
Abstract
Objective
Individuals living with HIV are at increased risk for psychiatric disorders. In this pilot randomized clinical trial, the effects of probiotics on improving psychiatric symptoms among patients living with HIV was examined.
Methods
A total of 50 patients living with HIV were randomly assigned to one of two groups: one group received a probiotic capsule. In contrast, the other received a placebo for 12 weeks, determined by a simple randomization method. Patients were evaluated at weeks 0, 4, 8, and 12 using the Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), Simplified Nutritional Appetite Questionnaire (SNAQ), and the Pittsburgh Sleep Quality Index (PSQI).
Results
Compared to the control group, HIV patients in the intervention group receiving probiotics exhibited a significantly greater reduction in anxiety symptoms and greater improvement in appetite compared to those in the placebo group (time*group interaction: F (3, 144) = 6.63, P < 0.001 for anxiety symptoms; F (3, 144) = 18.74, P < 0.001 for appetite).
Conclusions
Probiotics may be beneficial in alleviating anxiety symptoms and anorexia in persons living with HIV. Future studies in multicenter settings with larger sample sizes and extended follow-up periods are needed to replicate these results.
Introduction
Human immunodeficiency virus (HIV) infection has evolved into a chronic and manageable condition, becoming a significant global public health issue over the past 40 years. This epidemic has led to approximately 40 million deaths worldwide. 1 Although antiretroviral therapy (ART) has proven effective, lifelong treatment is required, and there is currently no cure. 2 Implementing a stigma-free, patient-centered care model can improve long-term outcomes by removing barriers to access at the community, health system, clinic, and individual levels. 3 Evidence-based interventions for the prevention and care of HIV can lead to reduced mortality rates, fewer new diagnoses, and significant economic benefits. 4
In Iran, around 60 000 individuals are living with HIV, with more than a third being aware of their HIV status. Among those aware, about two-thirds are receiving ART. 5 Studies indicate that the quality of life for patients living with HIV/AIDS in Iran is significantly low. 6 Drug use negatively impacts this quality of life. 7
Recent research has identified six common mental health issues among people living with HIV: depression, anxiety, suicidal ideation, post-traumatic stress disorder (PTSD), stigma, and psychological distress. The pooled prevalence rates for these conditions are 31%, 29%, 20%, 20%, 47%, and 44%, respectively. 8 Additionally, another study reported that the global prevalence of depressive symptoms over the past 5 years is 35%. These symptoms can vary based on factors such as geographic location, gender, assessment tools used, alcohol consumption, smoking, marital status, comorbidities, financial situation, and education level. 9 Anxiety disorders among individuals living with HIV/AIDS can hinder personal development and are linked to a range of negative mental, physical, and psychosocial outcomes, resulting in a diminished quality of life. However, addressing anxiety can help reverse some of the physical damage it causes. 10
Insomnia is another common comorbidity in individuals living with HIV/AIDS and is associated with lower health-related quality of life, an increase in depressive symptoms, and poorer medication adherence. 11 Moreover, HIV infection can lead to both anorexia and malnutrition, which are linked to decreased immune function. 12
The gut-microbiota-brain axis connects gut microbes with brain communication, and gut dysbiosis has been observed in various neuropsychiatric disorders.13,14 Probiotics play a crucial role in maintaining the balance in the gastrointestinal tract and ensuring proper gut-brain axis function. This connection influences how gut health affects the emotional and cognitive centers of the brain. Using probiotics may significantly contribute to this balance and overall gut function. 15
The use of probiotics to manage dysbiosis and gut-mucosal immune disorders is one of the proposed interventions in addressing chronic immune activation in the pathogenesis of HIV infection. Probiotics have been linked to reduced immune system activation and may help limit several related disorders. 16 In recent years, probiotics have gained attention as a potential therapeutic intervention for psychiatric disorders due to their role as modulators of the gut-brain axis. Improvements in immune and inflammatory profiles—such as reductions in C-reactive protein (CRP) and Interleukin 6 (IL-6)—have been suggested as possible mechanisms underlying this therapeutic response. 17
In a double-blind clinical trial, the probiotic Lactobacillus plantarum was associated with a significant reduction in Beck Depression Inventory scores and an improvement in sleep quality, especially during the deep sleep stage. 18 Furthermore, another randomized clinical trial found that administering the probiotic Lactobacillus acidophilus resulted in enhanced sleep quality, increased appetite, and a rise in body mass index among patients with chronic methamphetamine use. 19
Some studies suggest that using probiotics for more than 30 consecutive days can reduce the incidence of diarrhea in patients living with HIV/AIDS. However, probiotics do not appear to affect CD4 cell counts in these individuals. 20 Other research has indicated that probiotic supplementation may lead to a moderate increase in CD4 lymphocyte counts. 21
Based on the evidence presented and considering the safety of probiotic supplements for patients living with HIV/AIDS, we conducted a pilot triple-blind randomized clinical trial. We aimed to determine whether the use of these probiotics could lead to improvements in psychiatric symptoms, insomnia, and anorexia in patients living with HIV/AIDS.
Materials and Methods
This study is a 12-week randomized controlled trial aimed at investigating the effects of probiotic supplementation on symptoms of depression, anxiety, insomnia, and anorexia in patients with HIV. The research was conducted from May 2022 to May 2023 at the Counseling Center for Behavioral Disorders at the Alborz University of Medical Sciences in Iran.
Participants
The participants in this pilot study were Iranian outpatients with Human Immunodeficiency Virus (HIV) who were referred to the Counseling Center for Behavioral Disorders at the Alborz University of Medical Sciences. They received free medical care related to their HIV condition and had regular outpatient visits with an infectious disease specialist, who is a faculty member at the university. Antiretroviral treatment was not initiated for the participants during the study. Individuals were excluded from the study if there was a need to start antiretroviral therapy or if a participant’s CD4 count fell below 350; however, they were still evaluated in the final analysis.
The inclusion criteria for the study required participants to have received at least six months of medical care related to HIV at this center.
Additionally, participants must not have had a known psychiatric disorder requiring current treatment, as determined by a clinical interview conducted according to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) criteria, assessed by two independent psychiatrists who are faculty members at the Alborz University of Medical Sciences.
Furthermore, participants needed to be over 18 years old, have an IQ above 70, not have received electroconvulsive therapy (ECT) in the last two weeks, and not have consumed alcohol or other substances in the 3 months before entering the study. A CD4 cell count level above 350 was also required, along with the provision of written informed consent for voluntary participation in the study.
Other initial selection criteria for patients to participate in the study included not having specific neurological or organ diseases, cardiovascular diseases, or a history of brain or cardiovascular surgery.
Patients who exhibited any of the following conditions were discontinued from the clinical trial interventions but were not excluded from the statistical analysis of study participants: 1. Unwillingness to participate in the study. 2. Failure to attend follow-up assessments to evaluate the results of the intervention. 3. Inability to use the provided treatment for more than 3 consecutive days. 4. Occurrence of psychiatric disorders requiring hospitalization or other therapeutic interventions, including the need for antiretroviral drugs. 5. Use of psychotropic medications on an outpatient basis during the study. 6. Allergic reactions to probiotics. 7. Use of antibiotics or probiotics within 3 weeks prior to enrollment. 8. Unwillingness to continue participating in the study. 9. Pregnancy or breastfeeding.
It is important to note that non-dependent use of nicotine and caffeine was not considered an exclusion criterion.
Measures
Beck Anxiety Inventory (BAI)
BAI is a 21-item self-report instrument designed to assess the severity of anxiety. 22 Participants are asked to rate the intensity of their annoyance from common anxiety symptoms experienced in the past week using a 4-point scale. The questionnaire demonstrates high internal consistency (alpha = 0.92) and strong test-retest reliability over one week (r(81) = 0.75). 23 The psychometric properties of the Persian version of BAI have also been evaluated, showing good reliability (r = 0.72, P < 0.001), very good validity (r = 0.83, P < 0.001), and excellent internal consistency (alpha = 0.92). 24
Beck Depression Inventory (BDI)
The Beck Depression Inventory is a widely used tool for assessing the severity of depression in adults. Its validity and reliability have been confirmed in various studies across different cultural groups. 25 This inventory consists of 21 self-report items designed for clinical and educational. 26 Toosi et al evaluated the psychometric properties of the Beck Depression Inventory among high school students by measuring concurrent validity and conducting factor analysis. They reported reliability and correlation coefficients of 0.55 and 0.83, respectively, using test-retest methods and Cronbach’s alpha. 27 Similarly, Ahmadi et al 28 demonstrated that this inventory has acceptable psychometric properties for screening depression among Iranian patients with coronary heart disease, reporting an internal consistency of 0.90 based on Cronbach’s alpha.
Simplified Nutritional Appetite Questionnaire (SNAQ)
This questionnaire is a straightforward tool designed to assess appetite and predict weight loss. 29 The total score for this questionnaire ranges from 4 to 20. In many studies, a score of 14 or lower is considered an indicator of malnutrition and involuntary weight loss. 30 The reliability and validity of the Persian version of this questionnaire have been evaluated. The internal consistency was confirmed with a Cronbach’s alpha coefficient of 0.7. Additionally, the test-retest reliability exhibited consistency with a Pearson correlation of 0.85, measured over a 2-week interval. 31
The Pittsburgh Sleep Quality Index (PSQI)
The Pittsburgh Sleep Quality Index (PSQI) is used to evaluate sleep quality and disturbances through a self-reported and retrospective approach covering the previous month. 32 The questionnaire consists of seven components: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleeping medication, and daytime dysfunction, with a total of 19 individual items. Each item is rated on a 4-point Likert scale, ranging from 0 to 3. 33 The reliability and validity of the Persian version of this questionnaire have been assessed. In a study involving psychiatric patients as well as a control group, Cronbach’s alpha coefficients were found to be 0.77 for all subjects, 0.52 for the patient group, and 0.78 for the control group. Additionally, at a cutoff point of 5, the sensitivity and specificity were reported as 94% and 72%, respectively. 34
Procedures
Outcome
The primary aim of this study was to compare the effect of probiotics versus placebo on reducing depression and anxiety symptoms and improving sleep quality and appetite among patients with HIV. Patients receiving outpatient care at the Alborz University Medical Sciences Counseling Center for Behavioral Disorders were included in the study if they met the inclusion criteriaand did not meet the exclusion criteria.
Target patients underwent a diagnostic interview conducted by two independent psychiatrists, using DSM-5 criteria. If no psychiatric disorders requiring therapeutic interventions were identified, the patients were evaluated using the Beck Anxiety Inventory (BAI), Beck Depression Inventory (BDI), Simplified Nutritional Appetite Questionnaire (SNAQ), and Pittsburgh Sleep Quality Index (PSQI). Study participants were then re-evaluated using the same questionnaires at the fourth, eighth, and 12th weeks of the study. Various outcome measures were considered to assess the potential effects of probiotics on the psychiatric symptoms of patients with HIV.
Adverse events related to probiotic use were monitored using a 25-item checklist at regular intervals (weeks 4, 8, and 12).35,36
Additionally, participants were encouraged to report any other possible side effects in an open-ended question at the end of the questionnaire. They also had access to a 24-hour hotline to report any complications experienced at any time and receive the necessary advice.
Intervention
Using simple randomization, patients were assigned to one of two parallel groups to receive either probiotic capsules containing Lactobacillus acidophilus, Bifidobacterium, and Lactobacillus plantarum (108 colony-forming units (CFUs), Takgene Zist Co., Tehran, Iran) or placebo capsules that matched in shape, color, and dosage frequency. The treatment duration was 12 weeks, with administration twice a day. To ensure a triple-blind methodology, 37 neither the patients, researchers, nor those analyzing the results were aware of the capsule contents. By the end of the 12th week, no patients were receiving any other medications.
Randomization, Allocation Concealment, and Blinding
Upon screening patients for eligibility and obtaining written informed consent, participants were randomly assigned to either the intervention or control (placebo) group using a block randomization method with unequal block sizes of 2, 4, and 6. A randomization list was generated using the web software available at https://www.sealedenvelope.com/simple-randomiser/v1/lists. 38 To maintain allocation concealment, the sequence was hidden by selecting non-identical blocks. Each patient’s specific group assignment was placed in sealed envelopes corresponding to the order of the randomization sequence and each patient’s identification number. When a patient was identified, one of these envelopes would be opened to determine their assignment.
Capsules of both groups were packaged in numbered containers to ensure that they were indistinguishable in shape, color, and size. All of these procedures were conducted by an individual who was not involved in the study. None of the psychiatrists, the infectious disease specialist, or the patients had any knowledge of the contents of the packages.
Ethical Considerations and Registration
This study adhered to the principles outlined in the Declaration of Helsinki and its appendices throughout the research process. The ethical review board of the Alborz University of Medical Sciences approved the study protocol under the reference number IR.ABZUMS.REC.1402.013, and registration ID number IRCT20190316043072N3 was obtained from the Iranian Registry of Clinical Trials (as of May 31, 2023).
Participants provided written informed consent before taking part in the study, which was entirely voluntary. They retained the right to withdraw from the study at any time without providing a reason, and they incurred no costs for participation.
Sample Size
As no similar studies were available, this research is considered a pilot study involving 50 participants.
Statistical Analysis
Continuous variables were summarized as mean (standard deviation [SD]) or median (interquartile range [IQR]), depending on appropriateness. Categorical variables were presented as percentages and frequencies. To compare continuous variables between groups, we used either a t-test or the Mann-Whitney test, while categorical variables were analyzed using Fisher’s exact test. Primary outcomes were measured at four-time points: t1 (Baseline), t2 (Week 4), t3 (Week 8), and t4 (Week 12). The differences in these outcomes across groups were evaluated using a two-way mixed analysis of variance (ANOVA), which included the intervention group, time, and the interaction between group and time.
For the dependent variables, we checked all four assumptions necessary for a two-way mixed ANOVA: independence of observations, homogeneity of variance, normality, and sphericity. When the assumptions of normality (based on the examination of studentized residuals) or homogeneity of variances (assessed using Levene’s test) were violated, we performed log transformation to meet these assumptions.
The results are presented in their natural values to facilitate interpretation. Additionally, if our data did not meet the assumption of sphericity, we reported a Greenhouse–Geisser corrected P-value. We utilized Kolmogorov-Smirnov tests to assess the normality of the data. All statistical tests were two-tailed, and with Bonferroni correction applied a P-value of less than <0.0125 was considered statistically significant. All analyses were conducted using SPSS version 25.
Results
In this study, 60 patients underwent primary screening, but 10 were excluded because they did not meet all the inclusion criteria or chose not to participate. Ultimately, 50 patients remained in the study, with 25 receiving probiotics and 25 receiving a placebo. All participants completed the survey until the end of all stages (see CONSORT flowchart in Figure 1). Flow diagram of the clinical trial of the efficacy of probiotics on Depression, Anxiety, Insomnia, and Anorexia in Patients with HIV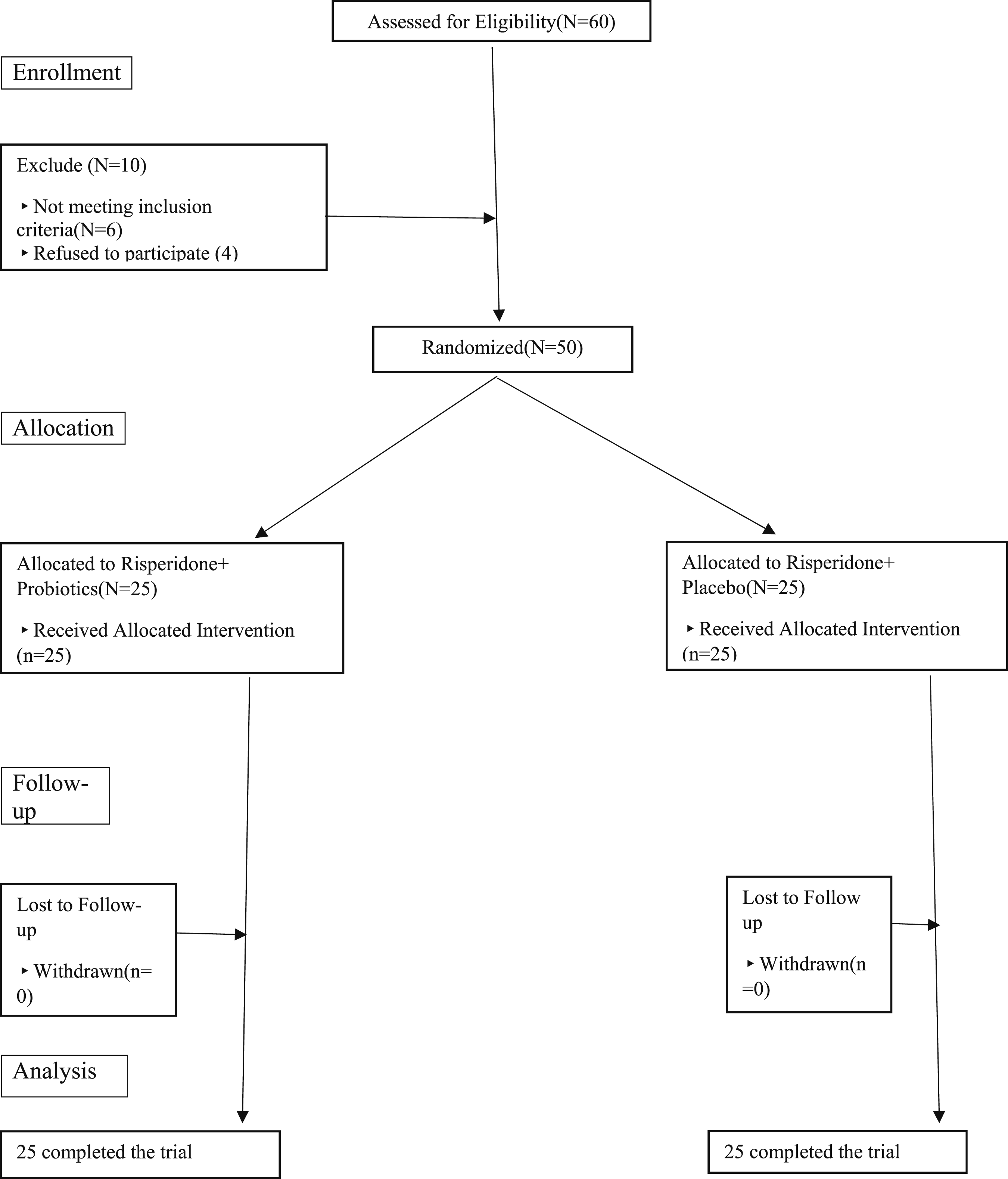
Background and Demographic Characteristics of Patients in the Intervention and Control Groups at Baseline
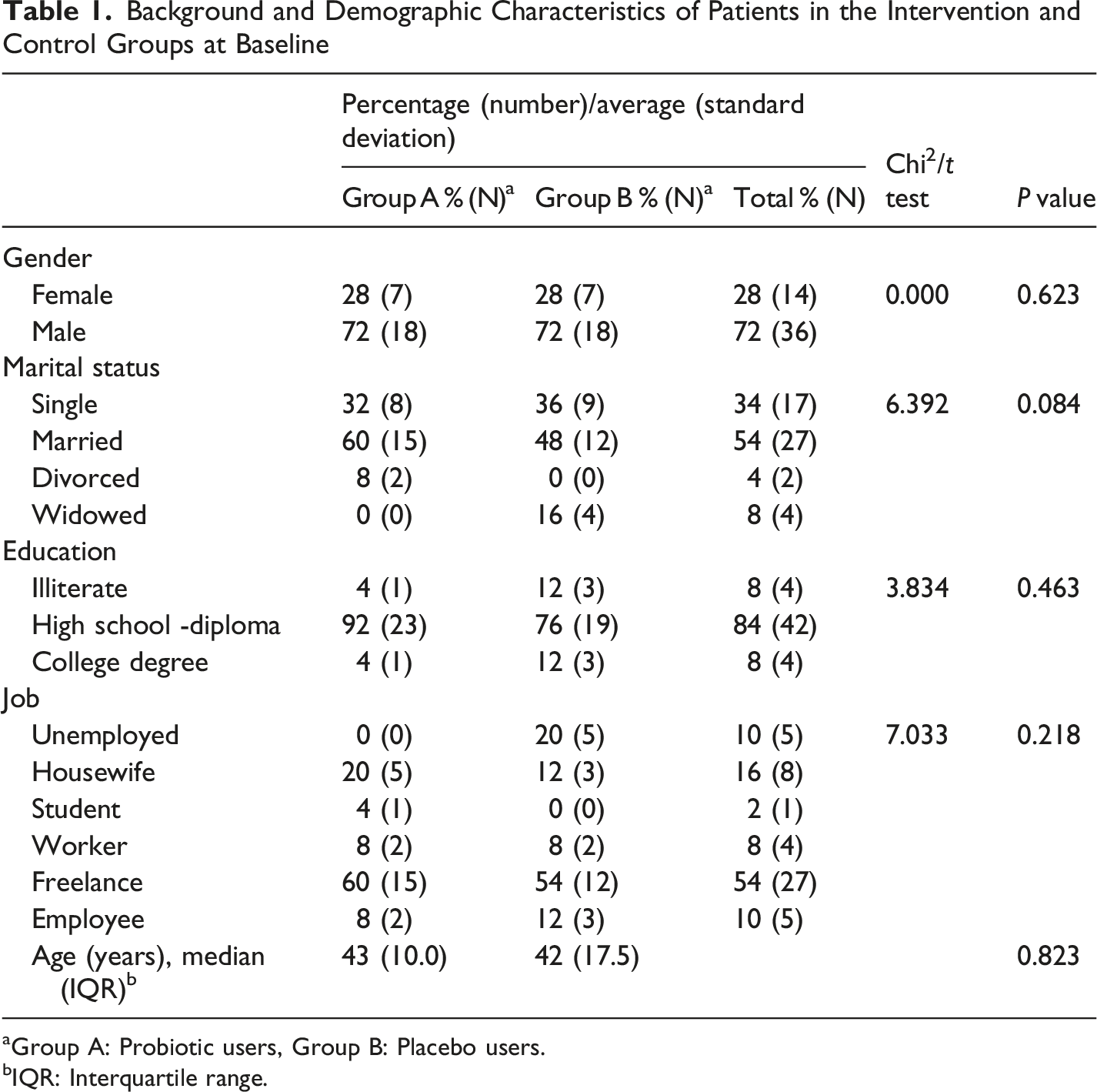
aGroup A: Probiotic users, Group B: Placebo users.
bIQR: Interquartile range.
Temporal Changes in Variables During Follow-Up (Results From Linear Mixed Effects Models)
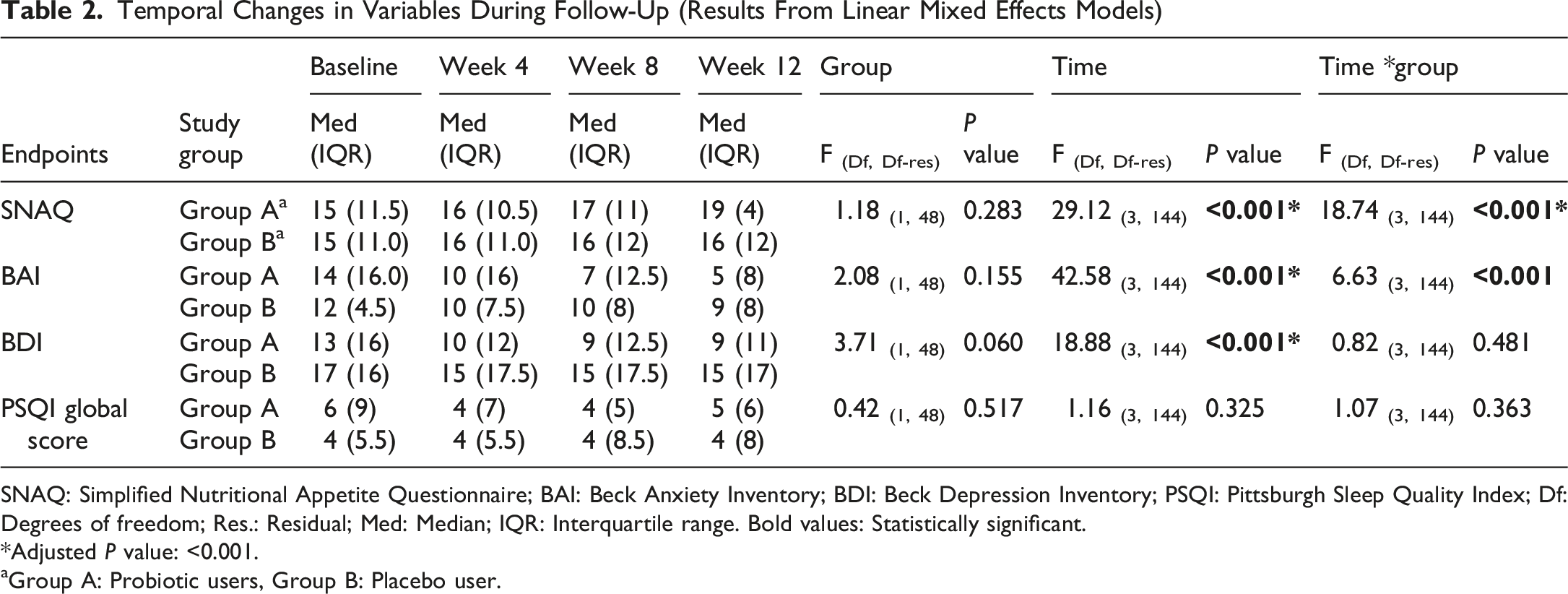
SNAQ: Simplified Nutritional Appetite Questionnaire; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; PSQI: Pittsburgh Sleep Quality Index; Df: Degrees of freedom; Res.: Residual; Med: Median; IQR: Interquartile range. Bold values: Statistically significant.
*Adjusted P value: <0.001.
aGroup A: Probiotic users, Group B: Placebo user.
Regarding adverse events, two cases of diarrhea and two cases of flatulence were reported among patients receiving probiotics, while two instances of flatulence were noted among patients receiving a placebo. These complications were self-limiting in both groups and improved gradually during the study without the need for medical intervention or discontinuation of treatment, typically within a few days (Figure 2). Changes in mean (A) Simplified Nutritional Appetite Questionnaire (SNAQ), (B) Beck Anxiety Inventory (BAI), (C) Beck Depression Inventory (BDI), and (D)The Pittsburgh Sleep Quality Index (PSQI) between endpoint (t4) and baseline (t1) in two groups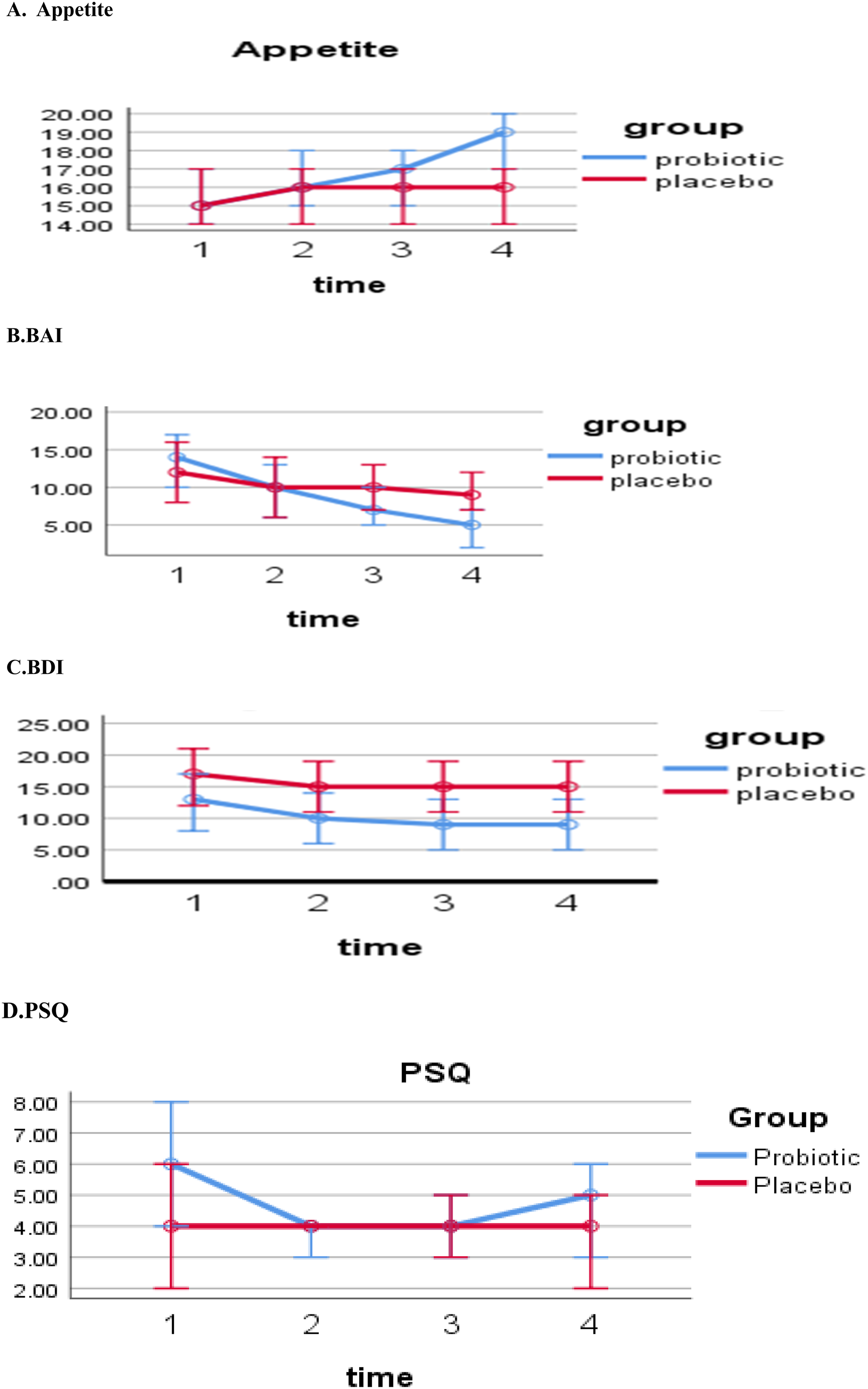
Discussion
In this study, we initially hypothesized that probiotics could be beneficial in alleviating symptoms of depression, anxiety, insomnia, and anorexia in patients living with HIV. The results indicated that probiotics did help improve symptoms of anxiety and anorexia. To the best of our knowledge, this is the first placebo-controlled pilot clinical trial to assess the effectiveness of probiotic supplements for enhancing psychiatric symptoms in individuals living with HIV.
The positive results from testing this hypothesis were consistent with those from UC San Diego’s HIV Neurobehavioral Research Program, which studied 94 adults living with HIV compared to 35 adults who were HIV-negative and reported that gut microbiome dysbiosis was associated with emotional well-being. 39 The study found a significantly higher relative abundance of aerotolerant bacteria in patients living with HIV, which was linked to poorer psychological well-being, less social satisfaction, and more negative emotional states in these individuals.
A review study of clinical trials examining the recent literature from the last decade (2014-2023) on the effects of probiotics on anxiety and depression symptoms found that most studies reported benefits from their use. 40 One longitudinal, non-randomized, single-arm pilot study involved patients living with HIV who met the eligibility criteria of having an HIV-RNA level below 50 copies/ml and CD4 counts above 400 cells/mm, which closely aligns with the inclusion criteria of our study. In this study, the administration of a high-concentration, lyophilized multi-strain probiotic supplement twice daily for six months was associated with improved anxiety levels. This improvement was measured using the State-Trait Anxiety Inventory Y-2 (STAY Y-2). 41 The reduction in anxiety symptoms observed in our study aligns with the findings of the previous research, underscoring the potential of probiotics to alleviate anxiety in patients living with HIV/AIDS.
Our study did not show a decrease in the BDI depression score. Previous research has produced mixed results regarding the effectiveness of probiotics in alleviating symptoms of depression.
For example, a study exploring the impact of Lactobacillus plantarum PS128 on patients with moderate depression found no significant effects after 8 weeks of treatment. 42 Differences in the severity of depressive symptoms and the specific types of probiotics used have been suggested as possible reasons for these varying outcomes.
Additionally, our investigation focused on improving depressive symptoms in individuals living with HIV who did not initially exhibit signs of depressive disorder. Conducting the study with a larger group of individuals living with HIV/AIDS, or those who presented with depressive symptoms at the beginning of the trial, could lead to more comprehensive conclusions in this area. These observations regarding the effectiveness of probiotics in patients living with HIV/AIDS may also apply to issues related to insomnia within this population.
Our study found that probiotics have a positive impact on improving anorexia in patients living with HIV. These findings are consistent with a similar study conducted in Tanzania, which involved over 160 patients with HIV/AIDS. That study reported that probiotics enhanced daily nutrient requirements, specifically for vitamin A, several B complex vitamins, and calcium. 43 Additionally, the effect of probiotics on anorexia corresponds with the results of another study we conducted, in which we examined their impact on anorexia in patients using amphetamines and methamphetamines. 19 Similar to those findings, we observed positive outcomes in this research involving patients living with HIV as well.
This study had several limitations. Due to the limited resources available to our research team, we were unable to assess the composition, density, and diversity of the gut microbiota among participants before and after our intervention. The study lasted 12 weeks, during which participants took a probiotic dosage of 108 CFUs twice a day. This duration and dosage may not have been sufficient to significantly impact the gut microbiota.
Furthermore, the length of the study may not have been adequate to improve symptoms of depression and insomnia in patients living with HIV/AIDS. Additionally, our analysis did not account for variations in factors such as diet and physical activity, which can influence the interactions among probiotics, gut microbiota, and psychiatric symptoms. The criterion for initiating ART in patients participating in this study (assuming the patient’s willingness to receive treatment) was based on CD4 count, independent of the original study design. Constraints related to resources—specifically, the availability of necessary personnel and financial resources for providing medications to individuals living with HIV—were key factors influencing this approach.
Conclusions
Given the chronic nature of HIV infection, it is essential to address and treat psychiatric symptoms, especially in the early stages of the disease. This study has demonstrated that probiotics can help reduce anxiety symptoms and anorexia in individuals living with HIV. However, research on the effectiveness of probiotics for managing psychiatric symptoms in these patients is limited. Therefore, it is recommended to conduct follow-up studies in multicenter settings with larger sample sizes and longer follow-up periods to reach more definitive conclusions in this field.
Footnotes
Acknowledgment
We would like to express our gratitude to the patients who participated in this study. We also appreciate the staff at the Alborz University of Medical Sciences Counseling Center for Behavioral Disorders for their collaboration in conducting the research. Additionally, we extend our special thanks to Takgene Zist Co. in Tehran, Iran, for their generous support in providing the probiotic supplements needed for the study.
Ethical Considerations
The provisions of the Declaration of Helsinki and its appendices were observed at all stages of this study’s implementation. The study protocol was approved by the Alborz University of Medical Sciences research ethics committee with the number of IR.ABZUMS.REC.1402.013 and the registration ID number IRCT20190316043072N3 were taken from the Iranian Registry of Clinical Trials (as of May 31, 2023).
Consent to Participate
Participants completed written informed consent forms before participating in the study, and their participation in the study was completely voluntary. They had the right to withdraw from the study at any time without giving a reason, and they did not incur any fees for participating in the study.
Author Contributions
Conceptualization: Atefeh Zandifar, Rahim Badrfam, Amirhossein Hajaligol, Tyler Kjorvestad, Mojtaba Kaveh, Mahya Beikmohammadi, Seyed Shahab-aldin Vakili, Zohreh Khodaii, Ali Reza Soleimani.
Data curation: Atefeh Zandifar, Rahim Badrfam, Amirhossein Hajaligol, Mojtaba Kaveh, Mahya Beikmohammadi, Seyed Shahab-aldin Vakili.
Formal analysis: Atefeh Zandifar, Rahim Badrfam.
Funding acquisition: Atefeh Zandifar.
Investigation: Atefeh Zandifar, Rahim Badrfam, Amirhossein Hajaligol, Zohreh Khodaii, Ali Reza Soleimani.
Data curation: Atefeh Zandifar, Rahim Badrfam, Amirhossein Hajaligol, Mojtaba Kaveh, Mahya Beikmohammadi, Seyed Shahab-aldin Vakili.
Methodology: Atefeh Zandifar, Rahim Badrfam, Tyler Kjorvestad, Ali Reza Soleimani, Zohreh Khodaii.
Project administration: Atefeh Zandifar, Rahim Badrfam.
Resources: Atefeh Zandifar, Rahim Badrfam.
Software: Atefeh Zandifar, Rahim Badrfam, Amirhossein Hajaligol, Mojtaba Kaveh, Mahya Beikmohammadi, Seyed Shahab-aldin Vakili.
Supervision: Atefeh Zandifar and Rahim Badrfam, Zohreh Khodaii, Ali Reza Soleimani, Tyler Kjorvestad.
Validation: Atefeh Zandifar and Rahim Badrfam, Zohreh Khodaii, Ali Reza Soleimani, Tyler Kjorvestad.
Visualization: Atefeh Zandifar and Rahim Badrfam, Tyler Kjorvestad.
Writing—original draft: Atefeh Zandifar and Rahim Badrfam.
Writing—review and editing: Atefeh Zandifar and Rahim Badrfam.
All authors reviewed and approved the final manuscript and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Alborz University of Medical Sciences, Grant/Award Number: IR.ABZUMS.REC.1402.013.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.