
Abstract
Objective
Psychiatric disorders are prevalent among heart failure (HF) patients and depression is a common psychiatric disorder. The benefit effect of dietary fiber on depression has been reported. We aimed to assess the association between dietary fiber intake and depressive symptoms.
Method
A cross-sectional analysis was conducted of NHANES data collected 2005-2018 from adults ≥18 years with physician-diagnosed HF. Total and source-specific dietary fiber intake (g/day) was calculated from the average of two 24-hour dietary recalls using USDA’s AMPM protocol. Age, sex, race, education, smoking status, diabetes, hypertension, renal function, and medication use were adjusted in analyses. Survey-weighted logistic regression models examined associations between fiber intake and depression (PHQ-9 ≥10), with adjustment for confounding variables. Sensitivity analyses examined modification by BMI categories (<25, 25-29.9, ≥30 kg/m2) and HF duration (≤5 vs >5 years).
Results
A total of 1041 participants were included, of which 188 (18.06%) with depression symptoms. High total dietary fiber intake (OR = 0.50, 95% CI: 0.29-0.86) and vegetable fiber intake (OR = 0.49, 95% CI: 0.25-0.97) were associated with the lower odds of depression in HF patients.
Conclusion
Depression is associated with vegetable fiber, but not with fiber from grains or fruits. Depression is less common in patients with HF who consume high levels of total dietary fiber and vegetable fiber.
Introduction
Heart failure (HF) is a progressive clinical syndrome which usually appears in the final stage of cardiovascular disease (CVD), affecting over 64 million individuals worldwide.1,2 Mental health disorders, particularly clinical depression, are highly prevalent in this population, with meta-analyses estimating that nearly one-third of HF patients are affected. 3 Furthermore, depression is an independent prognostic factor associated with a significantly higher risk of mortality in HF patients. 4 Therefore, identifying modifiable lifestyle factors to preserve psychological well-being in HF patients is imperative.
Dietary fiber comprises non-digestible carbohydrates derived from plant-based foods, characterized by diverse physicochemical properties including solubility, viscosity, and fermentability that dictate their physiological effects. Beyond its established role in metabolic health, emerging evidence links high fiber intake to improved psychological outcomes 5 in the general population through gut microbiota modulation and subsequent production of bioactive metabolites.6-8 Specifically, Saghafian et al 9 reported a protective, dose-response relationship between total fiber intake and depression. Mechanistically, fiber-mediated alterations in gut pH and permeability are thought to attenuate systemic inflammation, thereby mitigating depressive symptomatology. 5
Although these benefits are established in the general population, data specific to cardiovascular disease (CVD) patients remain scarce. A single study in hypertensive patients suggested a similar inverse association between fiber intake and depression risk. 10 However, the differential effects of fiber sources, such as vegetables, fruits, and cereals, have not been explored in HF. This represents a critical knowledge gap, as the biological mechanisms linking fiber to mental health are source-specific.5,11 For instance, vegetable fibers (eg, inulin) are fermented into short-chain fatty acids (SCFAs), which inhibit hippocampal NLRP3 inflammasome activation. 6 Additionally, vegetable fibers contain polyphenolic compounds (quercetin) that suppress the NF-κB pathway and reduce levels of pro-inflammatory factors such as IL-6. 5 Leafy greens are rich in folate, which influences neurotransmitter synthesis by acting as a cofactor in 5-HT production. 12 Thus, compared to fibers from grains or fruits, vegetable fiber possesses unique functional attributes, such as high viscosity and antioxidant capacity, which may confer superior neuroprotection in the context of HF. 13
We hypothesized that higher intake of vegetable-derived dietary fiber is associated with lower odds of depression in HF patients. Using cross-sectional data from the National Health and Nutrition Examination Survey (NHANES), we analyzed the associations between depression prevalence and fiber intake from specific sources (fruits, vegetables, cereals) to identify targeted dietary strategies for mitigating psychiatric symptoms in this vulnerable population.
Methods
Study participant
Data for this cross-sectional study were derived from NHANES cycles spanning 2005-2018. NHANES, administered by the Centers for Disease Control and Prevention (CDC), is a nationally representative, multistage probability survey designed to assess the health and nutritional status of the U.S population across all life stages. All participants provided written informed consent, and the original protocols received ethical clearance from the NHANES Institutional Review Board, precluding additional approvals for this secondary analysis.
In this study, the inclusion criteria were: (1) aged ≥18 years old; (2) documented HF diagnosis; (3) complete dietary fiber intake data. The exclusion criteria were: missing dietary fiber, weight, or depression status information.
Depression Assessment
The primary outcome was depression risk among heart failure (HF) patients, assessed using the Patient Health Questionnaire-9 (PHQ-9) depression score. This validated 9-item instrument evaluates depressive symptom frequency over the preceding 2 weeks. 14 Total PHQ-9 score ranges from 0 to 27 point, of which 0-9 point was no depression, 10-14 points was moderate depression, 15-19 point was moderately severe depression, and 20-27 point was severe depression. 13 Consistent with established clinical thresholds, 15 participants scoring ≥10 were classified as clinically relevant depressive symptoms.
Dietary Fiber Intake Assessment
Dietary fiber intake is quantified via 24-hour recall interviews conducted by trained staff at the NHANES Mobile Examination Centers (MECs). Participants detailed all foods and beverages consumed during the preceding 24-hour period. Fiber content was derived using the USDA Food Patterns Equivalents Database (FPED), 16 which standardizes consumption data by breaking items down into the following categories: Grains were categorized as whole or refined. Fruit included fruit juice, citrus fruits, melons, berries, and other fruits. Vegetables are categorized as red and orange vegetables, dark green vegetables, potatoes, and other vegetables.
The dietary fiber sources we focused on were total fiber and fiber from cereal fiber, fruits and vegetables. Fiber intake consumption was defined as the mean total fiber intake. Four types of dietary fiber were analyzed: total fiber, cereal fiber, vegetable fiber and fruit fiber. Vegetable fiber is defined as soluble fibre of more than 2 g/serving (carrots, broccoli). Cereal fiber is primarily insoluble (wheat bran).
Control Variables
Candidate variables, including demographic, comorbidities, lifestyle variables, were selected based on clinical relevance with depression (P < 0.10) in the weighted univariable logistic regression analysis. Age, gender and race were demographic information obtained from self-reported. The Poverty Income Ratio (PIR) was derived by dividing total family income by the poverty threshold, adjusting for family size, survey year, and state of residence. 17 Smoking was assessed by the question “Smoked at least 100 cigarettes in life” (yes/no). 18 Drinking was assessed by the question “Had at least 12 alcohol drinks/1 yr?” If participants answered negatively to this question, s/he was considered never drinker. Alcohol consumption was categorized using responses to: “How often did you drink alcohol over the past 12 months?” Occasional drinker: Less than 1 time per week (including non-drinkers). Regular drinker: 1 or more times per week. 19 Physical activity was quantified as total weekly Metabolic Equivalent of Task (MET)-minutes using the formula: physical activity (MET·min/week) = recommended MET × exercise time for corresponding activities (min/day) × the number of exercise days per week (day). 20 The age of onset of HF was obtained from the question “How old were you when a specialist first told you that you had HF?”. Duration of HF was calculated as the present participant’s age minus the age at the first HF diagnosis. Sleep disorders was assessed by the question “Ever told by doctor have sleep disorder?” (yes/no). 21 Thyroid disease was defined by the question “Has a doctor or other health professional ever told you that you had another thyroid problem?’ (yes/no). 22 Heart disease, including angina, myocardial and coronary heart disease were assessed by the question “Ever told you had angina/angina pectoris”, “Ever told you had myocardial infarction?” and “Ever told you had heart attack (also called myocardial infarction)?”. Stroke was defined by the question “Ever told you had a stroke?”. 23 Hypertension was defined as systolic blood pressure (SBP) ≥130 mmHg, diastolic blood pressure (DBP) ≥ 90 mmHg, self-reported or taking blood pressure medication. 24 Dyslipidemia was defied as total cholesterol (TC) ≥200 mg/dL or triglyceride (TG) ≥150 mg/dL or low-density lipoprotein cholesterol (LDL-C) ≥130 mg/dL or high-density lipoprotein cholesterol (HDL-C) ≤40 mg/dL, or self-reported hypercholesterolemia or taking lipid-lowering medication. 25 Diabetes were defined as glycosylated hemoglobin (HbAlc) ≥6.5%, or fasting glucose≥126 mg/dL, or 2 h glucose tolerance test (OGTT) ≥200 mg/dL or confirmed to be taking insulin or hypoglycemic agent or self-reported history of diabetes. 26 Emotional support was defined by the question “Anyone to help with emotional support?” (yes/no). The definition of CVD drugs and psychotherapeutic agents were also described in the “Potential covariate”. CVD drug use was identified based on participants’ self-reported use of the following drugs: antiadrenergic agents, antianginal agents, antiarrhythmic agents, inotropic agents, miscellaneous cardiovascular agents, vasodilators, vasopressors, angiotensin II inhibitors, aldosterone receptor antagonists, and renin inhibitors. Psychotherapeutic agents use was assessed using prescription drug information from the NHANES module: “Do you take medication for these feelings?”
Statistical Analysis
All analyses used SAS 9.4, accounting for NHANES’ complex survey design. Sampling weights (WTDRD1), stratification (SDMVSTRA), and clustering (SDMVPSU) were incorporated using PROC SURVEYFREQ to ensure representative estimates.
Continuous variables are expressed as weighted mean ± standard error (SE). Group comparisons (depressed/non-depressed) employed survey-weighted linear regression. Multiple imputation by chained equations (MICE) to generate five complete datasets, with sensitivity analysis confirming a coefficient of variation of less than 10% compared to complete-case analysis (Table S1). The weighted univariable logistic regression analysis was used to screen the covariates that associated with depression (Table S2) and multivariate logistic regression models were further used to explore the association between dietary fiber intake and the odds of depression in HF patients, with odds ratios (ORs) and 95% confidence intervals (CIs). Model 1 was a crude model without adjusting covariates. Model 2 adjusted age, gender, education, poverty-to-income (PIR), marital status, stroke, drug for CVD and psychotherapeutic agents. Model diagnostics were performed to ensure robustness. Multicollinearity was assessed using the Variance Inflation Factor (VIF), with all values < 5 indicating no significant collinearity. Model calibration was evaluated using the Hosmer-Lemeshow test, and discriminative ability was assessed using the C-statistic (AUC). Two-sided P < 0.05 was considered as statistically significant.
Results
Description of the Study Population
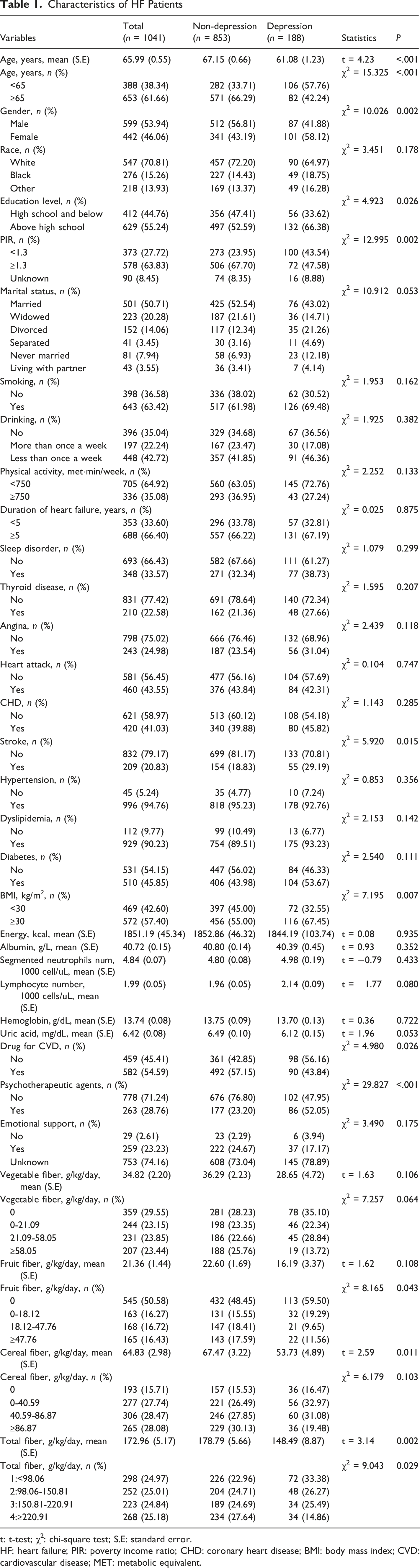
A total of 1355 HF patients aged ≥18 years were screened. Among them, 196 patients missing dietary fiber intake information, 39 patients missing weight data, and 79 patients missing depression test were excluded. The analytical cohort included 1041 HF patients, among whom 188 (18.1%) had depression. Figure 1 details participant selection. Characteristics of included participants were shown in Table 1. Patients with depression had lower intake of vegetable fiber, fruit fiber, cereal fruit and total fiber compared with the non-depression patients. Differences were found in age, gender, the level of education, PIR and BMI, the history of stroke, the use of CVD drug, psychotherapeutic agent and the level of fruit fiber, cereal fruit and total fiber intake between depression and non-depression groups (P < 0.05). The flow chart of population screening Characteristics of HF Patients t: t-test; χ2: chi-square test; S.E: standard error. HF: heart failure; PIR: poverty income ratio; CHD: coronary heart disease; BMI: body mass index; CVD: cardiovascular disease; MET: metabolic equivalent.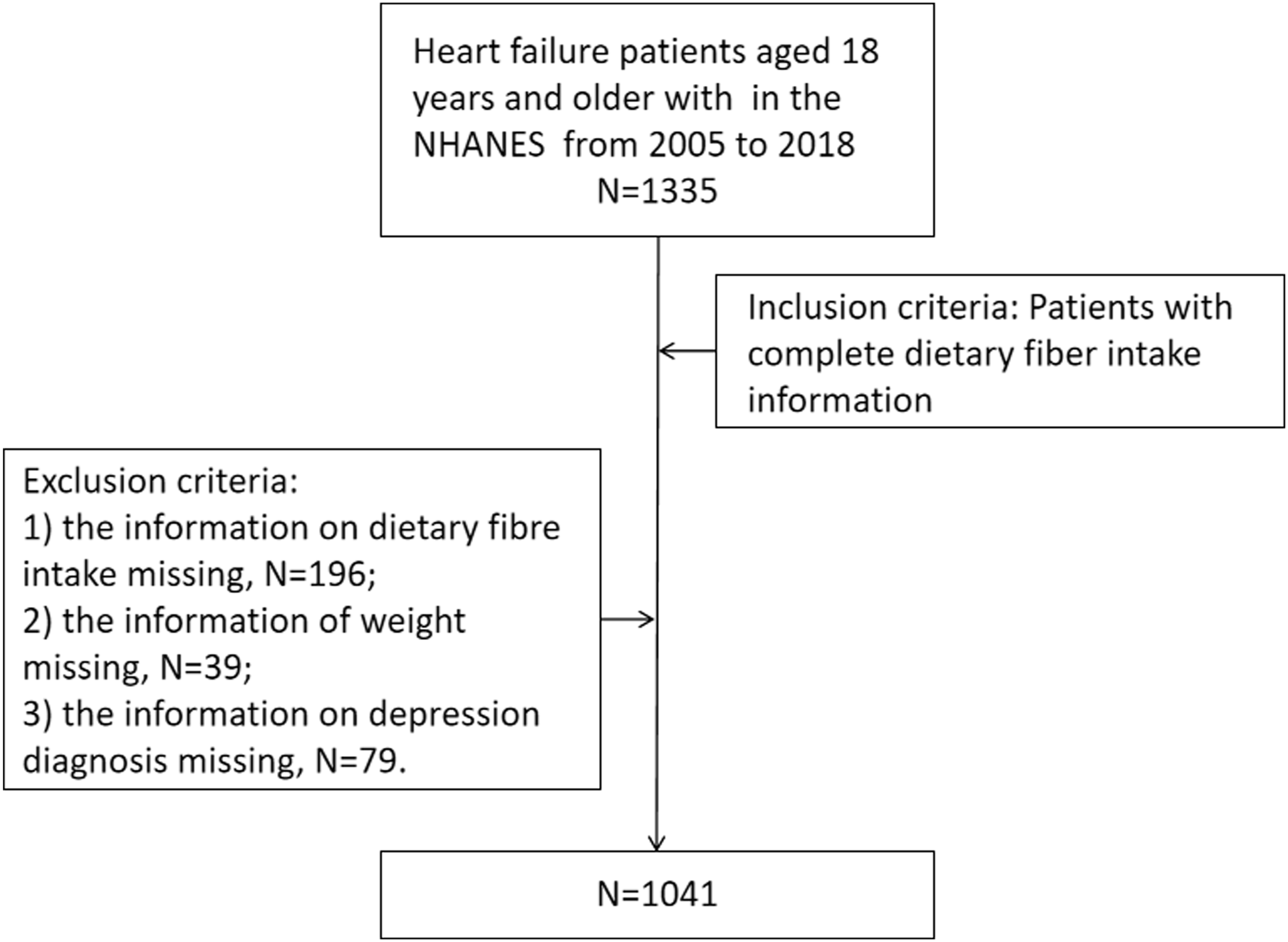
Associations Between Total Fiber Intake and its Different Sources and Depression
Association Between Total Dietary Fiber Intake and its Different Sources and Depression
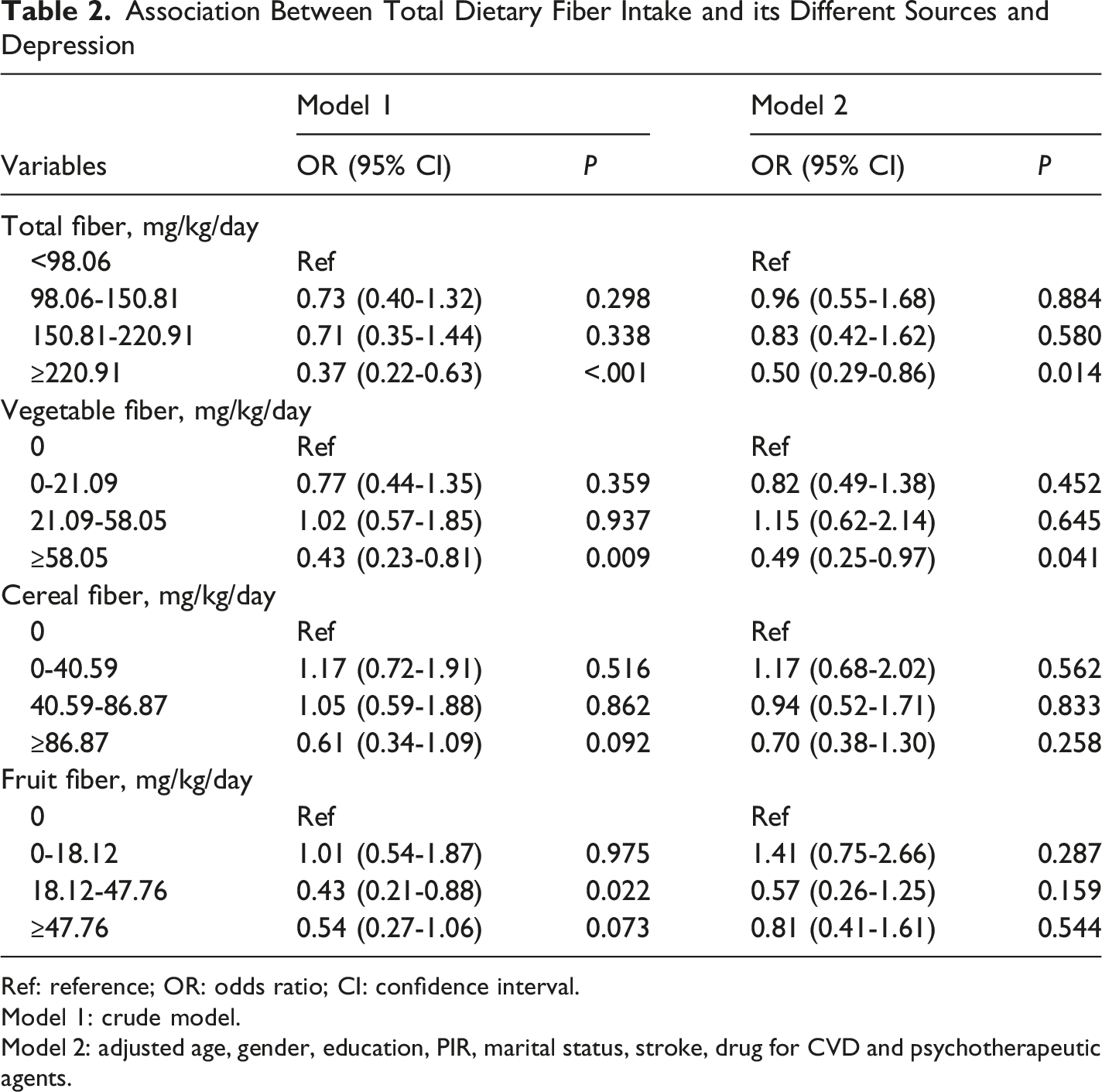
Ref: reference; OR: odds ratio; CI: confidence interval.
Model 1: crude model.
Model 2: adjusted age, gender, education, PIR, marital status, stroke, drug for CVD and psychotherapeutic agents.
Associations Between Total Fiber Intake and its Different Sources and Depression Based on BMI and Duration of HF
Association Between Total Dietary Fiber Intake and its Different Sources and Depression Stratified by BMI
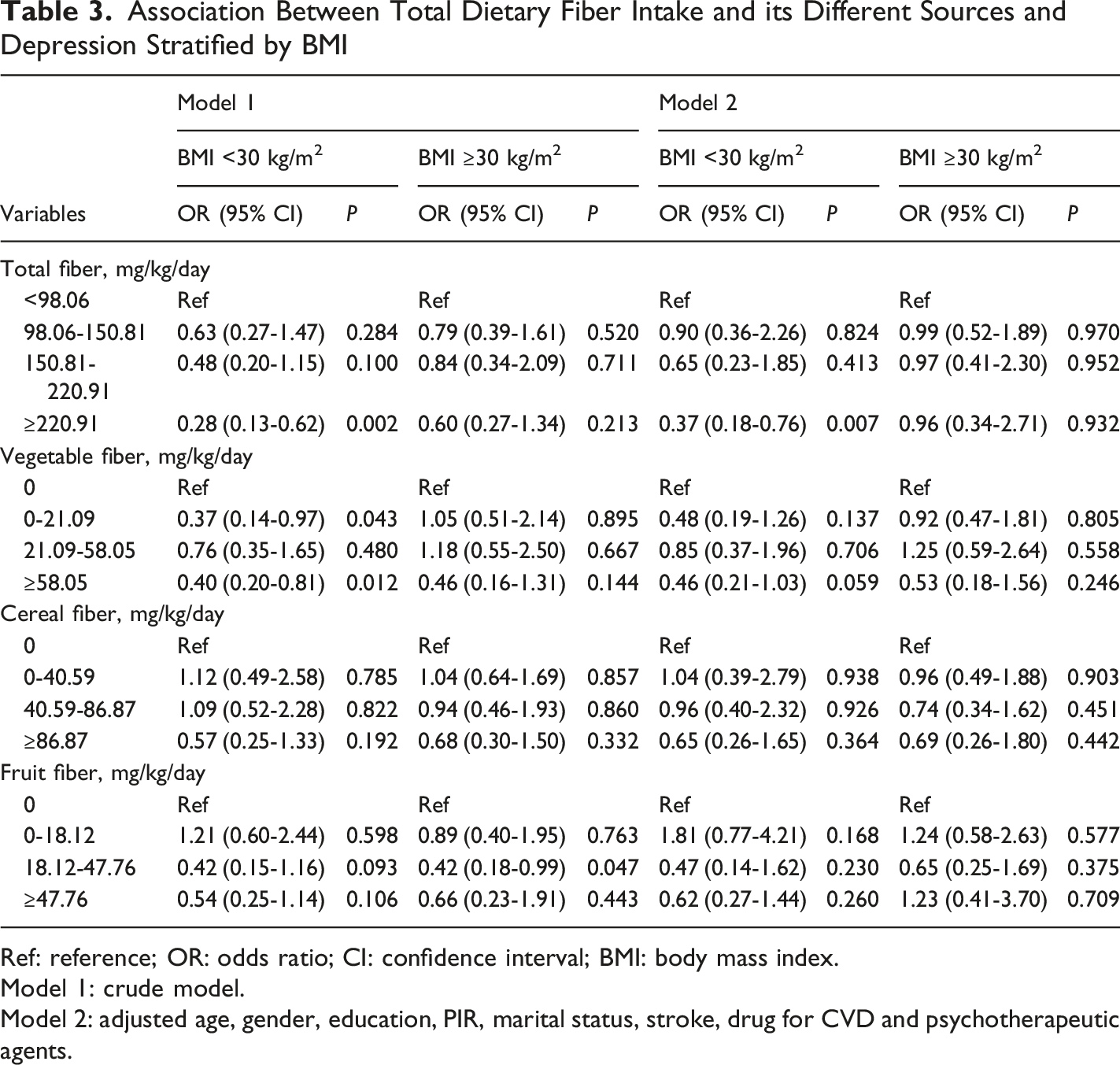
Ref: reference; OR: odds ratio; CI: confidence interval; BMI: body mass index.
Model 1: crude model.
Model 2: adjusted age, gender, education, PIR, marital status, stroke, drug for CVD and psychotherapeutic agents.
Association Between Total Dietary Fiber Intake and its Different Sources and the Odds of Depression Stratified by Duration of HF
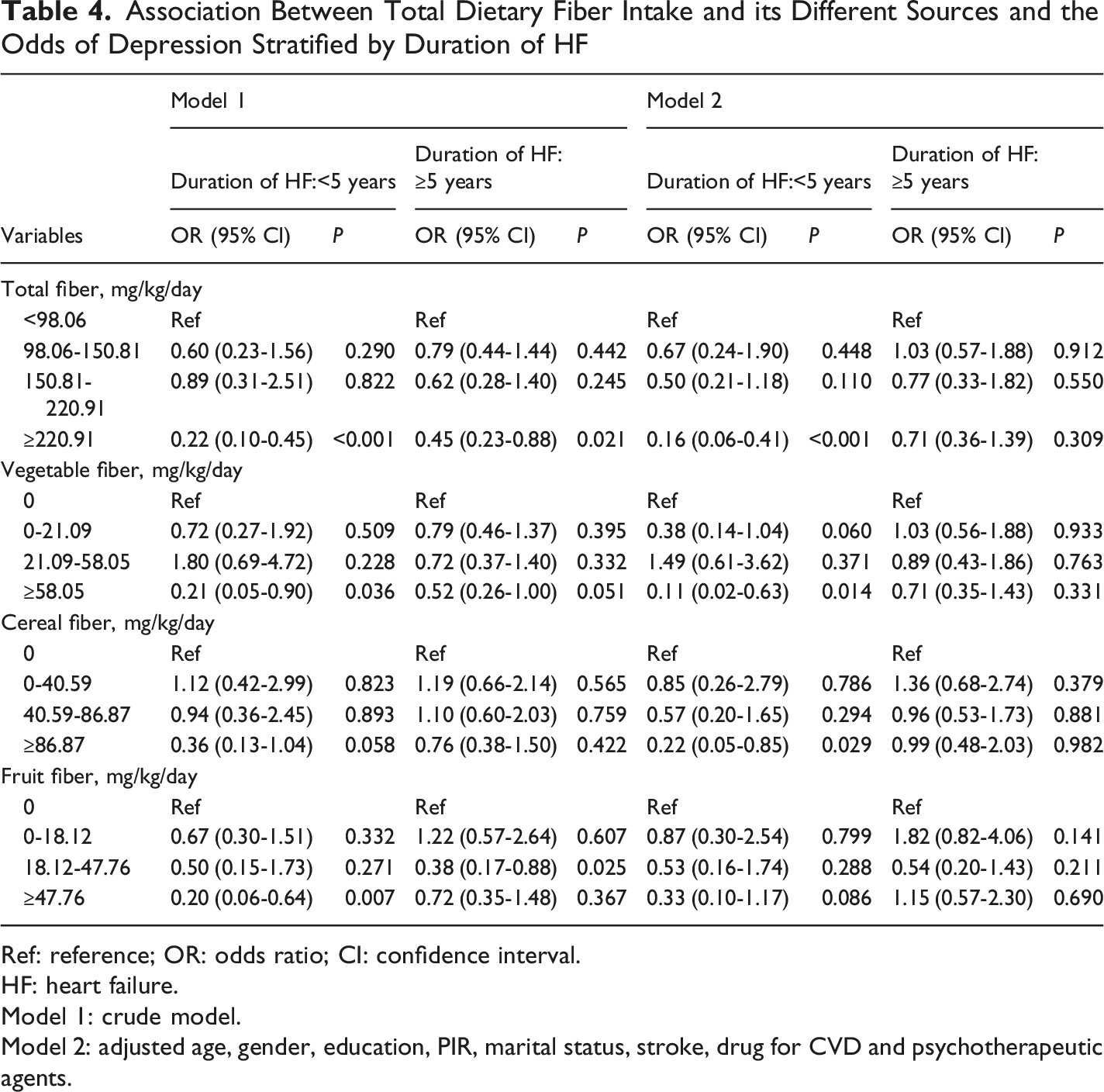
Ref: reference; OR: odds ratio; CI: confidence interval.
HF: heart failure.
Model 1: crude model.
Model 2: adjusted age, gender, education, PIR, marital status, stroke, drug for CVD and psychotherapeutic agents.
Discussion
In this cross-sectional study of HF patients, higher intake of total dietary fiber and specifically vegetable-derived fiber demonstrated a significant inverse association with odds of depression. No significant associations were observed for cereal or fruit fiber sources. These findings suggest that targeted dietary interventions focusing on vegetable fiber correlate with lower odds of depressive symptoms in the HF population.
Depression is a common comorbid condition in HF patients and constitutes a predictor of poor prognosis. 27 The burden of HF combined with depression is increasing annually. 28 HF and depression share overlapping pathophysiological mechanisms, including excessive immune activation and elevated circulating inflammatory cytokines. 29 Meta-analyses indicate that plasma levels of C-reactive protein, tumor necrosis factor-α, and interleukin-6 are significantly elevated in major depression and correlate positively with its incidence.30,31 These inflammatory factors are also significantly increased in HF patients, potentially mediating the increased risk of depression in this population.
Dietary fiber comprises non-digestible carbohydrates that escape small intestinal digestion and undergo fermentation in the colon. 32 Recognized globally as a crucial nutrient, dietary fiber intake is inversely associated with obesity, 33 type 2 diabetes, 34 several cancers, 35 CVD 36 and coronary heart disease. 37 Emerging evidence highlights the role of the gut-brain axis, wherein gut microbiota regulates emotional and cognitive functions.38-41 Compared to healthy controls, patients with depression exhibit gut dysbiosis characterized by an enrichment of pro-inflammatory bacteria.42,43 Consistent with prior research in Korean women 13 and US adults,44,45 our study found that total and vegetable fiber intake were inversely associated with depression, whereas fruit and cereal fibers were not. This source-specific effect may be attributed to vegetable-derived bioactive compounds (eg, polyphenols) and soluble fiber. A study from The Furukawa Nutrition and Health Study found that higher dietary fiber intake from vegetables and fruits may be associated with lower odds of depression. 46 Vegetable is generally universally promoted as healthy, and the human gut microbiota becomes diversified from the adequate intake of vegetables. 12 Inflammatory pathways may mediate the link between dietary fiber intake and depression. However, it is important to note that high fiber intake is often collinear with overall healthy dietary patterns and lifestyle behaviors, making it difficult to isolate the specific contribution of fiber from these interrelated factors. High dietary fiber intake modulates the pH and osmotic pressure of the intestinal lumen, which reduces the production of pro-inflammatory mediators derived from the gut and modifies enteroendocrine-neural signaling. This may reduce depressive symptoms. 5 Further longitudinal studies are needed to explore the association between vegetable, fruit and cereal intake and depression in different populations.
Subgroup analyses revealed that high total dietary fiber intake was associated with the lower odds of depression in HF patients with BMI <30 kg/m2 and those with a disease duration less than 5 years. While obesity is a known risk factor for both HF and depression,47,48 high-fiber diets may reduce total energy intake through enhanced satiety, offering a non-pharmacological strategy for cardiac metabolic management.49,50 This establishes fiber-rich dietary patterns as a non-surgical strategy for fat mass management that can enhance cardiometabolic outcomes alongside surgical interventions. Moreover, the duration of HF is associated with the odds of depression. It is generally believed that the longer the disease sustain; the higher odds of depression occurs. Our study suggested that in HF patients with BMI <30 kg/m2 or with HF duration <5 years, higher dietary fiber intake is associated with reduced depression risk. The pathophysiological mechanisms underlying this association require further investigation using biomarker and mediation analyses.
Current evidence on dietary fiber and depression in HF remains limited. We used survey-weighted multivariable logistic regression models to adjust for key covariates, including age, sex, comorbidities, medication use and socioeconomic status. Our results suggest that targeted increases in vegetable-derived fiber, beyond general fiber recommendations, are associated with better mental health outcomes in people with HF. Although we did not assess dietary supplements, these findings provide a rationale for prioritizing whole-food, vegetable-rich interventions to improve mood regulation in this high-risk population.
Study Limitations
This study has several limitations. First, dietary intake was assessed via self-reported 24-hour recalls, which may not capture long-term habitual intake and is vulnerable to recall bias. The cross-sectional design precludes causal inference, and reverse causality (eg, depression reducing appetite) cannot be excluded. Additionally, depression was defined by a PHQ-9 score ≥10, reflecting symptom severity rather than a clinical diagnosis of major depressive disorder. Second, despite adjusting for multiple covariates, residual confounding remains possible. Important confounders, including total energy intake, BMI, physical activity, diabetes, sleep disorders, detailed antidepressant use, and overall diet quality were not fully accounted for in Model 2. Given that dietary fiber correlates strongly with overall healthy dietary patterns, the observed associations may reflect broader lifestyle factors rather than a direct, fiber-specific effect. Third, excluding ∼25% of participants with missing data may have introduced selection bias, potentially underestimating the true association due to underrepresentation of individuals with severe depression or poorer health. Finally, we lacked data on HF severity; thus, these associations warrant confirmation across different stages of HF. Furthermore, subgroup analyses (stratified by BMI and HF duration) were exploratory and not prespecified. We did not perform formal interaction tests or adjust for multiple comparisons, so these findings should be interpreted as hypothesis-generating rather than confirmatory.
Conclusion
High total dietary fiber and vegetable fiber intake were associated with the lower odds of depression in HF patients. No relationships were found between fruit fiber and cereal fiber intake and the odds of depression. High dietary fiber supplementation and fiber-rich food intake was associated with lower odds of depression symptoms in HF patients.
Supplemental Material
Supplemental Material - Dietary Fiber Intake and Depression in Heart Failure Patients: A Cross-Sectional Study From NHANES Database
Supplemental Material for Dietary Fiber Intake and Depression in Heart Failure Patients: A Cross-Sectional Study From NHANES Database by Xuehui Qu, MM, Nan Zhou, BM and Lina Wang, MM in The International Journal of Psychiatry in Medicine.
Supplemental Material
Supplemental Material - Dietary Fiber Intake and Depression in Heart Failure Patients: A Cross-Sectional Study From NHANES Database
Supplemental Material for Dietary Fiber Intake and Depression in Heart Failure Patients: A Cross-Sectional Study From NHANES Database by Xuehui Qu, MM, Nan Zhou, BM and Lina Wang, MM in The International Journal of Psychiatry in Medicine.
Footnotes
Ethical Considerations
All participants provided written informed consent; original protocols received ethical clearance from the NHANES Institutional Review Board. Ethical approval was waived by the Ethics Committee of our hospital in view of the retrospective nature of the study. The study was performed in accordance with the ethical standards as laid down in the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards.
Author Contributions
Conceptualization: Xuehui Qu, Nan Zhou
Data curation: Xuehui Qu
Formal analysis: Xuehui Qu
Methodology: Nan Zhou
Resources: Lina Wang
Validation: Xuehui Qu
Visualization: Lina Wang
Writing-original draft: Xuehui Qu, Nan Zhou
Writing-review & editing: Lina Wang
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.