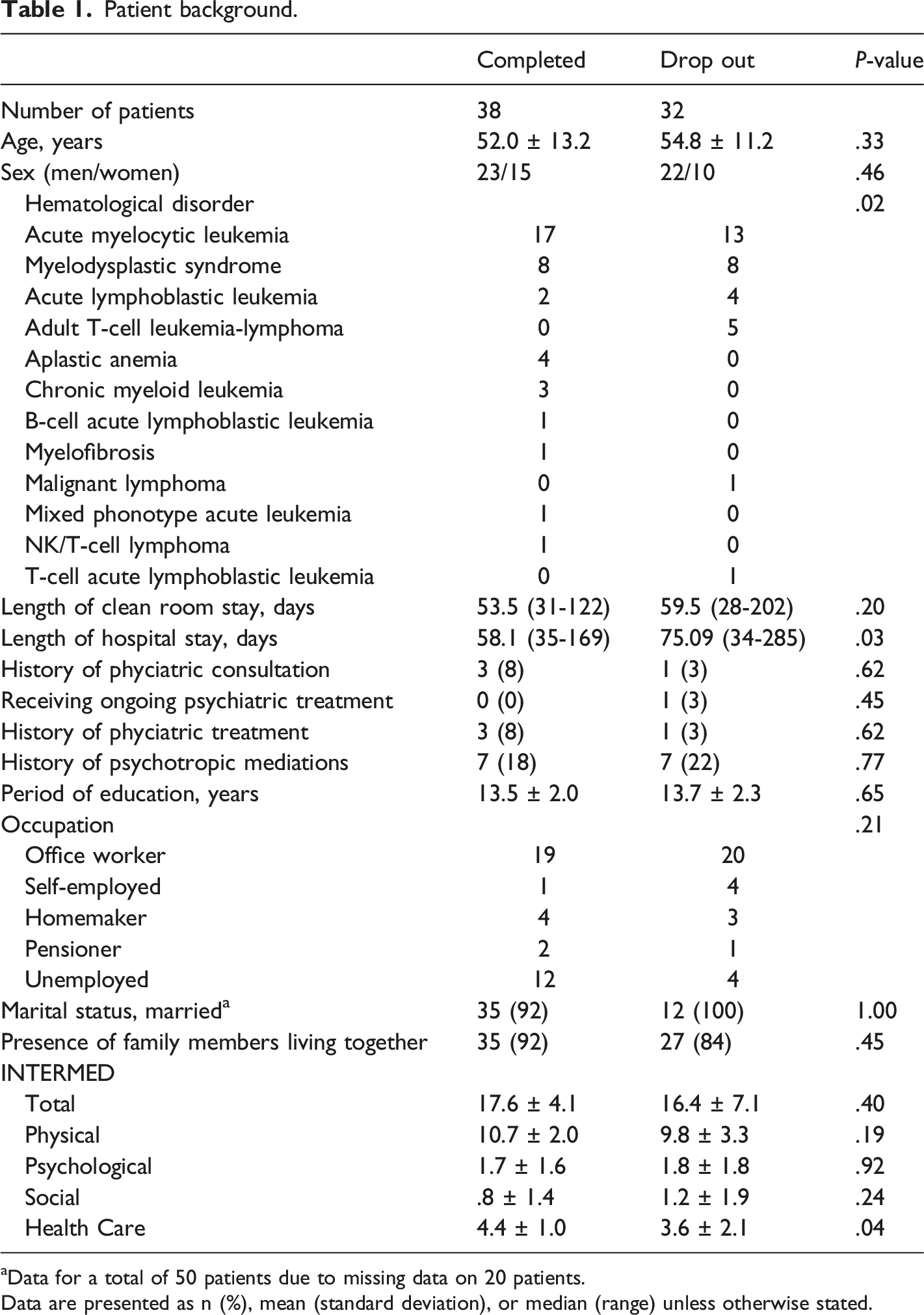
aData for a total of 50 patients due to missing data on 20 patients.
Data are presented as n (%), mean (standard deviation), or median (range) unless otherwise stated.
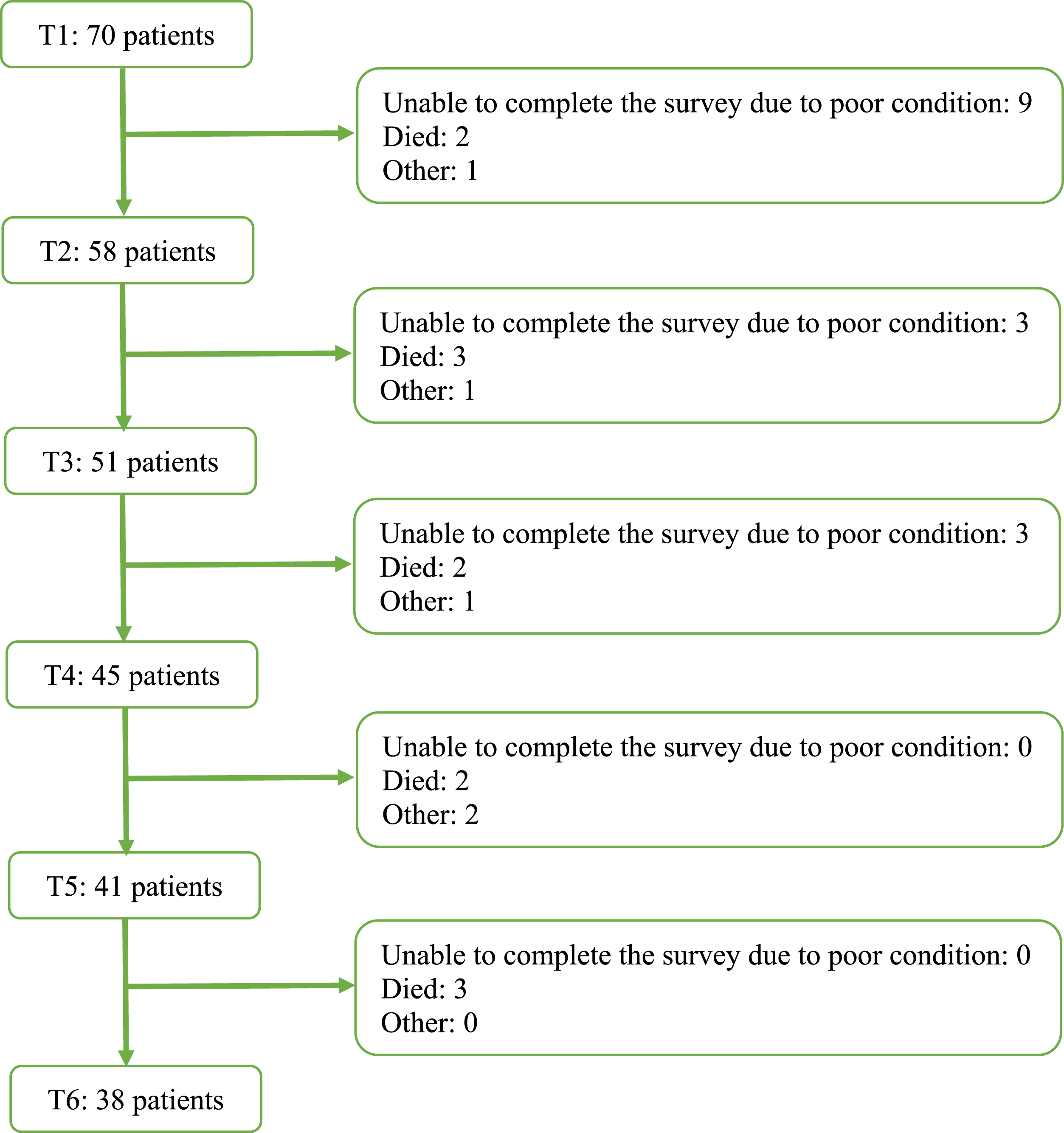
Reasons for discontinuation at all of the time points. T1 to T6 are time points at which patients were assessed: T1, before clean room admission; T2, during clean room stay (14-21 days after allo-HSCT); T3, within 7 days after clean room discharge; T4, 3 months after hospital discharge; T5, 6 months after hospital discharge; and T6, 12 months after hospital discharge.
CES-D and POMS results
CES-D and POMS results.

Data are presented as mean (standard deviation).
T1, before clean room admission; T2, during clean room stay (14 to 21 days after allogeneic hematopoietic stem cell transplantation); T3, within 7 days after clean room discharge; T4, 3 months after hospital discharge; T5, 6 months after hospital discharge; and T6, 12 months after hospital discharge.
Logistic regression analysis results
Results of logistic regression analysis.
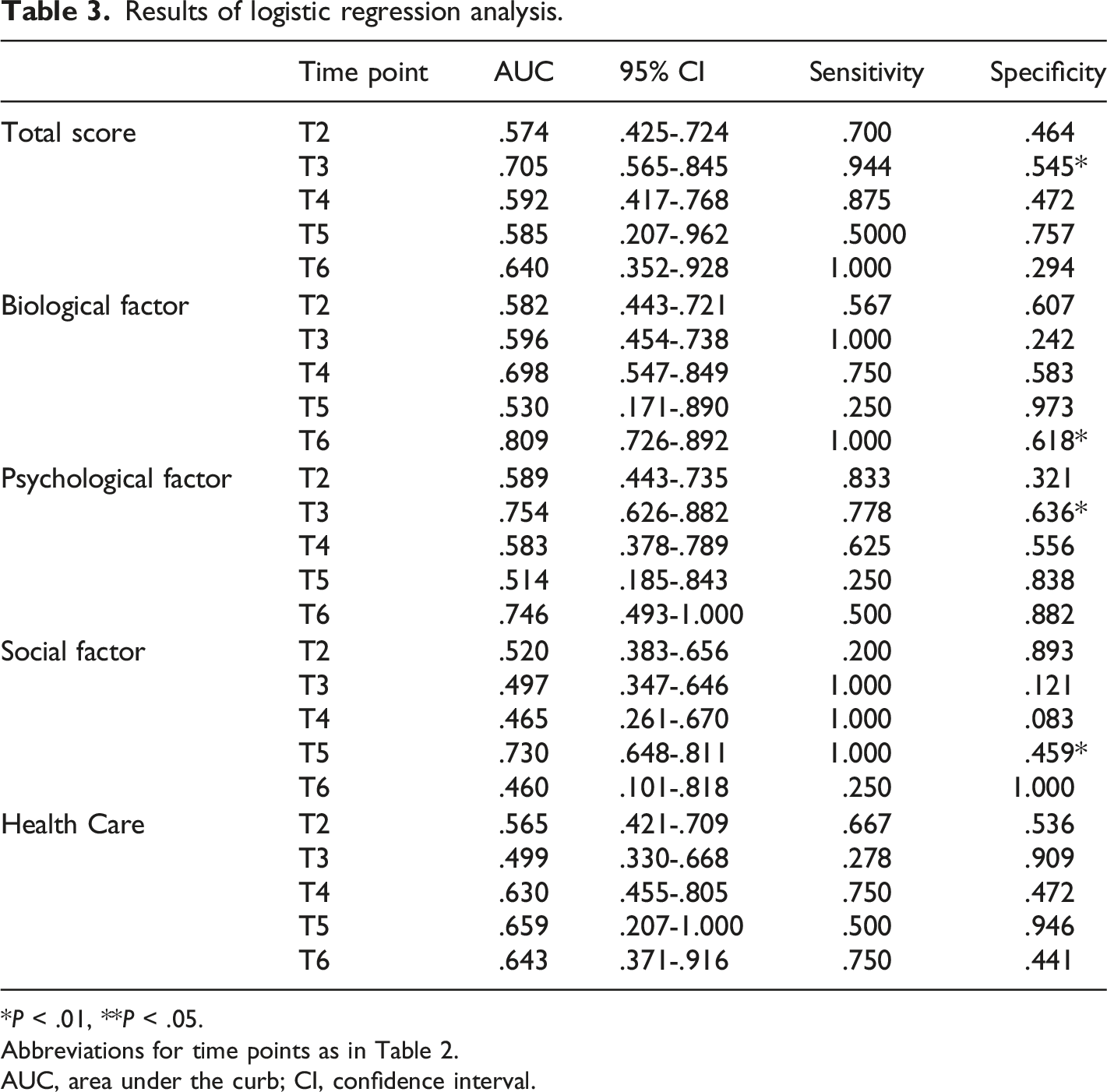
*P < .01, **P < .05.
Abbreviations for time points as in Table 2.
AUC, area under the curb; CI, confidence interval.
Discussion
This study examined whether INTERMED before allo-HSCT could predict psychiatric symptoms during a clean room stay, upon clean room discharge, and after hospital discharge. The results indicated that the total INTERMED and psychological factor scores were useful predictors of depressive symptoms at T3. The relationships between psychosocial background, mood state, and psychiatric symptoms after allo-HSCT have previously been reported. Yalvaç and colleagues 16 reported that psychiatric symptoms identified by screening before allo-HSCT were anxiety (57%), adjustment disorder (23%), and depression (10%), and that in patients undergoing allo-HSCT, 58% had a psychiatric consultation, 84% exhibited symptoms of anxiety or depression, and about 30% were diagnosed with an adjustment or mood disorder.
The presence or absence of depressive mood and psychiatric symptoms before allo-HSCT may be important indicators of transplantation therapy. Tecchio et al. 17 reported that patients with high trait anxiety during a clean room stay had neurotic tendencies on the Eysenck Personality Questionnaire Brief Version (EPQ/BV) before allo-HSCT and that the State-Trait Anxiety Inventory and Karnofsky Performance Status below 90 before allo-HSCT predicted trait anxiety during a clean room stay. In this study, a total INTERMED and psychological factor score of ≥18 and ≥2, respectively, before allo-HSCT were predictors of depressive symptoms upon clean room discharge, suggesting that patients with such scores require close monitoring for psychiatric symptoms and other preventative measures. Patients whose total INTERMED score and psychological factor score exceeded the cutoff value did not necessarily exhibit depressive symptoms during hospitalization but were more prone to depressive symptoms than those whose scores did not exceed the cutoff values. The probability of having depressive symptoms was .353 (18/51) without INTERMED; increased 1.5-fold to .531 (17/32) with a total INTERMED score of ≥18; and significantly decreased to .053 (1/19) with a total INTERMED score of <18. Even if psychiatric symptoms, including depressive symptoms, were not present before allo-HSCT, referral to a specialist may be beneficial for the patient. 18
Although this study did not examine changes in CES-D scores after hospital discharge in patients with depressive moods, patients with psychiatric symptoms, upon hospital discharge, may continue to have symptoms for several years.8-10 No previous study has examined the predictability of future mood or psychiatric symptoms using INTEREMED in allo-HSCT recipients. However, several reports from other fields have mentioned the predictability of future mood and psychiatric symptoms. In liver transplant recipients, the predictive utility of post-transplant mood was examined. A 1-point increase in the total INTERMED score was associated with a .93-point increase in the EuroQol score and a .93-point increase in the Hospital Anxiety and Depression Scale, which assesses anxiety and depression. 19 In patients with urological disorders, a total INTERMED score of ≥21 at diagnosis was associated with higher anxiety and depression scores three months after diagnosis, and the predictive utility of the total INTERMED score and subsequent mood status had also been clarified. 20 The predictability of post-transplant psychiatric symptoms based on the INTERMED score before allo-HSCT in this study may be supported by previous studies. Although exploratory, our findings on the predictors of psychiatric symptoms in allo-HSCT recipients provide an indicator that can be used in clinical practice. One of the features of INTERMED used in this study is that it incorporates past and future perspectives, such as the current state and multiple items, in addition to psychological assessments. In the questionnaire-based evaluation used in previous studies, patients rated themselves subjectively, whereas in this study, scoring was performed at conferences with the medical staff directly involved in the treatment. This objective and multifaceted evaluation of patients differed from previous studies.
In addition, allo-HSCT requires collaboration among multiple professionals, and a comprehensive pretransplant evaluation is considered useful for sharing information among professionals and clarifying checkpoints common to all professionals. One limitation of this study is that it did not consider the psychological impact of physical burden during the treatment period.
Physical symptoms caused by the primary disease, side effects associated with chemotherapy, and the grade of graft-versus-host disease, depending on the immune response after allo-HSCT, were ignored. Furthermore, the amount of physical activity upon hospital discharge, which may influence subsequent psychiatric symptoms, was not examined. In clinical practice, there is a correlation between the degree of physical burden and changes in mental health. 21 However, this needs to be clarified in future studies.
Limitations
This study has 2 major limitations. First, the sample size was small and did not allow for randomized comparisons. The number of patients undergoing hematopoietic stem cell transplantation was small at each institution that performed the transplants. The second limitation is attributable to the high dropout rate. As transplantation itself is a physically demanding treatment and transplantation-related deaths are common, discontinuation due to poor general health and transplantation-related deaths were the main reasons for dropping out.
Conversely, although the sample size was not large, the fact that a comprehensive pretransplant evaluation was conducted, which allowed assessment of psychiatric symptoms upon leaving the clean room, should contribute to improving the quality of transplantation care in the future. This study did not consider the psychological impact of the various physical side effects that occur due to high-dose anticancer therapy and graft-versus-host disease during hospitalization. Future studies considering these points are warranted.
Conclusion
Comprehensive pretransplant evaluation using scores of past psychiatric history, current mental status/adaptation, coping skills in the environment, and outlook for future psychiatric symptoms may contribute to predicting depressive mood upon leaving the clean room after allo-HSCT.
Footnotes
Author contributions
Takashi Imamura; Data curation, Investigation, Visualization, Writing – original draft. Takeshi Sudo; Conceptualization, Data curation, Investigation, Writing – review & editing. Yasushi Orihashi; Formal analysis, Writing – review & editing. Yuki Takahashi; Writing – review & editing. Yuichi Ohnishi; Writing – review & editing. Makoto Onizuka; Writing – review & editing. Katsunaka Mikami; Writing – review & editing. Yasunori Ueda; Writing – review & editing. Kenji Yamamoto; Conceptualization, Methodology, Writing – review & editing, Supervision.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Takashi Imamura declares no conflicts of interest associated with this manuscript.
Takeshi Sudo declares no conflicts of interest associated with this manuscript.
Yasushi Orihashi reports personal fees from Evastem Co., Ltd. and Association of Medical Education and Ethics, outside the submitted work.
Yuki Takahashi declares no conflicts of interest associated with this manuscript.
Yuichi Onishi has received honoraria from Takeda Pharmaceutical Co., Ltd.
Makoto Onizuka declares no conflicts of interest associated with this manuscript.
Katsunaka Mikami has received a Grant-in-Aid for Scientific Research (C) (Number 22K07624) and financial support from Otsuka Pharmaceutical Co., Ltd., and Shionogi & Co., Ltd.; honoraria from Miyarisan Pharmaceutical Co., Otsuka Pharmaceutical Co., Ltd., Shionogi & Co., Ltd., Sumitomo Pharma Co., Ltd., and Takeda Pharmaceutical Co., Ltd.; and a consulting fee from Otsuka Pharmaceutical Co., Ltd., Shionogi & Co., Ltd., and Viatris.
Yasunori Ueda declares no conflicts of interest associated with this manuscript.
Kenji Yamamoto reports grants from Grants-in-Aid for Scientific Research (C)(22K07588), grants and personal fees from Eisai Co., Ltd., grants and personal fees from Otsuka Pharmaceutical Co., Ltd., personal fees from Meiji Seika Pharma Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Pfizer Japan Inc., Mitsubishi Tanabe Pharma Corporation, Shionogi & Co., Ltd, Eli Lilly and Company, EA Pharma Co., Ltd., Merck Sharp & Dohme, personal fees from Viatris Inc., Astellas Pharma Co., Ltd. , Takeda Pharma Co., Ltd. , outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was conducted with the approval of the Ethics Committee of Kurashiki Central Hospital (approval no. 2546) and the Ethics Committee of Tokai University School of Medicine (approval no. 17R002) and was reviewed in accordance with the “Ethical Guidelines for Medical and Health Research Involving Human Subjects.”