
Abstract
Background
Growing evidence has shown that hypovitaminosis D is a risk factor for developing schizophrenia and comorbid conditions. Therefore, this study aimed to examine the effect of vitamin D supplementation on serum levels of vitamin D, metabolic factors related to insulin resistance (IR) and the severity of the disorder in patients with schizophrenia.
Methods
Forty-eight chronic male patients with schizophrenia with vitamin D deficiency (≤20 ng/mL= (≤50 nmol/l) were selected and randomly assigned to vitamin D treatment and placebo groups. Subjects were supplemented for 8 weeks with vitamin D (2000 IU/day) or placebo.
Results
Within-group comparison revealed that the vitamin D group had a significant reduction in waist circumference, Positive and Negative Syndrome Scale – total score (PANSS-TS), and glycogen synthase kinase 3 beta (GSK-3β) levels (P = .022, P = <.001 and P = .013, respectively). On the other hand, the placebo group showed a significant increase in the level of fasting serum insulin and Homeostatic Model Assessment of Insulin Resistance (HOMA-IR) (P = .003 and P = .003). The between-group comparison showed a significant difference in terms of PANSS-TS, GSK-3β, fasting serum insulin (FSI), and HOMA-IR (P = .022, P = .048, P = .013 and P = .014 respectively).
Conclusions
Among vitamin D deficient patients with schizophrenia, vitamin D supplementation may affect GSK-3 β, an important biomarker in schizophrenia and insulin resistance. In addition, vitamin D supplementation in such patients may reduce the disorder’s symptom severity.
Introduction
Schizophrenia is a severe, complex, and usually chronic disorder that characterized by heterogeneous positive (including hallucinations, delusions, and disorganized thinking), negative (including Lack of motivation or apathy, Reduced emotional expression or blunted affect, Anhedonia or reduced ability to experience pleasure), cognitive, and mood symptoms,1–3 although there has been extensive research on the etiology of schizophrenia, nutritional factors, such as vitamin D, deficiency may be a risk factor. Epidemiological studies have shown that hypovitaminosis D in early life may have been associated with a later increased risk of schizophrenia. Also, according to epidemiological studies; it seems that the low level of vitamin D in adults is also related to the increase in the incidence of schizophrenia.4–6
Vitamin D, as a neuro-hormone, contributes to the brain's development and adult brain function.7,8 Preclinical findings showed that Vitamin D is involved in the regulation of brain enzymes, neurotransmitters, and the synthesis of brain neurotrophins such as nerve growth factor (NGF).9–11 Various animal studies have found that severe vitamin D deficiency or vitamin D receptor (VDR) gene deletion disrupts neural development and increases the risk of psychiatric diseases including depression, anxiety, and schizophrenia.12,13 Studies have also suggested that there was clear evidence of an association between vitamin D deficiency and altered expression of many proteins in the mitochondria, cytoskeleton, and synapses of the hypothalamus and frontal cortex.14,15 Data suggests that there may be a potential role for vitamin D in the development of schizophrenia.10,16–20 In a meta-analysis of 36 observational studies conducted in 2020, with a total of 12528 participants, patients with schizophrenia were more likely to have vitamin D deficiency compared to healthy controls. 21
Treatment with antipsychotic medications leads to a high incidence of metabolic syndrome in patients with schizophrenia. Several factors can play a role in the occurrence of metabolic syndrome in these patients, as shown in a systematic review conducted by Sneller et al found that higher baseline BMI, higher current BMI, higher age, concomitant use of mood stabilizers, earlier using Second-Generation Antipsychotics, higher dose, longer duration of treatment, psychosis and tobacco smoking, hypo-adiponectinemia, elevated levels of C-reactive protein (CRP) and higher white blood cell (WBC) count, the rs1414334 C-allele of the HTR2C-gene was associated with metabolic syndrome in patients with schizophrenia. 22
Glycogen synthase kinase 3 (GSK-3) is a serine-threonine kinase expressed in all tissues with two isoforms α and β. It has been shown that the β isoform is abundantly expressed in the human central nervous system (CNS) and regulates various cellular processes including gene expression, cell proliferation, and differentiation. 23 It has been reported that disrupted expression and activity of GSK-3 are associated with mental illnesses. 24 Some physiological factors signaling pathways such as PI3K (phosphoinositide 3-kinase)/AKT can inhibit GSK-3β.24,25 N-terminal serine phosphorylation of GSK-3β (ser9-GSK-3β) caused by these factors inactivates GSK-3 β, while tyrosine phosphorylation (TYR216- GSK-3β) will activate it. 26 Insulin leads to the phosphorylation of GSK-3 β via the PI3k/Akt signaling pathway, while impaired insulin action results in decreased phosphorylation and consequently elevated activation of GSK-3 β in the brain. GSK-3 β has been involved in the development of IR, based on its role in the regulation of glycogen synthesis. Bersudsky et al described measuring the GSK-3β in the blood could serve as a marker for central abnormalities of the GSK-3 β. 27
Studies in the field of schizophrenia indicate the presence of abnormalities in serum insulin levels in these patients. In the study of Li and his colleagues, which evaluated fasting serum insulin, fasting glucose, HB1AC, and diabetes in patients with schizophrenia, it was observed that the increase in fasting insulin could be a causal factor in the pathogenesis of schizophrenia, while the schizophrenia-associated variants had a non-significant effect on fasting insulin levels. 28
Studies showed that Vitamin D and its receptor can activate the PI3K/AKT cascade or reduce the GSK-3β activity. 29 The result of an in vitro study on neuroblastoma cells showed that treatment with vitamin D can be a potential nutritional factor to stimulate PI3K and AKT and also can significantly decrease GSK3β expression. 30
Changes in the activity or protein levels of GSK-3 β have been reported in patients with schizophrenia by several studies.31,32 A decrease in the serine residue phosphorylation level of GSK-3β in the frontal cortex has been found in postmortem studies conducted on patients with schizophrenia brains. 33 In addition, the levels of AKT as an inhibitor of GSK-3β in lymphocytes, hippocampus, and frontal cortex are reduced in patients with schizophrenia.34,35
As far as we searched, no study has been done to examine the effect of vitamin D supplementation on serum levels of GSK-3β in patients with schizophrenia. Thus, this study aimed to evaluate the effect of vitamin D supplementation on serum levels of 25-hydroxy vitamin D, factors related to IR, and severity of the disorder in vitamin D deficient patients with schizophrenia.
Materials and Methods
Ethical Approval
The trial protocol was approved by the Ethics Board of the Tabriz University of Medical Sciences (IR.TBZMED.REC.1397.1025) and registered with the Iranian Registry of Clinical Trials (code: IRCT20190313043039N1). Written informed consent was also obtained from a first-degree relative of each patient before the participant were enrolled into the study.
Study Subjects and Procedures
This study included 42 patients recruited from among inpatients at Razi hospital, Tabriz University of Medical Sciences (Tabriz, Iran). The date range of study was from May 2020 to February 2021. The inclusion criteria were as follows: male patient diagnosed with schizophrenia according to Diagnostic and Statistical Manual of Mental Disorders, fourth Edition, Text Revision (DSM-IV-TR) criteria, total Positive and Negative Syndrome Scale (PANSS) scored 70-120 at the baseline, vitamin D deficiency [≤ 20 (ng/mL = ≤ 50 (nmol/L)] and age 18-65 years old; the exclusion criteria were subject with mental retardation (Intelligence Quotient <70, use of Vitamin D or other nutritional supplements for at least 6 months prior to enrollment, simultaneous onset of other major psychiatric disorders, or changes in treatment and medication during the intervention.
Randomization was performed using a random numbers table and then participants were allocated into two groups: treatment group (n = 21) or placebo group (n = 21). Treatment group received 2000 IU of vitamin D3 (cholecalciferol) every day and the placebo group received a placebo (paraffin soft gel capsules) for 8 weeks. All researchers and patients were blinded during the study until the end of statistical analysis. For each patient, a set of demographic variables (age, marital, residency and smoking status, and duration of disease) were collected.
Schizophrenia Severity Assessment
PANSS was used to assess general psychopathology and symptom severity of the disorder at the baseline and end of the trial. This tool was published in 1987 by Stanley Kay, Lewis Opler, and Abraham Fiszbein and has a 30-item scale composed of subscales to assess negative (seven items), positive (seven items), and general psychopathological (sixteen items) symptoms of schizophrenia. Each subscale is rated from 1 to 7 points ranging from absent to extreme (1 = absent, 2 = minimal, 3 = mild, 4 = moderate, 5 = moderate severe, 6 = severe, and 7 = extreme). The range for the Positive and Negative Scales is 7-49, and the range for the General Psychopathology Scale is 16-112. The PANSS total score is between 30 and 210 and determines the severity of schizophrenia as follow: 58 points mildly ill, 75 points moderately ill, 95 points markedly ill and 116 points severely ill. 36
Biochemical Measures
Fasting venous blood samples (10 mL) were obtained at the beginning and after the 8 weeks of intervention. The samples were centrifuged, and serums were isolated and stored at −80°C until analysis. The quantitative chemiluminescent immunoassay (CLIA) method was used to determine serum levels of vitamin D and the enzyme-linked immunosorbent assay (ELISA) kits were used to measure serum levels of total GSK-3β (Bioassay Technology Laboratory) and insulin (Pars Azmoon). Serum levels of fasting blood glucose (FBG) were determined by enzymatic methods. Model Assessment for Insulin Resistance (HOMA-IR) was calculated according to the formula: fasting insulin (μU/mL) x fasting glucose (mg/dL)/405. 37
Anthropometric measurements
Participants' height was determined using a scale-mounted stadiometer to the nearest .5 cm, and their weight was measured with light clothing to the nearest .1 kg using a calibrated scale (Seca, Hamburg, Germany); body mass index (BMI) was calculated as weight/height2. Waist circumference (WC) was measured at the midpoint between the lower margin of the last palpable rib and the top of the iliac crest to the nearest .5 cm using a non-extendable measuring tape (SECA, Hamburg, Germany). All the measurements were performed by one person to minimize the error rate. Dietary calorie intake was assessed using 3-day diet records.
Statistical Analyses
To determine the sample size, basic information including the mean and standard deviation of the PANSS positive subscale variable was obtained from Graham et al.'s study.
38
Considering 95% confidence, 80% test power, two-tailed test and using the formula:
The sample size in each group was calculated to be 21 people.
Data analysis was done using SPSS version 16.0 (SPSS Inc, Chicago, IL). Kolmogorov-Smirnov test was employed to check the normal distribution of data. Normally distributed variables were reported as mean and standard deviations, whereas non-normally distributed variables were presented as geometric mean (minimum–maximum). Independent samples t test, chi-square test and Fisher exact test were used to compare continuous and categorical variables between groups. For nonnormal distribution of variables, logarithmic transformation was applied. Within-group differences before and after the intervention were evaluated by the paired t test and Analysis of covariance (ANCOVA) test was used to control the effect of confounding variables and determine the differences between the two groups post-intervention. A P value ≤.05 was considered statistically significant.
Results
Participants Description
Baseline Characteristics of Participants.
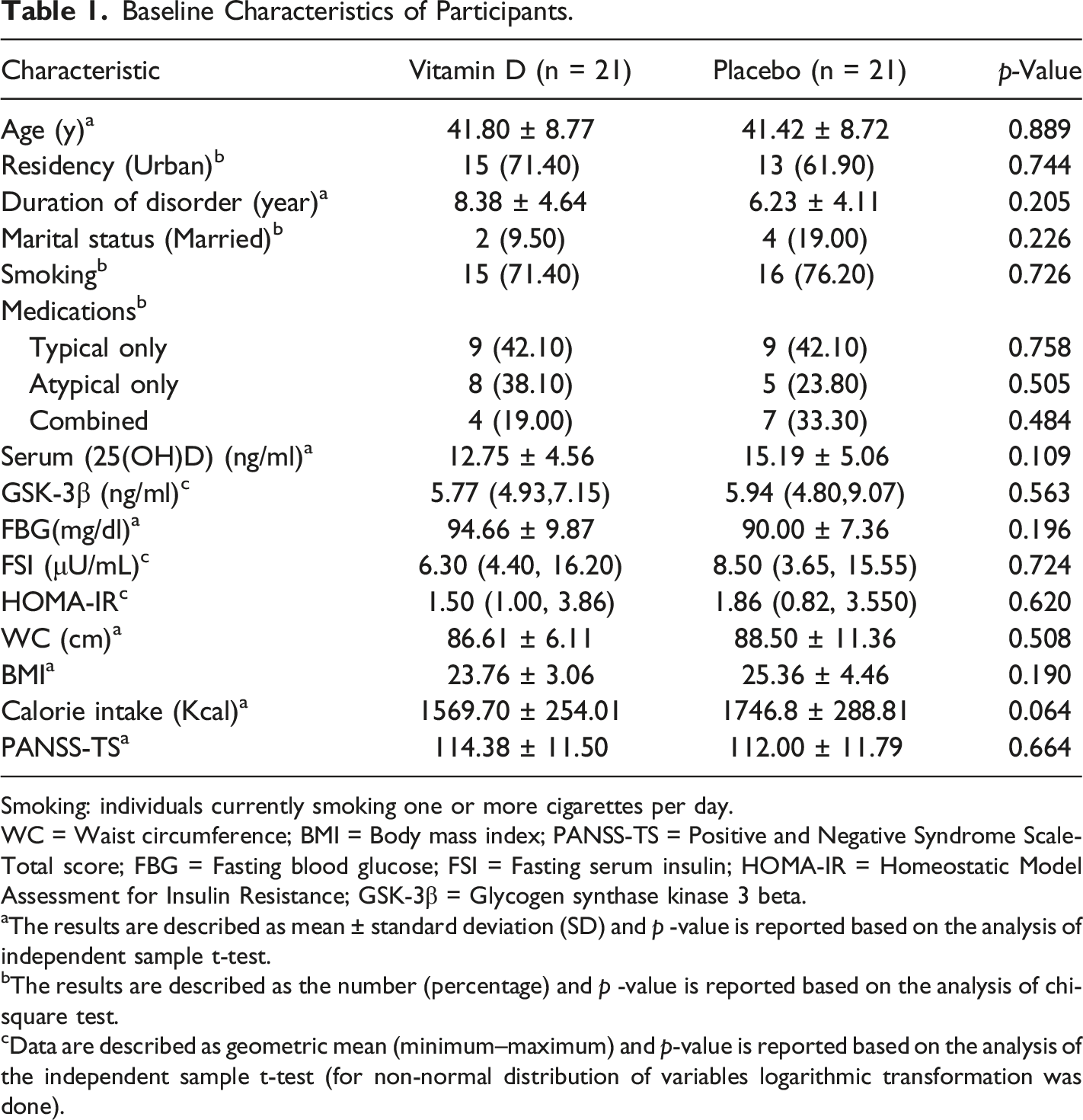
Smoking: individuals currently smoking one or more cigarettes per day.
WC = Waist circumference; BMI = Body mass index; PANSS-TS = Positive and Negative Syndrome Scale-Total score; FBG = Fasting blood glucose; FSI = Fasting serum insulin; HOMA-IR = Homeostatic Model Assessment for Insulin Resistance; GSK-3β = Glycogen synthase kinase 3 beta.
aThe results are described as mean ± standard deviation (SD) and p -value is reported based on the analysis of independent sample t-test.
bThe results are described as the number (percentage) and p -value is reported based on the analysis of chi-square test.
cData are described as geometric mean (minimum–maximum) and p-value is reported based on the analysis of the independent sample t-test (for non-normal distribution of variables logarithmic transformation was done).
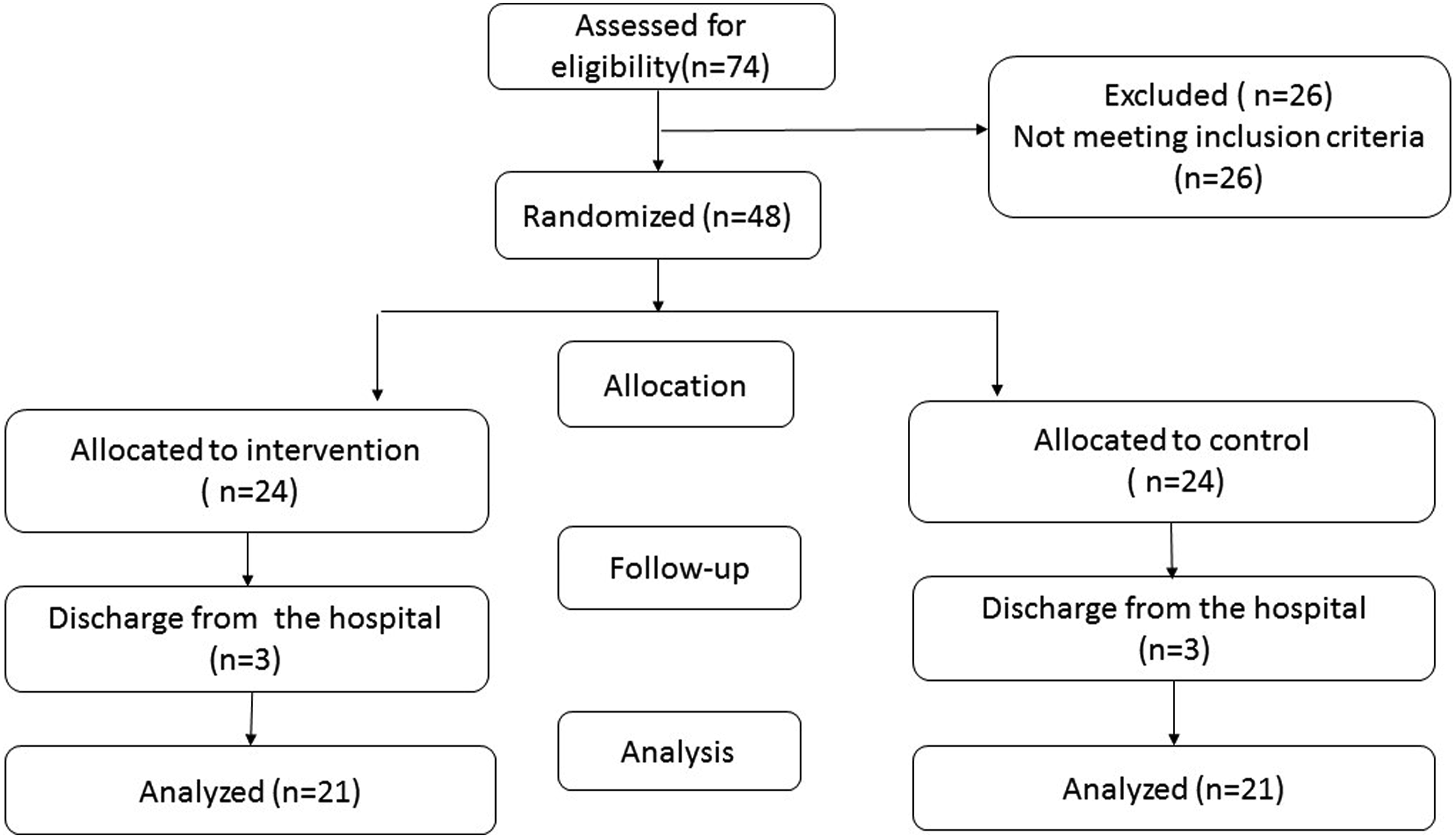
Flow diagram.
Serum Levels of 25-Hydroxy Vitamin D
Within and Between Group Comparisons of Serum Vitamin D, Anthropometric Data and Severity of Symptoms in Patients With Schizophrenia Before and After the Intervention.
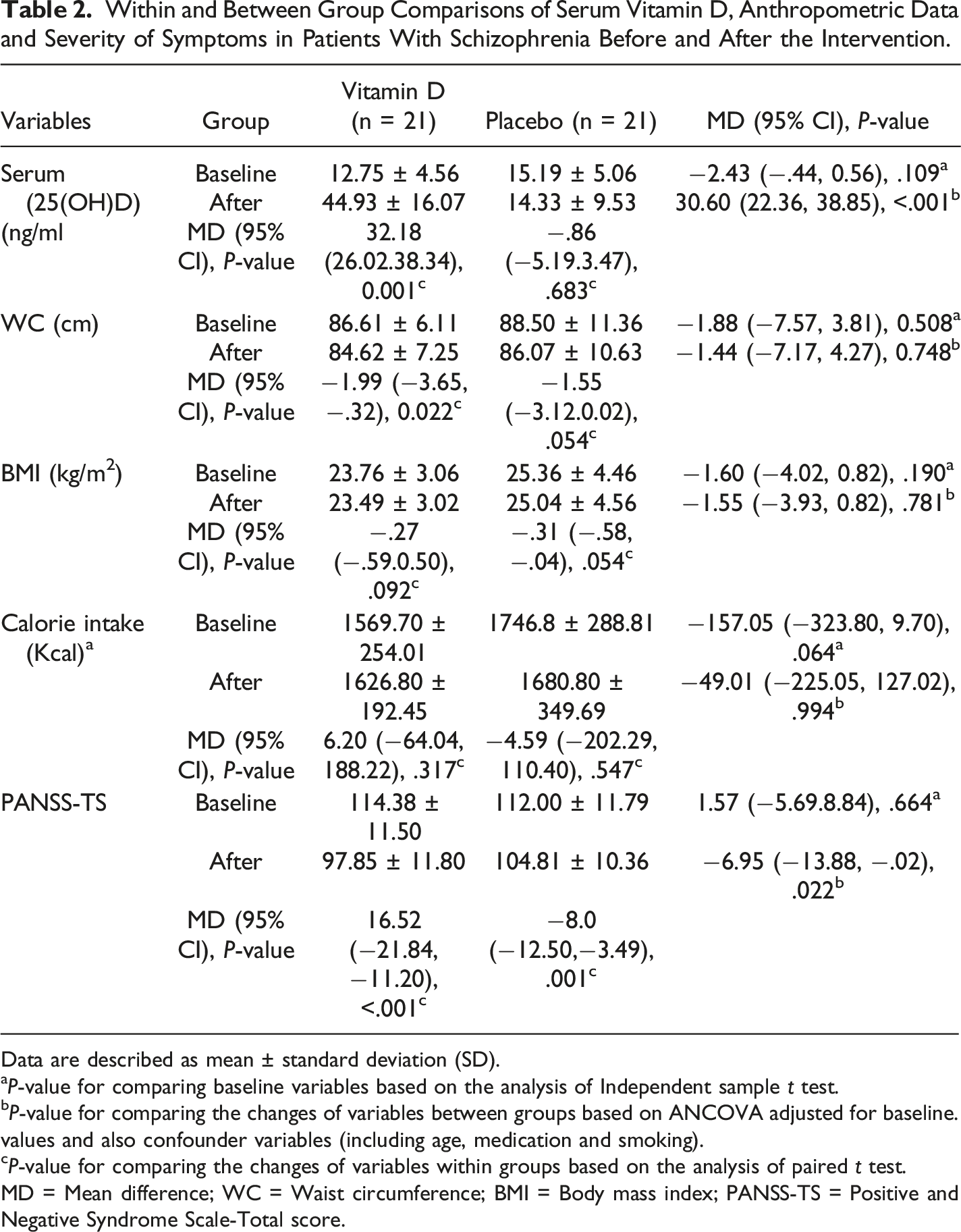
Data are described as mean ± standard deviation (SD).
aP-value for comparing baseline variables based on the analysis of Independent sample t test.
bP-value for comparing the changes of variables between groups based on ANCOVA adjusted for baseline.
values and also confounder variables (including age, medication and smoking).
cP-value for comparing the changes of variables within groups based on the analysis of paired t test.
MD = Mean difference; WC = Waist circumference; BMI = Body mass index; PANSS-TS = Positive and Negative Syndrome Scale-Total score.
Anthropometric Factors and Calorie Intake
As shown in Table 2, a significant decrease was observed in WC in the treatment group after supplementation (P = .022). No significant changes in caloric intake before and after the intervention were observed in both groups (P ≥ .05).
Disorder severity
After 8 weeks supplementation, the mean PANSS-TS reached from 114.38 ± 11.50 to 97.85 ± 11.80, and from 112.00 ± 11.79 to 104.81 ± 10.36 in treatment and placebo groups, respectively (P < .001 and P = .001). The results of ANCOVA showed that there were significant differences between the two groups regarding the post-intervention PANSS-T score (P = .040) (Table 2).
Serum Levels of Glucose, Insulin, HOMA-IR and GSK-3β
Within and Between Group Comparisons of Metabolic Factors Related to IR in Patients With Schizophrenia and After the Intervention.
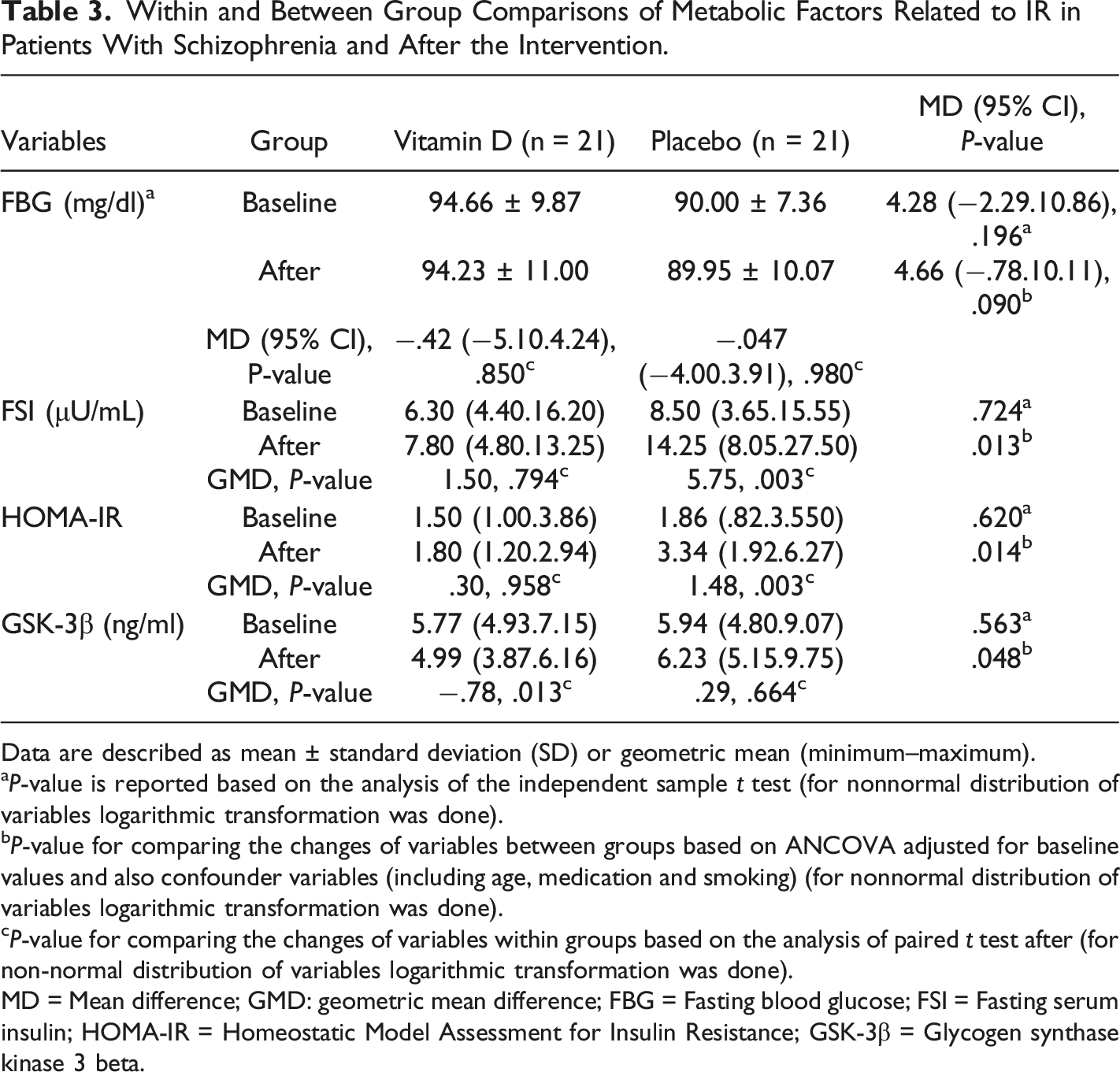
Data are described as mean ± standard deviation (SD) or geometric mean (minimum–maximum).
aP-value is reported based on the analysis of the independent sample t test (for nonnormal distribution of variables logarithmic transformation was done).
bP-value for comparing the changes of variables between groups based on ANCOVA adjusted for baseline values and also confounder variables (including age, medication and smoking) (for nonnormal distribution of variables logarithmic transformation was done).
cP-value for comparing the changes of variables within groups based on the analysis of paired t test after (for non-normal distribution of variables logarithmic transformation was done).
MD = Mean difference; GMD: geometric mean difference; FBG = Fasting blood glucose; FSI = Fasting serum insulin; HOMA-IR = Homeostatic Model Assessment for Insulin Resistance; GSK-3β = Glycogen synthase kinase 3 beta.
After 8 weeks, although Fasting serum insulin (FSI) and HOMA-IR did not significantly change in the treatment group, but in the placebo group, FSI showed a significant increase (P = .003) and the same trend was seen for HOMA-IR (P = .003). Between-group comparison based on ANCOVA, adjusting for baseline values and confounding variables, demonstrated a significant difference in FSI and HOMA-IR between treatment groups (P = .013 and P = .14, respectively).
Discussion
Our results showed that a daily supplementation dosage of 2000 IU vitamin D for 8 weeks significantly increased serum levels of vitamin D in the treatment group. Similarly, a study in patients with schizophrenia with low levels of vitamin D (<75 nmol/l) showed 8 weeks' supplementation with vitamin D (14 000 IU/weekly), could significantly increase serum levels of vitamin D in the vitamin D group. 39 A number of studies have also shown that the trend of a rise in serum vitamin D levels may occur during 2 months of supplementation.40,41
The cause of high levels of hypovitaminosis D in patients with schizophrenia could be related to some factors including poor nutrition, a sedentary lifestyle, low exposure to the sun, the overlap of 70 genes between schizophrenia and vitamin D-related genes, and excessive smoking.42,43
After the intervention, there was a significant decrease in the PANSS-TS in the treatment group compared to the placebo group. The finding is in agreement with the findings of previous investigations. Krivoy et al 39 found Vitamin D supplementation was associated with a trend towards improved cognition subscale of PANNSS in patients treated with clozapine and supplemented with vitamin D (14 000 IU/weekly) after 8 weeks. 39 Ghaderi et al 44 reported that supplementation with vitamin D (50 000 IU every 2 weeks) and 8 × 109 CFU/day probiotic for 12 weeks decreased disorder severity based on the general and PANSS-TS in patients with schizophrenia. 44 Given the extensive roles of the vitamin D in the protection and development of neurons, 45 the effect of vitamin D supplementation on the severity of the disorder in patients suffering from vitamin D deficiency was predictable and according to several studies, serum levels of vitamin D can be associated with its activity in different parts of the brain. 46 There are some postulated mechanisms for the effect of vitamin D on the development of schizophrenia and the severity of its symptoms. First, dysfunction in dopamine systems has been proposed in the pathophysiology of schizophrenia. 47 Moreover, Vitamin D is a potent stimulus of the glial cell line-derived neurotrophic factor (GDNF), suggesting that GDNF is crucial for the survival of dopaminergic neurons. 48 In rodent models with developmental vitamin D–deficient, the absence of vitamin D ligand in gestation reduced GDNF receptors, proto-oncogene tyrosine-protein kinase receptor Ret (C‐Ret) expression. 49
Second, genome-wide association studies (GWAS) have shown that genetic variants of L-type voltage-gated calcium channel (L-VGCC) subunits are correlated with an increased risk for schizophrenia. 50 The active form of vitamin D is modulating L-VGCCs in peripheral and brain tissues, and in the opposite, suboptimal concentrations of vitamin D could alter brain maturation through modulation of L-VGCCs and reducing calcium influx which associated with behavioral dysfunction. 51
Third, a decrease in N-methyl-d-aspartate (NMDA) receptor function is associated with schizophrenia. 52 Reduced NMDA transmission may cause dopamine abnormalities, synaptic connectivity and worsen glutamatergic function. 53 , 54 It has been reported in a number of studies that Vitamin D deficiency leads to novelty-induced hyper locomotion (correlate with positive symptoms) in response to NMDA-antagonists. 55 , 56 On the other hand, hypofunction of NMDA can occur due to glutathione deficiency. Glutathione levels are reduced in the cerebrospinal fluid and prefrontal cortex of schizophrenia patients. 57 According to the literature active form of vitamin D increases glutathione expression in rat astrocytes. 58
At the endpoint, we noted a significant decrease in serum levels of GSK-3 β in the treatment group. In addition, there was a difference between the vitamin D and placebo groups with regard to GSK-3β levels in 8-week supplementation. To the best of our knowledge, this is the first study to investigate the effect of vitamin D supplementation on the serum levels of GSK-3 β in schizophrenia patients. As mentioned above, the PI3K/AKT/GSK-3 β signaling pathway has a major role in neuron function and could be regulated with many extracellular signals such as nutrients. 24 Vitamin D has been studied as one of these nutrients in a number of articles. 29 , 59 , 60
AKT, which is activated by PI3K, has a significant contribution to cell survival and regulates the size of neurons and apoptosis. 61 – 63 Three types of AKT isoforms have been identified in mammalian cells: AKT 1, AKT 2, and AKT 3. AKT 1 seems to be more associated with schizophrenia. 35 Some studies have reported AKT1 level abnormalities in lymphocytes and different parts of patients with schizophrenias' brains. 64 , 65 AKT is known as a negative regulator of GSK-3ß and its failure to set in patients with schizophrenia will affect GSK-3β disruption. 27 Several studies reported an increased level of GSK-3β in patients with schizophrenia. In a study by Joaquim et al. GSK-3β platelet levels were higher in drug-naive patients with first-episode psychosis (FEP) than in the healthy group, and the phosphorylated GSK-3β levels or the total enzyme activity (rGSK3β) did not change after one month of treatment with antipsychotics. 66 In addition, Emamian et al. reported increased GSK-3β kinase activity among patients with schizophrenia. 34
In the present study, vitamin D supplementation, based on the findings of a number of previous studies, showed an increase in GSK-3β levels in patients with schizophrenia compared to the healthy group, and decreased serum GSK-3β levels after 8 weeks of supplementation.
Mechanisms of increased GSK-3β levels in patients with schizophreniawith vitamin D deficiency can be thought of as follows: vitamin D deficiency is associated with the dysregulation of PI3K and AKT expression, 60 and these abnormalities can lead to decreased activity of GSK-3 β. 60 It has been documented that dysregulation of neurotransmitters in the CNS can occur due to vitamin D deficiency. 67 , 68
On the other hand, neurotransmitters, including serotonin, dopamine, and glutamate, could modulate the action of GSK-3β. 69 , 70 Vitamin D deficiency from this path can also cause abnormalities in the regulation of GSK-3β. 71 – 73
Although serum insulin levels and insulin secretion did not change in the vitamin D group, given the increase in these factors in the placebo group after the intervention, it may be inferred that vitamin D may prevent insulin resistance due to prescribing antipsychotics.
Limitation
The study had some limitations. Because a woman who is eligible for our study was not hospitalized on the date of sampling, sampling was done only on men, which can be considered a limitation of the present study. Small sample size and recruitment of subjects from a single hospital were other limitations of the study. Further factors in signaling pathways and phosphorylated GSK-3β levels could not be considered due to cost constraints, and all patients were treated with different classes of antipsychotic medications, which could affect the results of the study, although we tried to adjust the effect of these factors through the statistical tests.
Conclusions
This study found a beneficial effect of vitamin D supplementation on reducing serum levels of GSK-3β and severity of psychotic symptoms in vitamin D-deficient hospitalized patients with schizophrenia. Further studies with larger sample sizes, longer durations, and higher doses of vitamin D supplementation are needed to confirm these findings.
Supplemental Material
Supplemental Material - A randomized controlled trial of Vitamin D supplementation in Iranian patients with schizophrenia: Effects on serum levels of glycogen synthase kinase‐3β and symptom severity
Supplemental Material for A randomized controlled trial of Vitamin D supplementation in Iranian patients with schizophrenia: Effects on serum levels of glycogen synthase kinase‐3β and symptom severity by Parinaz Kalejahi, Sorayya Kheirouri, Seyed Gholamreza Noorazar in The International Journal of Psychiatry in Medicine.
Footnotes
Acknowledgements
The authors would like to thank all the patients who participated in the study and all the people who contributed to this research project. All authors were involved in manuscript writing and approved the final manuscript.
Authors’ Contribution
Sorayya Kheirouri and Parinaz Kalejahi: concept and design the study. Seyed gholamreza Noorazar: diagnosis and introduction of patients. Parinaz Kalejahi: data collection and interpretation of the data. sorayya Kheirouri, Parinaz Kalejahi and Seyed gholamreza Noorazar: wrote the manuscript with input from all authors. All authors discussed the results and contributed to the final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is supported by Tabriz University of Medical Sciences, IRAN supported this study (Grant number: 61676)
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.