
Abstract
Background
Poststroke depression (PSD), with an approximately one third prevalence in stroke patients, is associated with increased morbidity and mortality. This study investigated the relationship between serum brain-derived neurotrophic factor (BDNF) levels and early-onset PSD, along with other clinical variables.
Methods
Clinical data and radiological images of 88 patients diagnosed with acute ischemic stroke were examined. Serum BDNF levels were measured within the first 72 hours following stroke diagnosis. On the 14th day following stroke diagnosis, Montreal Cognitive Assessment (MoCA), Hamilton Depression Rating Scale (HAMD17), and National Institutes of Health Stroke Scale (NIHSS) were administered to the patients.
Results
Serum BDNF levels (P = 0.022) and MoCA values (P = 0.004) of patients with early-onset PSD were significantly lower, and NIHSS values (P = 0.027) were significantly higher compared to patients without early-onset PSD. There was a significantly negative correlation between BDNF value and HAMD-17 score. Receiver operating characteristic (ROC) analysis was used to investigate the extent that BDNF level could predict early-onset PSD, and cut-off values were determined. For a BDNF cut-off value of 361.5, sensitivity and specificity values were 75% and 56%, respectively, indicating that serum BDNF levels could serve as a useful predictor of early-onset PSD.
Conclusion
Lower serum BDNF levels are associated with early-onset PSD and may serve as a potential biomarker, although causal conclusions are limited due to the study's cross-sectional design.
Introduction
Poststroke depression (PSD) is considered one of the most important stroke complications, which is often difficult to diagnose. PSD affects approximately one third of stroke patients and is associated with challenges in the rehabilitation process, decreased functionality, and increased morbidity and mortality. PSD symptoms manifest as suicidal ideation, feelings of worthlessness, decreased concentration, sleep disturbances, weight changes, anhedonia, psychomotor agitation, and fatigue; most patients do not have notable sadness and despair. Its various physical symptoms, including fatigue, tension-type headache, anxiety, loss of appetite, and sleep disorders, are more frequently observed. 1 Depressive symptoms usually occur during the first 3 months of stroke. 2 The clinical picture which includes the onset of depressive symptoms within the first 2 weeks of a stroke is called early-onset PSD. 3 It is well-established that depressive symptoms have a more severe course and are associated with worse functional outcomes in early-onset PSD compared to late-onset PSD. 2
As the mechanisms responsible for the etiopathogenesis of PSD are yet to be elucidated, there is an ongoing need for reliable biomarkers, and early diagnosis of PSD is still difficult. Its pathogenesis is complex and multifaceted, and it is believed that biological, social, functional, and psychological mechanisms might be involved. Hypotheses for biological mechanisms are quite diverse. It is considered that involvement of noradrenergic and serotoninergic pathways following a stroke is associated with predisposition to depression. It was shown that concentration of serotonin metabolites in the cerebrospinal fluid of patients with PSD was decreased, and it was confirmed that the occurrence of PSD was associated with a decrease in monoamine neurotransmitters. 4 The importance of inflammation regarding the risk of PSD was suggested by numerous studies in recent years. Available data indicate that inflammatory responses are activated centrally and peripherally following an acute stroke and that proinflammatory cytokines initiate the inflammatory response. Dysfunction in the noradrenergic system may occur due to inflammation, causing depression. 5
Moreover, there is evidence that dysfunction of astrocytes, one of the glial cells, is involved in the etiopathogenesis of depression. Various neurotrophic factors, including glial-derived neurotrophic factor, brain-derived neurotrophic factor (BDNF), and fibroblast growth factor 2 (FGF 2), the release of which is regulated by astrocytes, are known to increase synaptic plasticity, regulate nerve function, and support nerve growth. 6 BDNF is a protein that affects neurogenesis and neuroplasticity in the central nervous system, and it is involved in axon and dendrite growth and synaptic plasticity. BDNF is critical for dopaminergic, serotonergic, glutamatergic neuronal transmission, and synaptic formation in cognitive processes, and it is involved in neurogenesis. 7 Recent studies suggested that BDNF was associated with the occurrence of PSD. 8 It was found that the BDNF pathways in the hippocampus of PSD rats were less active. 9 Qiu et al. 10 reported a negative correlation between BDNF levels and depression scores in patients with stroke. Yang et al. 11 suggested that low serum BDNF following a stroke is associated with early-onset PSD. Kim et al. 12 investigated the relationship between BDNF methylation status and PSD, and reported that increased methylation was associated with a higher incidence of PSD and worse symptoms.
In addition to its potential association with PSD, BDNF levels have also been linked to various clinical characteristics of stroke, such as stroke severity, cognitive function, and lesion localization. Previous studies have suggested that lower BDNF levels may correlate with greater neurological deficits and poorer cognitive outcomes in stroke patients.13,14 Furthermore, lesion location—particularly when involving the frontal lobe or left hemisphere—has been associated with both decreased BDNF expression and a higher risk of PSD.15,16
The early-onset PSD mechanisms may be different from late-onset PSD. Thus, it is crucial to identify predictors of early-onset PSD, which is known to affect mortality, morbidity, and functional outcomes. Numerous studies have investigated the potential predictors of early-onset PSD. A study by Geng et al. 17 associated low glutamate levels with early-onset PSD. Uslu et al. 18 investigated the relationship between early-onset PCD development and serum VEGF levels. However, a limited number of studies have investigated the relationship between poststroke serum BDNF levels, occurrence of early-onset PSD, and whether BDNF could serve as a predictor of the severity of PSD. The present study aimed to investigate the relationship between BDNF levels and early depression scores in poststroke patients.
Material and method
Participants and procedure
The study was conducted pursuant to the Declaration of Helsinki, and written informed consents of all participants were collected prior to the commencement of the study. This case-control study was conducted at the Fethi Sekin City Hospital. G*Power 3.1.9.2 program was used to calculate the sample size of the study, and the study titled as “Higher homocysteine and fibrinogen are associated with early-onset poststroke depression in patients with acute ischemic stroke” was taken as reference. The rank-biserial correlation coefficient (r) (effect size) value was calculated as 0.758 using the Z value given in the HAMD-17 comparison provided in above study. The Mann–Whitney U test tab was selected, the effect size was set to 0.758 in the G*Power program, and accordingly it was determined that at least 80 patients in total, including at least 40 participants each in the Non-PSA and PSA groups, should be reached with a 95% confidence interval and 90% power.
Inclusion criteria: Patients over 18 years of age who were diagnosed with acute ischemic stroke by magnetic resonance imaging (MRI) or computed tomography (CT) within 24 hours of hospitalization. Exclusion criteria: Patients with impaired consciousness and dysarthria/aphasia, patients with a history of cognitive disorders such as psychiatric diseases, dementia, other neurological diseases in the pre-stroke period, patients with a history of malignancy, and patients with liver and kidney failure.
Clinical variables, neuroimaging and blood biomarker examination
Since it is crucial to begin rehabilitation as soon as possible, 19 patients were referred to us during the acute rehabilitation phase once hemodynamic and clinical stabilization was attained within 72 hours following a stroke. Sociodemographics and clinical characteristics of patients with ischemic stroke were analyzed. Routine blood tests were conducted in all patients and their systolic/diastolic blood pressures were measured. Blood pressure (systolic/diastolic) was measured within the first 4 hours upon admission. T1-, T2-sequences, and diffusion-weighted imaging were analyzed on MRI scans within 24 hours after admission to determine the location of brain infarction. Infarct localization was recorded either as anterior circulation (anterior cerebral artery, middle cerebral artery) or posterior circulation (posterior cerebral artery, vertebrobasilar artery).
Blood samples of all participants were collected at 08:00-08:30
This ELISA kit uses the Competitive-ELISA principle. The micro ELISA plate provided in this kit has been pre-coated with BDNF. During the reaction, BDNF in the sample or standard competes with a fixed amount of BDNF on the solid phase supporter for sites on the Biotinylated Detection Ab specific to BDNF. Excess conjugate and unbound sample or standard are washed from the plate, and Avidin conjugated to Horseradish Peroxidase (HRP) are added to each microplate well and incubated. Then a TMB substrate solution is added to each well. The enzyme-substrate reaction is terminated by the addition of stop solution and the color change is measured spectrophotometrically at a wavelength of 450 nm ± 2 nm. The concentration of BDNF in the samples is then determined by comparing the OD of the samples to the standard curve.
Functional status, cognitive status, and depression were assessed on the 14th day following stroke diagnosis. The functional status of the patients was assessed by a physical medicine and rehabilitation specialist using the NIHSS scale. Moderate to severe stroke was defined as one with an NIHSS score of ≥5. Cognitive status was assessed by a psychiatrist using the Montreal Cognitive Assessment (MoCA) Test. The occurrence of post-ischemic depression was assessed at Week 2 of stroke based on the Diagnostic and Statistical Manual of Mental Disorders, fifth edition (DSM-5). 20 The severity of depressive symptoms was assessed using the Hamilton Depression Rating Scale (HAM-D17). Patients were assigned to mild, moderate, or severe PSD groups based on the HAMD-17 scores.
Scales used in the study
National institutes of health stroke scale (NIHSS)
NIHSS assesses the functioning in stroke patients and provides an idea about future prognosis. The total NIHSS scores can range from zero to 42. A score of zero indicates normal stroke, 1-4 indicates mild stroke, 5-14 indicates moderate stroke, 15-20 indicates moderate-heavy stroke, and ≥21 indicates severe stroke. 21
Montreal cognitive assessment
MoCA is a rapid screening test aimed to assess mild cognitive impairment. The scale items include executive functions, attention and concentration, memory, language, abstract thought, visual structuring skills, and calculation. The total MoCA scores can range from zero to 30. Twenty one points and above are considered normal. 22
Hamilton depression rating scale (HAM-D17)
HAM-D17 is a 17-item test that inquiries about symptoms of depression experienced in the last 7 days, and it is used to measure the severity of depression. A score of 7-17 points is considered mild depression, where 18-23 points is considered moderate depression, and 24 points and above, severe depression. The validity and reliability of the scale for the Turkish language weas conducted. 23
Statistical analysis
The Statistical Package for the Social Sciences (SPSS Inc., Chicago, IL) software version 22 was used for statistical analyses. Descriptive data were presented in n and % values for categorical data and mean ± standard deviation (Mean ± SD), respectively, and median interquartile range (25-75 percentile values) for continuous data. The Chi-squared analysis (Pearson Chi-square) was used to for intergroup comparison of categoricblal variables. The Kolmogorov–Smirnov test was used to test the normal distribution hypothesis for continuous variables. Student’s t test and Mann–Whitney U test were used for variables with and without normal distribution, respectively, for the comparison of paired groups. The Kruskal–Wallis test was used to compare more than 2 variables. Spearman’s correlation test was used to investigate the relationship between continuous variables. The ROC curves were drawn to measure the value of BDNF in cases of PSD. The Enter method was used to construct the model and accordingly those with a significant relationship in the correlation test were included in the model. A P level of <0.05 was considered statistically significant for all analyses.
Results
Comparison of all parameters by occurrence of depression.
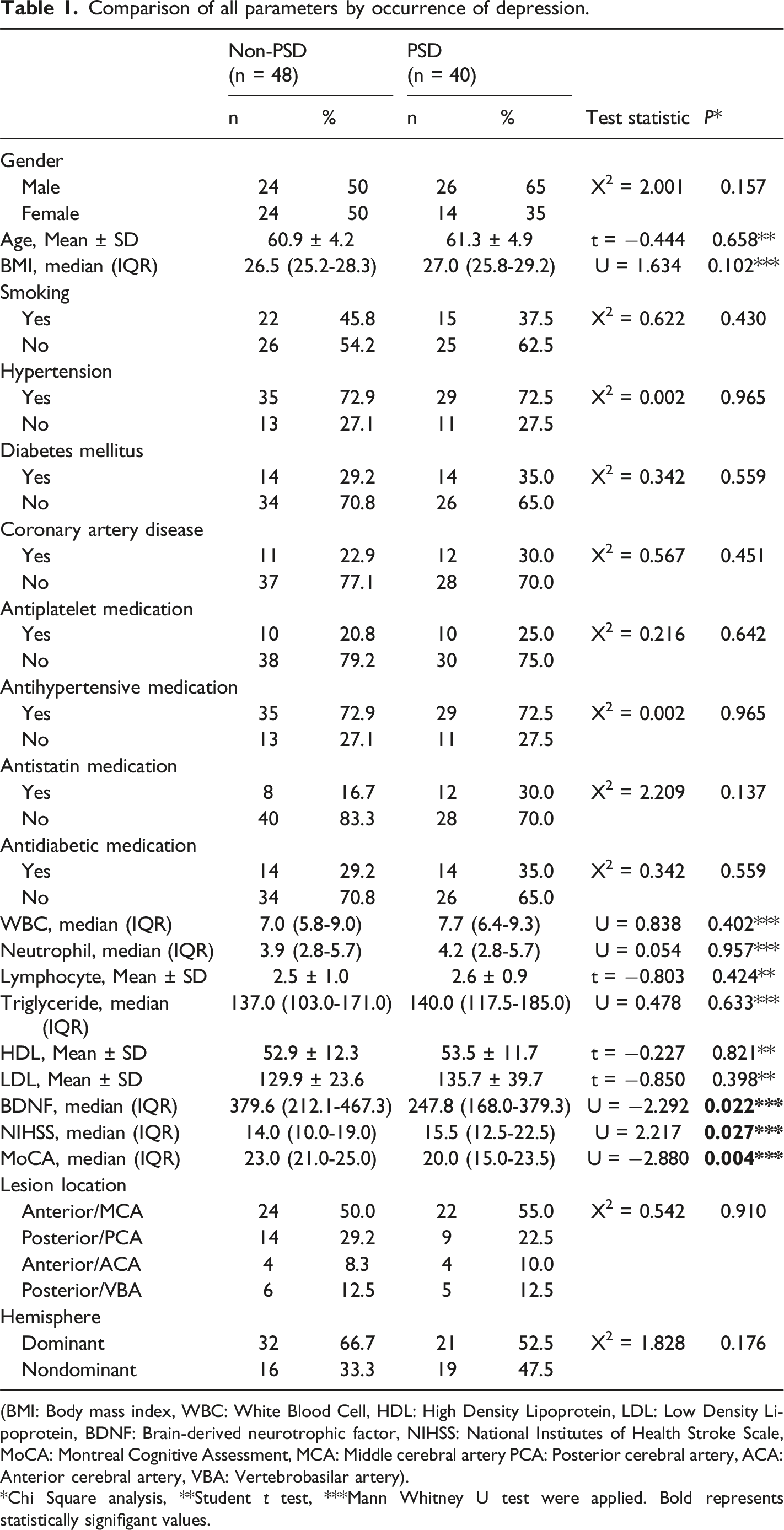
(BMI: Body mass index, WBC: White Blood Cell, HDL: High Density Lipoprotein, LDL: Low Density Lipoprotein, BDNF: Brain-derived neurotrophic factor, NIHSS: National Institutes of Health Stroke Scale, MoCA: Montreal Cognitive Assessment, MCA: Middle cerebral artery PCA: Posterior cerebral artery, ACA: Anterior cerebral artery, VBA: Vertebrobasilar artery).
*Chi Square analysis, **Student t test, ***Mann Whitney U test were applied. Bold represents statistically signifigant values.
Comparison of BDNF, NIHSS, MoCA, and location of lesion in patients with low and moderate/severe depression.
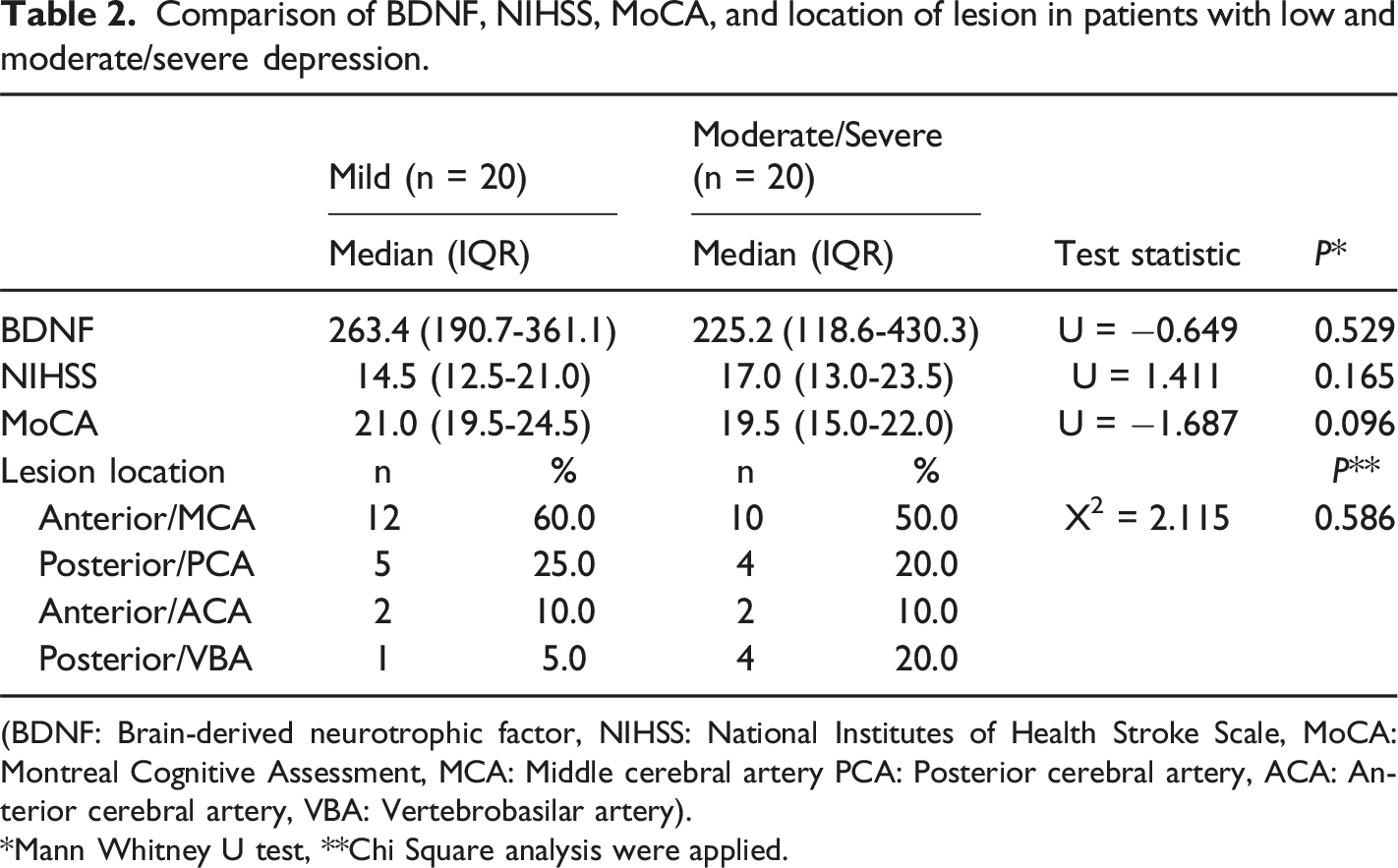
(BDNF: Brain-derived neurotrophic factor, NIHSS: National Institutes of Health Stroke Scale, MoCA: Montreal Cognitive Assessment, MCA: Middle cerebral artery PCA: Posterior cerebral artery, ACA: Anterior cerebral artery, VBA: Vertebrobasilar artery).
*Mann Whitney U test, **Chi Square analysis were applied.
Correlation of BDNF level and HAM-D17 scores with other variables.
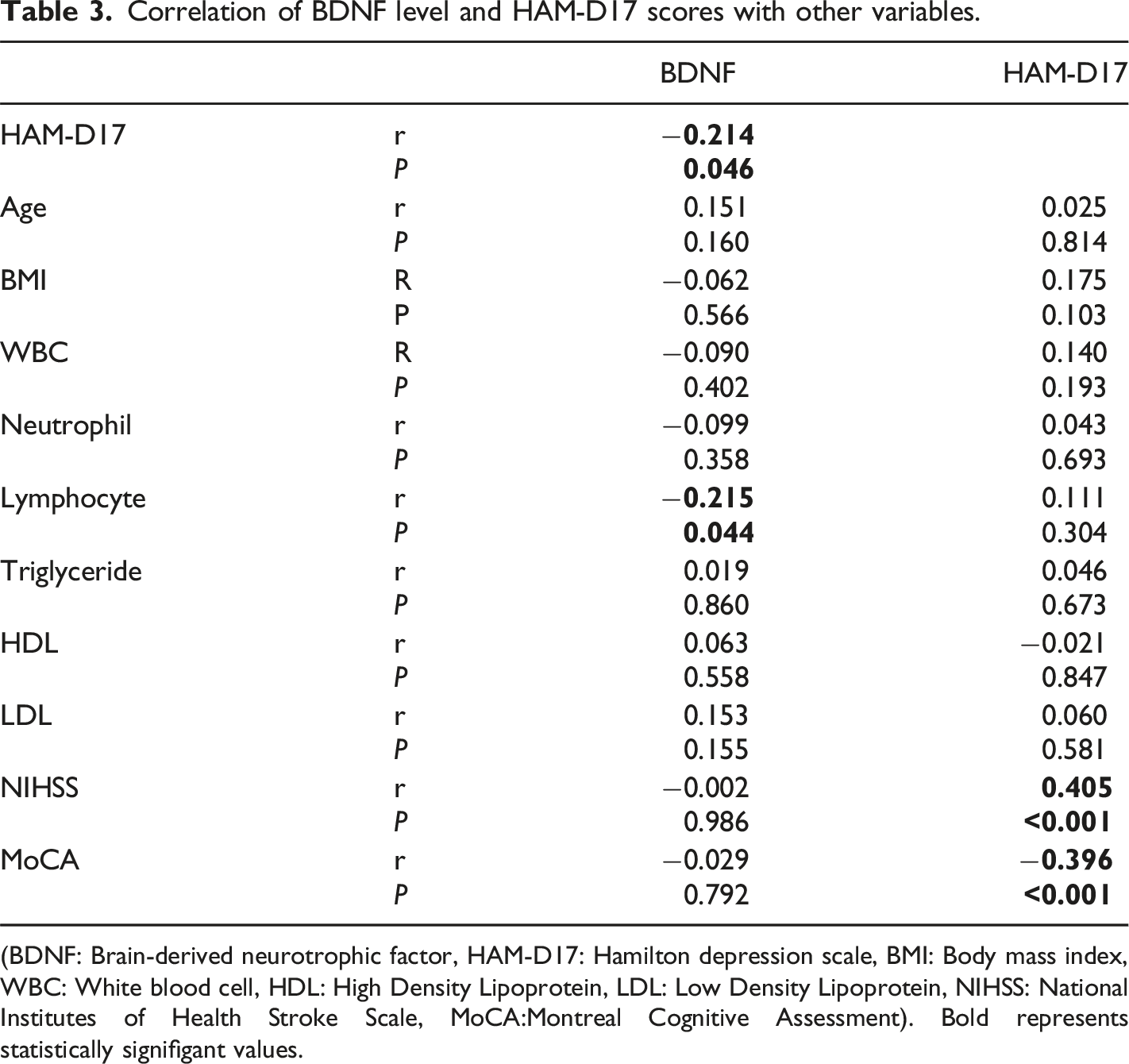
(BDNF: Brain-derived neurotrophic factor, HAM-D17: Hamilton depression scale, BMI: Body mass index, WBC: White blood cell, HDL: High Density Lipoprotein, LDL: Low Density Lipoprotein, NIHSS: National Institutes of Health Stroke Scale, MoCA:Montreal Cognitive Assessment). Bold represents statistically signifigant values.
Receiver operating characteristic (ROC) analysis was used to investigate the extent the BDNF level could predict early-onset PSD and cut-off values were determined. With a BDNF cut-off value of 361.51, the sensitivity and specificity values were 75% and 56.2%, respectively, which indicated that BDNF was a good predictor. The area under the curve (AUC) in the drawn ROC was found to be 0.642 (P < .001). (Figure 1). ROC Curve of BDNF value for the presence of PSD. (ROC: Receiver Operating Characteristic Curve. BDNF: Brain- derived neurotrophic factor. PSD: Poststroke Depression).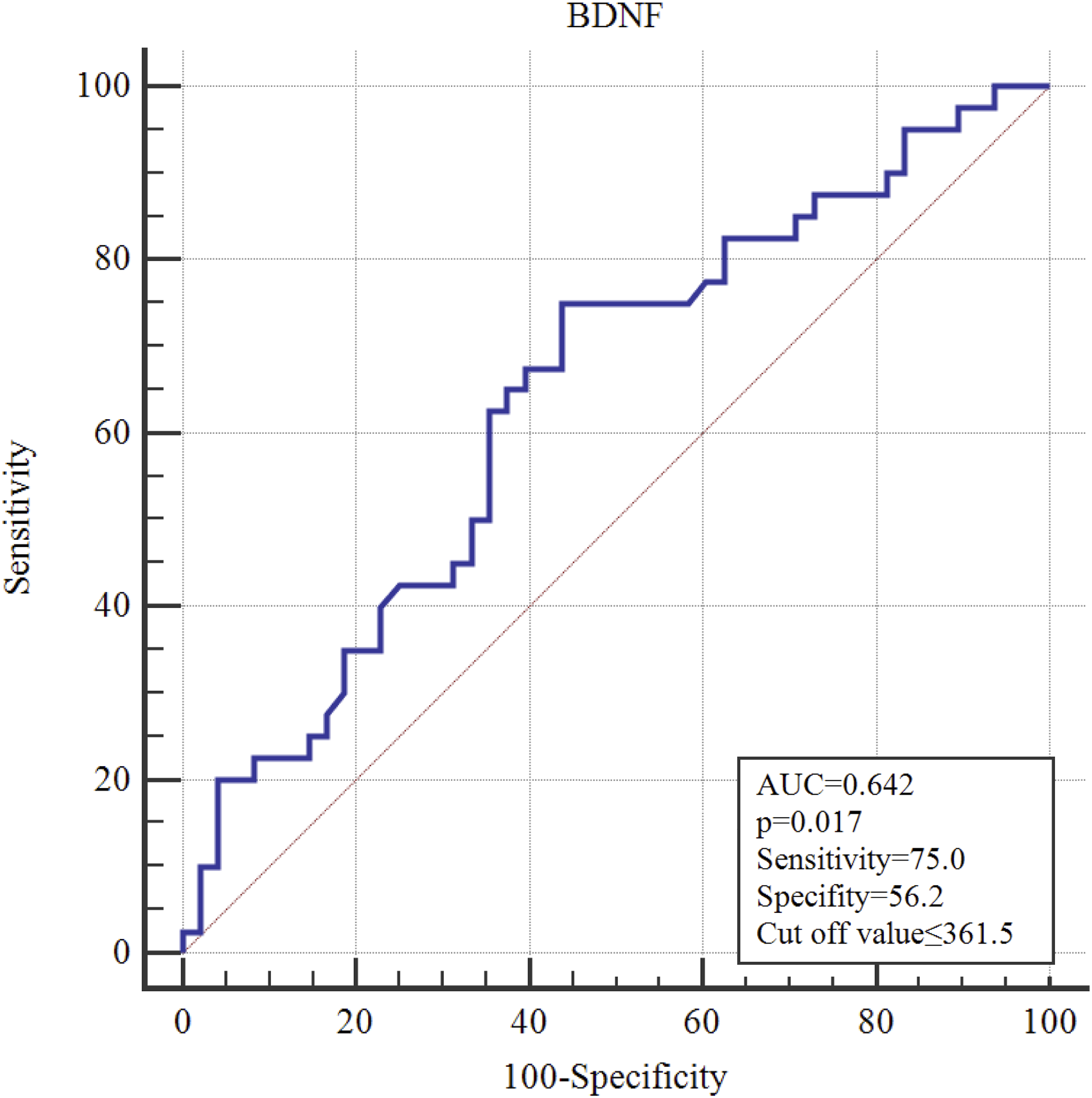
Discussion
This study investigated the relationship between serum BDNF levels and early-onset PSD and the relationship between serum BDNF levels and clinical variables in patients with ischemic stroke. Results reveal that serum BDNF levels were lower in patients with early-onset PSD, but there was no difference in the severity of depression and serum BDNF levels. The severity of disease and rate of disability increased, where cognitive capacity decreased in the early-onset PSD group. These findings indicate that serum BDNF may have potential clinical relevance in the context of early-onset PSD; however, its predictive value remains uncertain due to the cross-sectional nature of the study.
In the present study, 45% of patients with ischemic stroke were diagnosed with early-onset PSD at Week 2 of stroke. Similarly, Chen et al investigated whether acute stroke-induced peripheral immunoinflammatory response was associated with the occurrence of poststroke depression and reported that 47% of 103 stroke patients were diagnosed with early-onset PSD. In the same study, the complete blood parameters of patients with and without a diagnosis of early-onset PSD were similar, except for the monocyte value. 24 Chen et al. associated monocyte count with the risk of early-onset PSD. 24 Another study suggested that higher neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio were associated with PSD at Month 6. 25 It was suggested that dysregulation of peripheral lipids was associated with depression and cognition; thus, medical conditions with chronic lipid dyshomeostasis had early predictive value for the risk of depression and cognitive decline. 26 There was no association between whole blood parameters and blood lipids and early-onset PSD in the present study. Although it was suggested that these values might predict early-onset PSD, 27 these inconsistent results might be related to the duration of depression assessed. Although there was no significant difference by sex between the groups with and without early-onset PSD, the rate of early-onset PSD was higher in men. Women have a more proinflammatory response to stress, and therefore, their mental status is more affected by stressors. It was reported by a study of 786 stroke patients that there was no difference by sex in the initial onset of depression after having a stroke for the first time. 28 This difference may be due to the fact that the present study was designed as cross-sectional research and conducted using a scale based on self-reported symptoms.
It was reported that PSD symptoms were associated with active smoking status. 29 A 2024 study suggested that active smokers had higher levels of depression after a stroke. It was reported that continued active smoking in patients with stroke decreased the quality of life of patients with mild to moderate poststroke sequelae. 30 The results were similar in terms of smoking status between our patients with and without a diagnosis of depression during the early poststroke period. Patients with and without early PSD had similar rates of comorbidities (hypertension, diabetes, etc.) It is well-established that systemic diseases increase the risk of depression by increasing inflammation as well as impairing the functionality and decreasing the quality of life. 31 Particular results of the present study might be associated with the fact that our patients were evaluated at Week 2 of stroke. Long-term evaluation of patients can help better understand this situation. It was reported that the location of the lesion in the left hemisphere, especially in the cerebral cortex and anterior region, was associated with a higher likelihood of PSD. 32 It was suggested that different lesions may affect PSD symptoms in stroke patients. 33 There was no association between location of lesion and depression among the patients included in the present study. This may be due to the evaluation of stroke patients at Week 2 of stroke. Determining the likelihood of PSD development based on the location of lesion may inform the psychosocial interventions for patients from the first hours of stroke.
Patients diagnosed with depression during the early poststroke period had higher levels of disability, lower cognitive functions and lower serum BDNF levels compared to patients without early PSD. Lower BDNF levels were associated with poor prognostic functional outcome in stroke patients. 34 It was reported that Serum BDNF levels, which were considered important for cognitive functions, were lower in patients with PSD compared to those without depression, and it was suggested that antidepressants might increase BDNF expression in the brain and mitigate symptoms of depression. 35 Another study with stroke patients reported that serum BDNF levels of PSD patients were significantly lower on Day 1 compared to patients without PSD, but there was no significant difference between patients with and without PSD on Day 7, and lower BDNF levels on Day 1 after stroke were significantly associated with increased risk of PSD. 11 In a metanalysis of 268 stroke patients with PSD and 425 stroke patients without PSD, the serum BDNF levels decreased in patients with PSD, and it was suggested that BDNF level could be used as a potential biomarker to predict the risk of PSD among stroke patients. 36 Nevertheless, a study of patients with acute ischemic stroke reported that serum BDNF levels did not differ between Day 7 and Month 6 after stroke in patients with and without PSD. 37 Li et al investigated 295 patients with ischemic stroke and reported that serum BDNF levels were lower in PSD patients compared to non-PSD patients. Similar to the present study, it was reported that serum BDNF levels were negatively correlated with NIHSS scores and low serum BDNF levels were associated with increased severity of stroke. 38 Upon a review of previous studies, it can be suggested that there is a relationship between changes in serum BDNF levels and PSD. Nevertheless, there is an ongoing debate on whether serum BDNF levels measured in the early stage of stroke can be used to predict the risk of subsequent PSD. 39 The results of the present study are consistent with most of the previous studies. Early diagnosis of early-onset PSD is important for it increases morbidity and that patient’s cooperation is important during physical therapy and rehabilitation phase after stroke. Therefore, low serum BDNF levels in early blood samples collected from patients after ischemic stroke may predict the diagnosis of early PSD.
In the present study, there was no significant difference between serum BDNF levels and gender, smoking status, comorbidities, medication use, location of lesion, and hemisphere by BDNF levels. Tuwar et al. suggested that higher BDNF levels were associated with blood pressure, HbA1c, white blood cells, and higher creatinine levels in acute ischemic stroke. 40 It was reported that there was no relationship between infarct volume and serum BDNF level in stroke patients. 41 Another study reported that serum BDNF levels in stroke patients were independent of individual variables, including sex and smoking status. 42 Previous studies, which investigated the relationship between serum BDNF level and severity of disease and clinical variables reported contradictory results, and therefore, there is a need for further studies with larger sample groups.
Havlosvka et al suggested that hemodynamic subtype and 1-day BDNF level can predict the risk of cognitive impairment in the acute period of ischemic stroke. 43 Upon ROC analysis in terms of early-onset depression after ischemic stroke, the sensitivity and specificity levels were 75% and 56.2%, respectively, with a BDNF cut-off value of 361.51, indicating acceptable predicting qualities for BDNF. Furthermore, the BDNF level predicted the HAM-D17 score. This suggested that serum BDNF level might serve as a parameter for use in addition to psychiatric scales in early-onset PSD.
The limitations of the study include the lack of a control group of healthy people with clinical characteristics along with the patient group, the relatively small sample group, and the fact that the study was performed in a single center. The lack of a healthy control group limits the contextual understanding of BDNF levels in this population. Additionaly, the cross-sectional design prevents any inference of temporality or causality between low BDNF levels and PSD.
In conclusion, there is a need for longitudinal studies with larger sample sizes to further elucidate whether serum BDNF levels could serve as appropriate markers for recognizing early-onset PSD and to determine the severity of depression in stroke patients. Recognizing the risk of developing early-onset PSD in the early stages of stroke and providing patients with the necessary psychosocial support can help patients benefit better from physical therapy and rehabilitation and to improve their quality of life. The results may also suggest that early-onset PSD may be treated with drugs that affect BDNF levels. To the best of our knowledge, the present study is the first study to investigate the BDNF levels in patients with early-onset PSD. We believe that our results will provide insights for further studies in this field.
Footnotes
Acknowledgements
We would like to thank Bilal YILDIZ, a neurology specialist working at Fethi Sekin City Hospital, for consulting stroke patients to us.
Author contributions
Conceptualization, Sevler Yildiz and Emine Yıldırım Uslu; methodology, Sevler Yildiz and Sevler Yildiz; software, Sevda Korkmaz and Emine Yıldırım Uslu; validation, Sevda Korkmaz, Sevler Yildiz; formal analysis, Sevler Yildiz; investigation, Sevda Korkmaz and Emine Yıldırım Uslu; resources, Emine Yıldırım Uslu, Sevler Yildiz and Sevda Korkmaz; data curation, Sevda Korkmaz; writing— original draft preparation, Emine Yıldırım Uslu and Sevler Yildiz; writing—review and editing, Sevda Korkmaz, Emine Yıldırım Uslu, Sevler Yildiz; visualization, Sevler Yildiz; supervision, Emine Yıldırım Uslu; project administration, Sevda Korkmaz; funding acquisition, Emine Yıldırım Uslu and Sevler Yildiz All authors have read and agreed to the published version of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data Availability Statement
The original contributions presented in this study are included in the article. Further inquiries can be directed to the corresponding author. The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.