
Abstract
Objective
Delirium is a common psychiatric condition in general hospitals and a known risk factor for suicidal ideation. However, little is known about suicide deaths among patients with delirium. This study examined the clinical characteristics of hospitalized patients with delirium who died by suicide.
Methods
Analyzed were anonymized medical incident data reported to the Japan Council for Quality Health Care from 2010 to 2022. Among reported inpatient suicide deaths, cases with documented delirium were identified and analyzed.
Results
A total of 403 inpatient suicides were identified during the study period, of which 12 (5.1%) involved patients with delirium, all of whom were admitted to medical wards. The most common methods of suicide were jumping from a height and hanging, often occurring in hospital rooms. Suicidal ideation and distress related to physical illness, including depression, anxiety, and pain, were frequently observed. However, only about half of the patients had received specialist interventions, such as psychiatric consultation. Patient characteristics, including sex and primary illness, were consistent with previous studies of inpatient suicide, with the exception of age.
Conclusions
While this study cannot determine whether delirium independently contributes to suicide risk, the findings suggest that recognizing and managing delirium—together with timely specialist interventions, such as psychiatric consultation, and standard inpatient safety measures, including restricting access to means and making appropriate decisions regarding patient leave—may be important components of suicide prevention in general hospital settings. Further research is needed to better understand how delirium influences suicide risk.
Introduction
Delirium is a common acute and fluctuating neuropsychiatric syndrome characterized by disturbances in attention and awareness, accompanied by additional cognitive disturbances such as memory deficits, disorientation, language impairment, visuospatial dysfunction, or perceptual abnormalities, as defined in the DSM-5-TR. 1 Delirium commonly occurs in medically ill patients and has been reported in approximately 10-30% of inpatients in general hospitals.2-4 The prevalence is substantially higher among critically ill patients in intensive care units (approximately 60-90%) and terminally ill cancer patients (about 45-90%).2,4 Common precipitating factors include infections, metabolic disturbances, medications, surgery, and advanced medical illness.2-4 Delirium episodes are typically transient, lasting from several days to weeks, but may persist longer depending on underlying conditions.2-4 Delirium has been associated with adverse outcomes, including prolonged hospitalization and increased mortality.2-4 A recent review of patients’ experiences indicates that delirium is commonly perceived as an intensely distressing state, characterized by fear, anxiety, confusion, and vivid unreal experiences such as hallucinations and nightmares. 5 In addition, several studies have suggested an association between delirium and suicidal ideation.6,7 Suicide is a complex behavior resulting from the interaction of multiple biological, psychological, social, and environmental factors, and identifying its precise causes remains challenging. 8 However, little is known about the specific characteristics of suicide deaths among patients with delirium. In a previous review, Ballard et al noted that although reports of inpatient suicides associated with delirium are rare, clinical observations have suggested that delirium may contribute to suicide among hospitalized patients. 9 Despite these observations, empirical data on suicide related to delirium remain extremely limited.
One of the few studies to address this issue is by White et al, 10 which analyzed inpatient suicides by jumping from a height in a general hospital. The study reported that 3 of 8 patients who died by suicide had delirium at the time of the incident, all exhibiting signs of agitation. White et al 10 suggested that agitation could be a critical indicator of delirium and suicidality. Regarding the mechanisms by which delirium influences suicide, Matsubara and Horikawa 11 proposed that delirium may intensify patients’ distress regarding their underlying physical illness and its treatment, increasing suicidal ideation. They also noted that persecutory delusions or hallucinations associated with delirium may contribute to suicidality. Similarly, Glickman 12 reported that delirium tremens was present in 6 of 22 patients who died by suicide and in 8 of 23 who attempted suicide, with many incidents occurring within 24 h of delirium onset. Other studies have examined the prevalence of delirium among inpatients who died by suicide. Suominen et al 13 reported that 3 out of 26 inpatients who died by suicide had delirium. Additionally, several studies have found that 7-14% of inpatients who attempted suicide while admitted to medical wards were diagnosed with delirium.14-16
Despite these findings, few studies have examined the clinical characteristics of patients with delirium who die by suicide. This study examined the clinical characteristics of hospitalized patients with delirium who died by suicide.
Methods
This study utilized medical incident data from the Japan Council for Quality Health Care (JCQHC), a third-party organization that evaluates medical institutions through the “Project to Collect Medical Near-Miss/Adverse Event Information”. 17 Launched in 2004, this project aims to enhance patient safety by collecting and analyzing data on medical accidents, including suicides. All data are fully anonymized prior to public release and are available through the JCQHC’s publicly accessible reporting system. Reports are gathered from hospitals with mandatory reporting requirements, primarily large academic and public hospitals, as well as by voluntarily participating institutions. As of December 2022, the project included 275 hospitals subject to mandatory reporting and 883 voluntarily participating hospitals. 18
For this study, we extracted cases of suicide deaths among hospitalized patients reported between 2010 and 2022. The study population consisted of patients who died by suicide during their hospitalization, including incidents that occurred outside the hospital. Cases were eligible for inclusion only when the medical incident data explicitly documented that the patient had delirium or had been diagnosed with delirium. We did not infer delirium based on symptom descriptions alone, and reports describing isolated symptoms without a diagnosis were excluded.
For the selected cases, we analyzed patient characteristics, including the admitting department, primary disease or reason for admission, sex, and age group, as well as details of the suicide, including the method and location. In Japan, hospital-based palliative care teams are frequently involved in the management of delirium, particularly among patients with cancer or severe physical symptoms. In addition, some hospitals have dementia care teams that may also be involved in the management of delirium. Therefore, the incident reports often documented psychiatric consultation, palliative care team involvement, or dementia care team involvement as forms of specialist interventions. These items were obtained from structured fields within the reporting system. In contrast, information regarding specialist interventions (such as psychiatric consultation or palliative care team involvement), delirium-related symptoms, and events leading up to the suicide attempt was not included in the structured fields. These items were extracted manually by the authors through a detailed review of the free-text narrative sections of the medical incident reports. Descriptive analyses were conducted to summarize patient characteristics, delirium-related symptoms, suicide methods, and clinical circumstances.
Because the dataset was fully anonymized prior to public release, no anonymization procedures were required.
Results
Between 2010 and 2022, a total of 3978 death reports were filed, of which 403 documented suicides during hospitalization. Delirium was clearly noted in 12 of the 403 cases, and only these 12 patients were included in the analysis. Cases where delirium was suspected, such as those involving hallucinations due to physical deterioration, were excluded unless delirium was clearly diagnosed. All included cases involved patients admitted to non-psychiatric departments (ie, medical wards). Of the 403 inpatient suicides, 234 involved patients who were admitted to medical wards. Among these 234 cases, 5.1% (12 cases) involved patients with delirium. This proportion increased to 8.2% (9 out of 110) in patients aged 70 and older.
Details of Suicide Deaths in Inpatients With Delirium
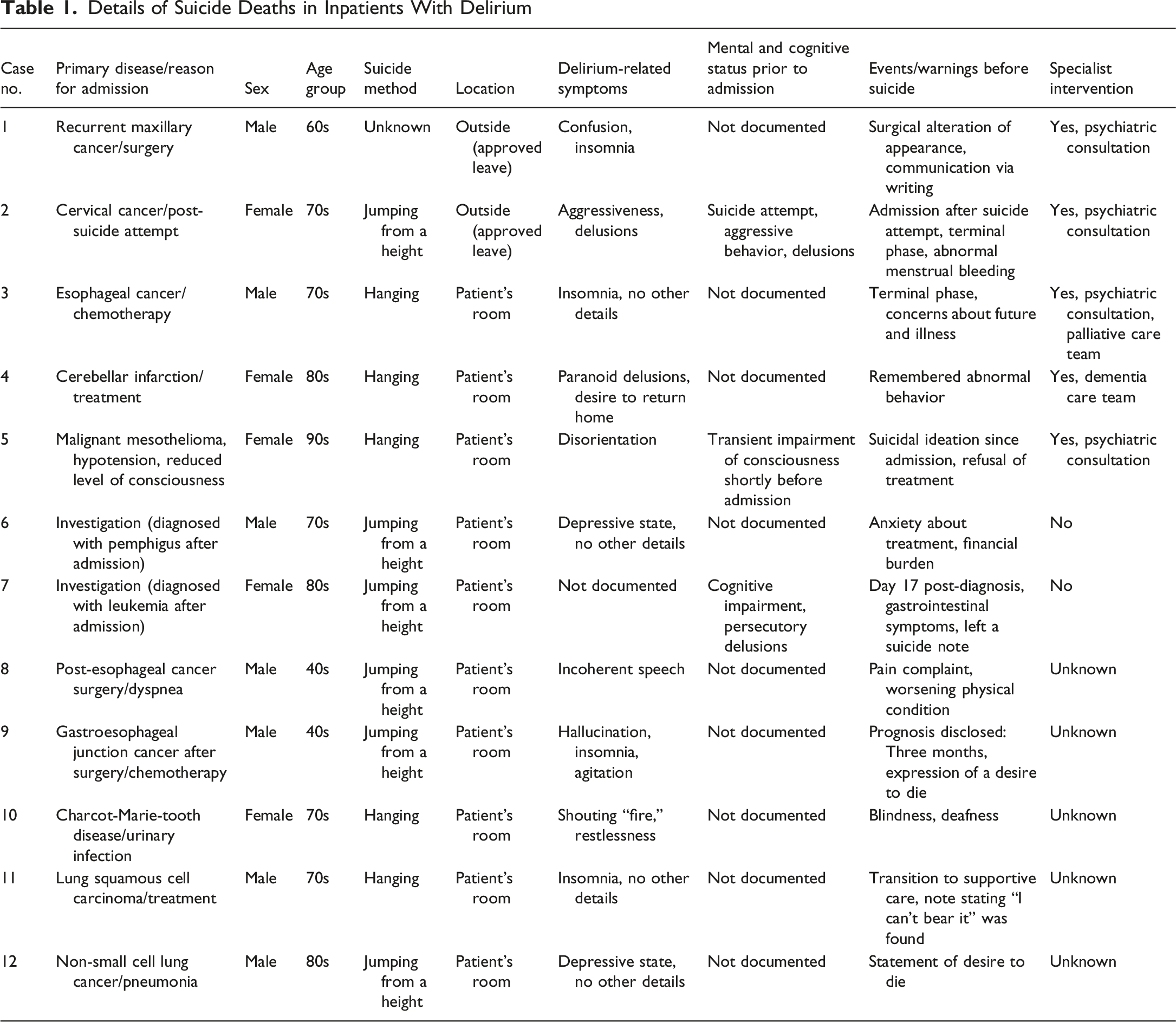
The primary suicide methods were jumping from a height (6 cases) and hanging (5 cases). Most suicides occurred in hospital rooms (10 cases), while 2 occurred outside the hospital. In 4 cases, patients had verbally expressed suicidal ideation, such as saying “I want to die,” prior to the incident. Additional concerns noted in the reports included anxiety about prognosis in one patient, refusal of treatment in 2 patients, disclosure of prognosis in one patient, and a terminal stage of illness in 2 patients. Delirium-related symptoms described in the medical incident data included hallucinations, insomnia, disorientation, and delusions.
Only 5 of the 12 patients had received a specialist intervention. Among these 5 patients, the medical incident data provided very limited information regarding the content of the evaluations. Only one patient was referred because of suicidal ideation. The remaining referrals were requested for reasons such as agitation, insomnia, or suspected delirium, although the medical incident data did not include sufficient detail to clarify the specific assessments performed. Two cases occurred during authorized leave from the hospital: one after medical staff believed that returning home might improve the patient’s delirium, and the other due to the patient’s strong desire to go outside.
Discussion
This study examined the characteristics of suicide deaths among hospitalized patients with delirium. All cases occurred among patients admitted to medical wards, with no cases reported among those admitted to psychiatric wards. Consistent with previous findings on inpatient suicides while admitted to medical wards,9,16,17 cancer was the most common underlying illness, and more cases involved male patients than female patients. While a previous review reported a mean age of 54.3 years for inpatient suicide deaths, 9 our dataset included only age categories rather than exact ages, making it impossible to calculate a mean age for comparison. Instead, the most frequent age group in this study was 70-79 years, followed by 80-89 years. This difference likely reflects the focus on delirium, a condition that is more prevalent among older adults.
Approximately half of the patients received specialist interventions such as a psychiatric consultation. A previous survey 19 also found that psychiatric consultations were rare among inpatients who died by suicide while admitted to medical wards. These findings highlight the importance of access to psychiatric or palliative care support for hospitalized patients with delirium. Aside from age, the characteristics of inpatients with delirium who died by suicide, such as sex and underlying illness, align with those reported in earlier studies of inpatient suicide while admitted to medical wards.
Except for one case with an unclear method, all patients died by jumping from a height or hanging. The most common location for suicide attempts was the patient’s own hospital room, consistent with previous studies.9,19,20 Two cases occurred during approved leave. In one case, despite a history of prior suicide attempts and ongoing aggression and delusions, the patient was inappropriately allowed to leave, based on the mistaken belief that returning home would alleviate their delirium. To prevent suicides among patients with delirium during hospitalization, it is essential to implement measures similar to those recommended for preventing inpatient suicide in general.21-23 These include restricting access to means that could be used for hanging, restricting window opening, and making careful decisions regarding leave permission.
Known risk factors for inpatient suicide include verbal expressions of suicidal ideation, physical symptoms such as pain, worsening physical condition, and depression.9,19,23 Similar factors were observed in this study and should be considered when assessing suicide risk in patients with delirium. Morita et al. 24 reported that, among 9 terminal cancer patients with delirium and suicidal ideation, 4 no longer expressed such ideation within 2 weeks. This suggests that suicidal ideation in delirious patients, even those who are seriously ill, may be transient. Clinicians should not consider suicidal ideation in delirium to be fixed; instead, they should respond with comprehensive suicide prevention efforts, including prompt delirium treatment, environmental safety measures, and frequent monitoring.
Previous literature has suggested that delirium may increase suicide risk through agitation, impulsivity, hallucinations, and delusions,10,11,13 but the specific contribution of these factors in the cases examined here remains unclear. Moreover, the present data do not clarify whether delirium independently contributes to suicide risk. Many patients had advanced malignancies, depression, pain, or substantial psychosocial burden, which may have played a major role in their vulnerability. Therefore, delirium should be regarded as a potentially interacting or amplifying factor rather than a direct causal mechanism. In Cases 2 and 5, where suicide risk was high at admission, delirium-related symptoms appeared temporally associated with heightened suicide risk; however, this interpretation remains speculative. Future research should investigate changes in suicide-related indicators, such as suicidal ideation, before and after delirium onset, and conduct detailed interviews with patients who survived suicide attempts during delirium.
In cases other than the 12 included in this study, several reports described suspected delirium that had not been formally documented, such as hallucinations post-admission, suggesting possible underrecognition of the condition. Moreover, this study focused solely on cases explicitly reported as suicides. In patients with organic mental syndromes, including delirium, deaths resulting from self-injurious behavior may sometimes be classified as accidental due to uncertainty about suicidal ideation. 25 These factors suggest that the prevalence of suicide among patients with delirium may have been underestimated. Therefore, identifying and managing delirium should be considered a key component of inpatient suicide prevention.
Delirium is typically a transient and reversible neuropsychiatric syndrome, and appropriate management is important for facilitating recovery. In this study, approximately half of the patients received specialist interventions, such as a psychiatric consultation or palliative care team involvement. However, the overall adequacy of delirium management could not be evaluated because the medical accident reports did not include information regarding routine delirium care, such as non-pharmacological interventions. Future research should examine how various approaches to delirium care, including psychiatric consultation, and standard non-pharmacological interventions, are associated with suicide prevention in hospitalized patients.
Study Limitations
This study has several limitations. First, it included only cases explicitly reported as suicides with clearly documented delirium. Some deaths resulting from the patient’s own actions may have been misclassified as accidental due to unclear suicidal ideation, 25 potentially leading to an underestimation of the true prevalence. Second, delirium was diagnosed based on available documentation, and some patients did not receive psychiatric evaluations, making the diagnosis potentially uncertain. Third, as a retrospective study, the temporal relationship between delirium and suicide could not be thoroughly examined. Specific details, such as the timing of suicide relative to delirium onset, remain unclear. Fourth, the medical incident reports did not specify the delirium subtype for each case. Although several cases exhibited features suggestive of hyperactive delirium—such as agitation or impulsive behavior—and others showed depressive or withdrawn states that may have reflected hypoactive delirium, it was not possible to determine whether the presentations were hyperactive, hypoactive, or mixed. Fifth, the medical incident reports rarely documented routine non-specialist delirium care, such as orientation interventions, environmental modifications, management of underlying medical conditions, or correction of sensory impairments. Consequently, it was not possible to determine whether these interventions had been implemented or to evaluate the overall adequacy of delirium management. Lastly, the small sample size limited statistical analysis and generalizability. Future large-scale, prospective studies involving patients with confirmed delirium are needed to clarify how delirium influences suicide risk. In particular, research should examine whether the characteristics and mechanisms of suicide differ across delirium subtypes, as this may help identify which specific delirium symptoms contribute to suicide risk.
Conclusion
This study highlights the characteristics of hospitalized patients with delirium who died by suicide. Suicidal ideation was documented in several cases prior to death, suggesting that warning signs may be present in at least some patients. This study provides new evidence regarding the clinical and situational contexts in which these rare but serious events occur. These patients shared several established suicide risk factors with other inpatients, including suicidal ideation and distress related to physical illness. However, specialist intervention such as psychiatric consultations were documented in only about half of the cases. Given that delirium is often treatable, early recognition and appropriate management of delirium may improve patient care and safety, although the specific role of these measures in suicide prevention remains unclear. Future research is required to clarify how delirium contributes to suicide risk and to support the development of effective preventive strategies for this vulnerable population. This study contributes to the limited literature on suicide deaths among hospitalized patients with delirium by describing their clinical characteristics and the circumstances surrounding these events.
Footnotes
Ethical Considerations
This study used anonymized data that are publicly available online; therefore, formal ethical approval was not required.
Author Contributions
Keisuke Inoue: Conceptualization, Writing – review & editing, Writing – original draft, Data curation. Yoshinori Cho: Conceptualization, Writing – review & editing. Kotaro Otsuka: Conceptualization, Writing – review & editing. Hideki Onishi: Conceptualization, Writing – review & editing. Chiaki Kawanishi: Conceptualization, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, Keisuke Inoue, upon reasonable request.