
Abstract
This study aimed to examine the determinants of life satisfaction of older adults in Turkey. The sample consisted of 2,959 older adults over 65 years. The effects of psychological, daily life and instrumental activity, physical health and health status, and other important variables on life satisfaction were analyzed. The variables lessening life satisfaction for older adults included poverty, a lower self-reported health status, a decline in physical health, ability to chew, ability to do household activities, and an increase in feelings of depression and feeling social withdrawn. In contrast, being married, having a higher education level, and having an income-generating work increased life satisfaction among older adults. This study suggests the necessity of developing local and national policies that enable older adults to become more active in their communities. These policies should be coordinated under the framework of national aging policies that bridge health, social, and economic issues.
Introduction
The world’s older adult population has been increasing rapidly. Their numbers have increased from 418 million in 2000 to 588 million in 2014, an annual increase of 2.4% over the past 14 years although the global rate of population growth has declined to 1.2% (The World Bank, 2016). Turkey, similar to the rest of the world, has been experiencing a gradual increase in its older adult population (age 65 and over) in the past few decades. According to the offical statistics, the number of older people reached 6.651.503 (8.3% of total population) in 2016, up from 3.9 million (5.7%) in 2000 (Turkish Statistical Institute [TUIK], 2016a, 2017), and average life expectancy at birth has increased to 78 years (75.3 years in males and 80.7 years in females; TUIK, 2016b).
Greater life expectancy, almost by definition, is associated with an increasing number of older adults in the population, and, thus, they face changes in social networks, socioeconomic, health-related, and demographic conditions. These changes that older people experience affect their life satisfaction and quality of life unless society addresses the concerns in an effective manner (Altinparmak, 2009; Bilgili & Arpaci, 2014; Borg, Hallberg, & Blomqvist, 2006; Pinto & Neri, 2013). There is a tendency to link increasing age with decreased life satisfaction and quality of life brought on by physical and psychological disabilities, chronic diseases, and social and financial problems/loses often witnessed with old age (Bilgili & Arpaci, 2014; Celik, Kapucu, Tuna, & Akkus, 2010; Chen, 2001; Fernández-Ballesteros, Zamarrón, & Ruiz, 2001).
Veenhoven asks, “how much one likes the life one lives, or more formally, the degree to which one evaluates one’s life-as-a-whole positively” and then mentions this question is differently answered in three theories linked to different theories about how we evaluate life. He states set point theory focuses more on the mental processes that maintain a stable attitude toward life than on the processes that have brought it about, while comparison theory sees life satisfaction evaluation rather as a continuous judgment process involving the comparison of perceptions of life as it is with notions of how life should be. He explains affect theory sees happiness as a continuous mental process and a reflection of how well a person feels generally. According to affect theory, gratification of needs has a special importance in feeling good or bad. Veenhoven also arises the question “whether these theories adequately reflect reality or not” (Veenhoven, 2009). As Veenhoven states, life satisfaction and quality of life are general, broad, difficult to measure, and multidimensional concepts and define a person’s subjective satisfaction or happiness with his or her life and health. Aspects of importance to both life satisfaction and quality of life are cognitive, subjective, and objective domains such as psychological well-being, symptoms/outlook, physical health, occupation, social relations, financial status, and the ability to perform activities of daily living. Life satisfaction and quality of life also depend on an individual’s adaptation process, perception of their position in life within the context of the culture and the value systems they hold and how these relate to their goals, expectations, standards, and concerns (Arun & Cakiroglu, 2013; Bowen et al., 2015; Campos, Ferreira, Vargas, & Albala, 2014; Diener, Inglehart, & Tay, 2013; Fernández-Ballesteros et al., 2001; Kim, 2013; Maher, Pincus, Ram, & Conroy, 2015; McNamee & Mendolia, 2014; Mollaoglu, Tuncay, & Fertelli, 2010; Netuveli, Wiggins, Hildon, Montgomery, & Blane, 2006; Oishi, Diener, Lucas, & Suh, 1999; Renwick et al., 2015; Rosengren, Jonasson, Brogardh, & Lexell, 2015; Rouch et al., 2014; Seib et al., 2014; van Leeuwen et al., 2012; WHOQOL Group, 1995; Yamada, Merz, & Kisvetrova, 2015).
Considering these aspects of life satisfaction, many studies have concluded that subjective well-being is a theoretical construct that encompasses a person’s emotions, affect, and feelings, psychological state (positive functioning), social relations with others, and spiritual beliefs to include a sense of purpose in life (Hyde, Wiggins, Higgs, & Blane, 2003; Lindert, Bain, Kubzansky, & Stein, 2015; Meadow, Mentzer, Rahtz, & Sirgy, 1992; Oishi et al., 1999). Furthermore, studies about life satisfaction have been conducted among diverse population subgroups. Some studies have measured life satisfaction among people with certain diseases (Bowen et al., 2015; Renwick et al., 2015; Rosengren et al., 2015; van Leeuwen et al., 2012). Others have been conducted in the general population, or among people who are older, in disadvantaged groups (Banjare, Dwivedi, & Pradhan, 2015; Gregersen, Jordansen, & Gerritsen, 2015; Joshanloo, 2016; Kobayashi et al., 2015; Maher et al., 2015; Mollaoglu, Tuncay, & Fertelli, 2010), or in different health-care settings (Wilson, 2012), and countries (Oishi et al., 1999). Therefore, more studies that focus on the relationship between aging and life satisfaction and the factors including psychological and physical, social, demographic, and economic variables that influence or determine life satisfaction are needed.
Maslow’s need gratification theory of well-being might be useful in examining more likely predictors of life satisfaction because this theory assumes higher need gratification produces more profound happiness than lower need gratification. According to Maslow’s need gratification theory, (a) people in wealthier nations tend to be more satisfied with their lives and (b) people in wealthier nations tend to base their life satisfaction judgments on the level of gratification of higher needs. People in poorer nations should tend to base their life satisfaction judgments on the level of gratification of more basic needs. When we think of life satisfaction as the level of achieving the goals that the individual has drawn to him or her, there may be enough satisfaction about one’s self-fulfillment, and this also is directly proportional to life satisfaction. Maslow’s theory in psychology comprises a five-tier model of human needs (physiological, safety-security, belongingness, esteem, and self-actualization). In this theory, people are motivated to achieve certain needs and that some needs take precedence over others. One must satisfy lower level deficit needs before progressing on to meet higher level growth needs. Once these growth needs have been reasonably satisfied, one may be able to reach the highest level called self-actualization. Therefore, life satisfaction is not handled in a one-sided dimension, and that is why it is a general assessment of an individual’s life (McLeod, 2017; Oishi et al., 1999).
Determinants of a global sense of satisfaction with life might be very different. There are better clues to well-being come from knowing about a person’s traits, close relationships, work experiences, culture, and religiosity (Myers & Diener, 1995). “What predicts people’s life satisfaction?” In aswering this question, Oishi and his colleagues mentioned various demographic and personality variables, ranging from income, education, and marital status to personality variables such as self-esteem, optimism, and frequent positive emotional experiences. They also discuss that standards for life satisfaction judgments vary across cultures (Oishi et al., 1999). Abu-Bader and his colleagues grouped the factors influencing life satisfaction as environmental characteristics, such as the availability of social support, and personal traits, such as self-esteem, physical health, financial resources, a sense of connectedness, and locus of control (Abu-Bader, Rogers, & Barusch, 2002).
The choice of a measurement tool as well as significant determinants of life satisfaction depends heavily on the research question being addressed. The measurement of life satisfaction requires thoughtful consideration of national and international health-care policies and what decisions are relevant for the country/region being analyzed. Therefore, epidemiological population-based studies are important for identifying the determinants and etiological factors associated with aging and life satisfaction among aged populations. Traditionally, Turkish people view older adults as a source of wisdom and guidance based on their varied life experiences. Religious and cultural norms and traditions also encourage and support the contributions made to society by older people. Furthermore, older people usually remain with their children and other family members until death with care usually being given by the family no matter how seriously ill or disabled their aged relative may be. Feelings of guilt prevent most people from moving their aged parents to a nursing home or other such aged care facility, even though they believe that their parents may be given better care there (Celik et al., 2010). Nevertheless, Turkish society has undergone many social changes in recent decades. More women are now working outside the home, and the development of the nuclear family has impacted people’s attitudes toward older people. These developments are expected to have a serious effect on the life satisfaction of older people in Turkey. For this reason, this study aimed to measure and determine the life satisfaction predictors among the older population in Turkey. The results of this study have the potential to shape more appropriate health and social care policies that are more relevant to Turkey and its older population in the future and to improve life satisfaction among older adult population groups in Turkey.
Methods
Data and Study Population
The principal aim of this study was to measure and examine the determinants of life satisfaction among older adults who were over 65 years old in Turkey. The 2012 Turkey Health Survey (THS), a large and nationally representative survey, was the source of data for this study. This survey collected data on many health indicators and use of health services from over 33,000 individuals living in 14,400 households (TUIK, 2012). As the present study focuses on older adults, only those who were over 65 years old in the survey data were selected and included in this study. The selected data compiled information from 3,396 older adults, and after excluding 437 cases with missing values, the final sample was 2,959.
Sociodemographic and Economic Characteristics of Older Adults (N = 2,959).
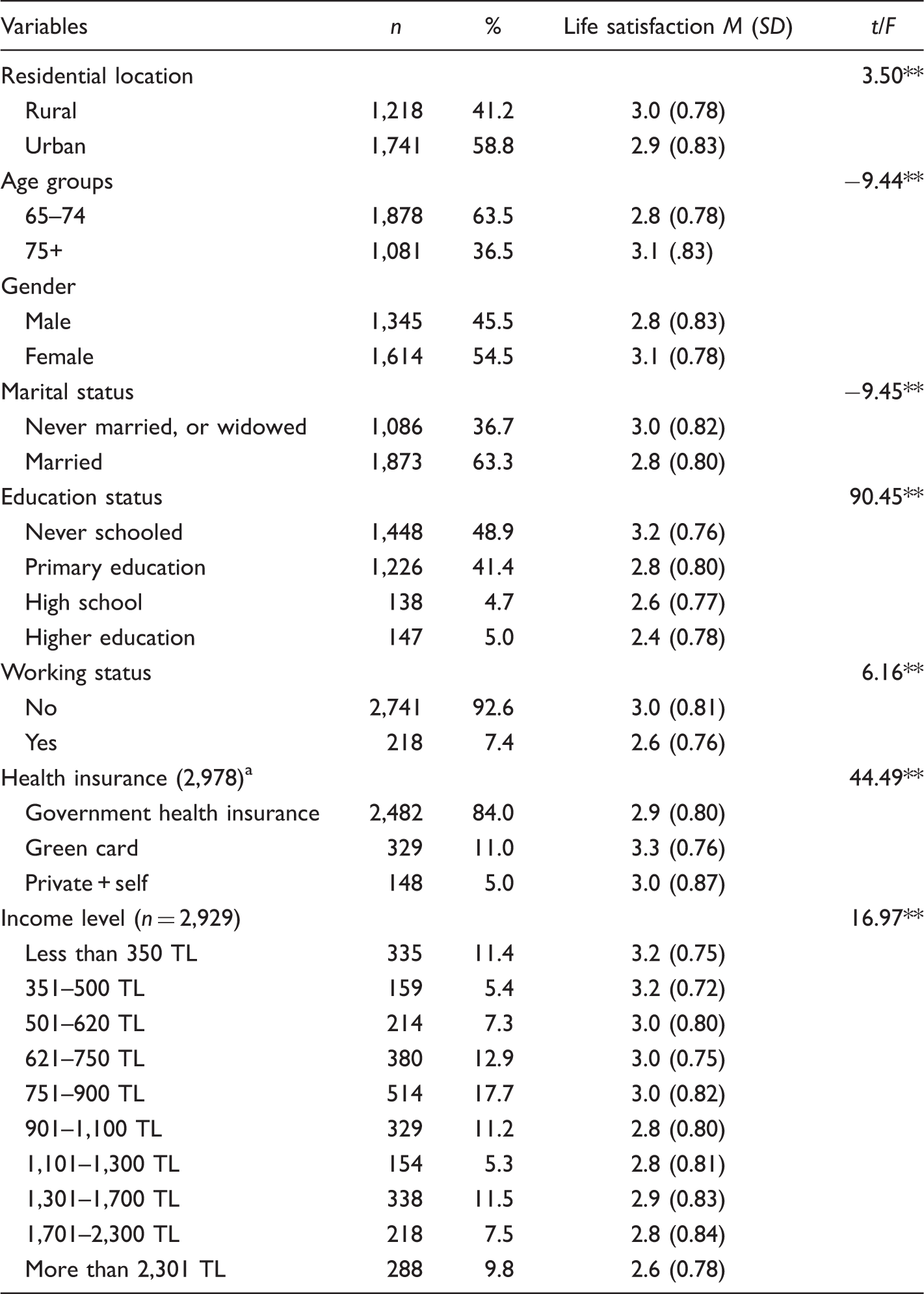
Some older adults have more than one type of health insurance.
p < .05.
Health Status of Older Adults (N = 2,959).
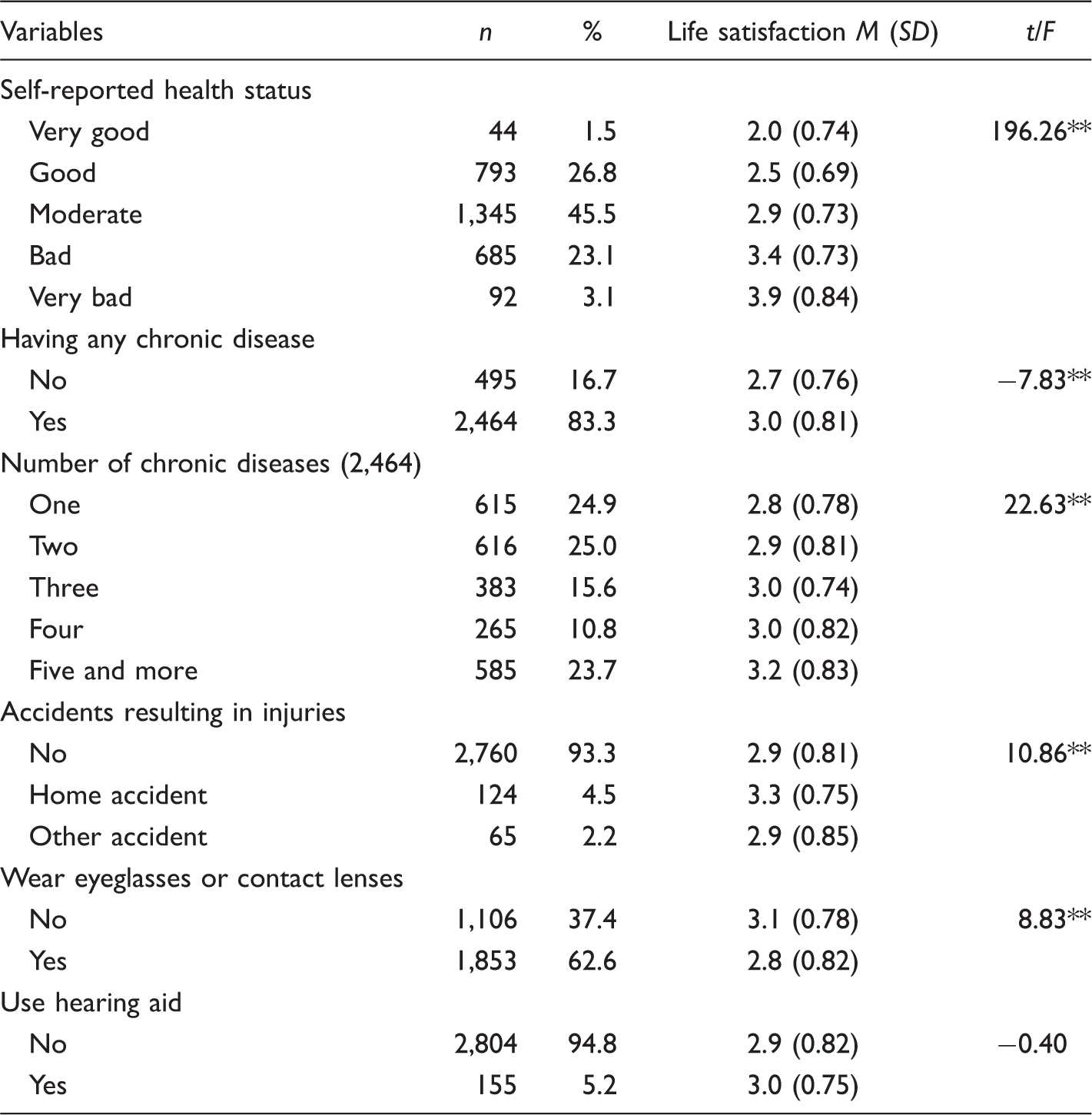
p < .05.
Study Variables
Derived and Measured Variables in the Study and Factor Analyses Results.
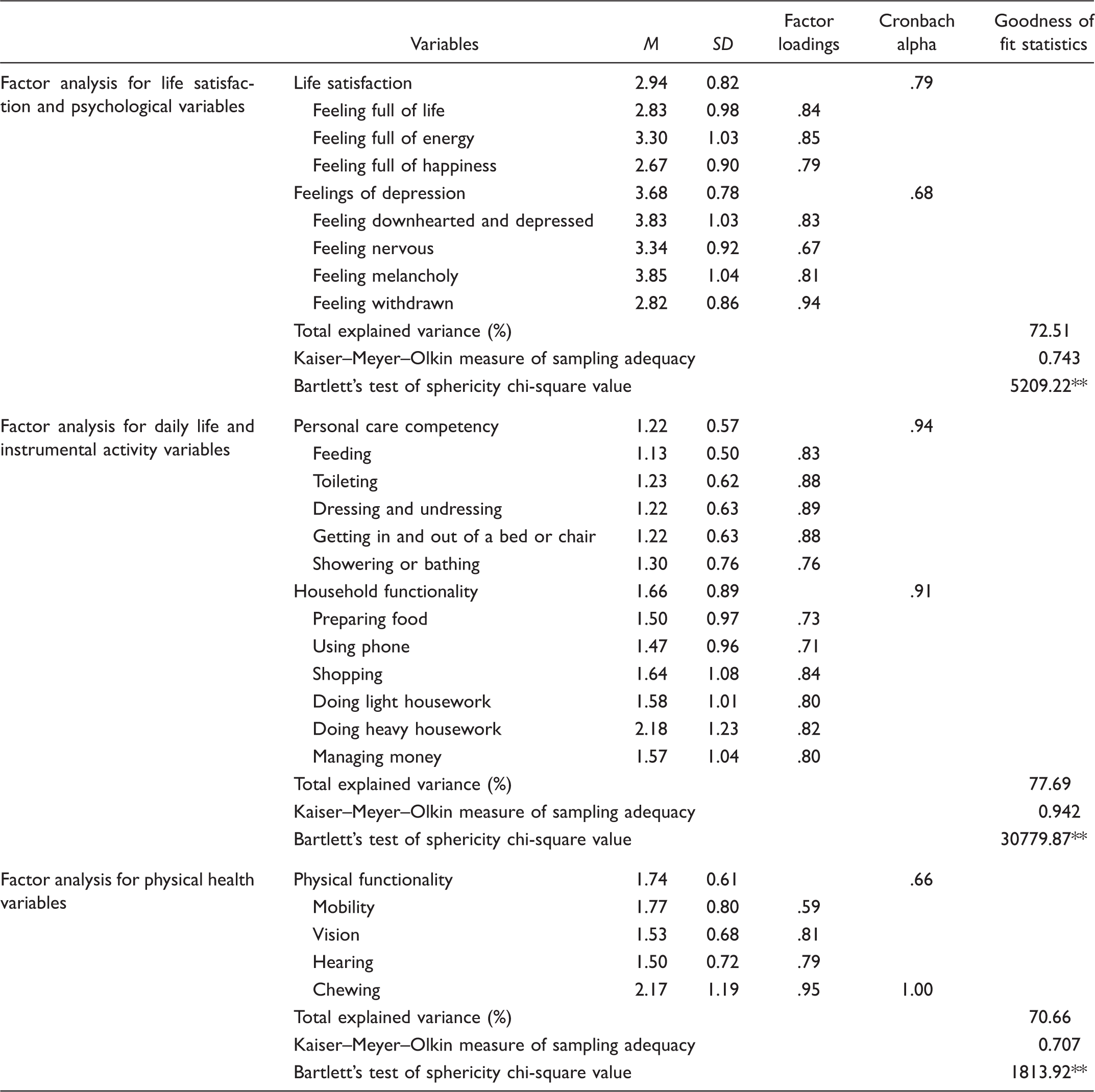
p < .05.
Independent variables that were more likely to affect life satisfaction were determined based on a literature review (Arun & Cakiroglu, 2013; Bowen et al., 2015; Hyde et al., 2003; Lindert et al., 2015; Maher et al., 2015; McNamee & Mendolia, 2014; Meadow et al., 1992; Mollaoglu et al., 2010; Netuveli et al., 2006; Oishi et al., 1999; Rouch et al., 2014; Seib et al., 2014; Yamada et al., 2015) and grouped under five categories: (a) Psychological variables measured feeling depressed and social withdrawn; (b) Daily life and instrumental variables measured functionality in personal care and household activities; (c) Physical health variables measured physical health functionality and chewing ability; (d) the Social, demographic, and economic characteristics of older adults, and (e) Health status variables.
Psychological variables: Two variables (feeling depressed and social withdrawn) under this category were derived from the psychological discomfort section in the data. Psychological discomfort was measured by asking respondents how frequently they had experienced specific feelings and concerns in the past 4 weeks, using a 5-point scale (1 indicated experiencing the feeling always and 5 indicated never). The variable called “feeling of depression” was derived from three variables measuring the feelings of downhearted, depressed, nervous, and melancholy, while a single variable was used to measure the feeling of social withdrawn. Higher scores in these variables imply fewer feelings of being depressed and social withdrawn (Table 3). Daily life and instrumental activity variables: THS included many variables to assess the ability of a respondent to do their daily life and instrumental activities. The variables measuring the functionality in doing daily life and instrumental activities might be grouped under two main categories: personal care competency and household activities functionality. Personal care competency was defined as the ability to do daily personal care activities such as feeding or dressing/undressing, while household activities functionality was thought to be a composite function of the ability to perform daily household tasks such as preparing food or shopping. Personal care competency and household activities functionality variables were measured on a 4-point scale (1: no difficulty; 4: serious difficulty; Table 3). Physical health variables: Physical health was defined with respect to vision, mobility, hearing, and chewing. The ability scores on four different physical health variables ranged from 1 (no problem at all) to 4 (serious problem), with a lower average score indicating better physical health. However, each physical ability was measured using a different number of variables. For instance, vision and mobility were measured with more than one variable, while hearing and chewing abilities were measured with only one variable. To equalize the distribution of data points across the measures of physical health, we created two new composite variables for vision and mobility by calculating the mean responses to vision and mobility variables. Then, these four variables were entered to factor analysis, and the results indicated that vision, mobility, and hearing abilities might be grouped under a single factor named “physical functionality,” while chewing ability was considered a separate factor (Table 3). Social, demographic, and economic variables: Age, gender, marital status, and health status of respondents were demographic variables, while residential area, income and education level, and working in an income-generating activity were social and economic variables. Health status variables: There are a number of variables describing health status of older adults in THS. However, six different variables were selected, and descriptive findings on these variables were provided in Table 2 for better understanding of health status of older adults in this study.
Data Analysis
Frequency, percentage, and mean calculations were used to describe variables. Principal components exploratory factor analysis with varimax rotation was used to construct the variables of “life satisfaction” and “psychological, physical health and daily life/instrumental activity variables.” The correlation matrix was computed first, and Kaiser–Meyer–Olkin’s measure of sampling adequacy and Bartlett’s test of sphericity were calculated to verify the appropriateness of using factor models. It is recommended that the Kaiser–Meyer–Olkin value should be higher than 0.50, and the chi-square value calculated for Bartlett’s test of sphericity is statistically significant (Field, 2009; Sharma, 1996). Eigen values that were equal or bigger than 1 were considered to determine the number of factors. Then, bivariate correlation coefficients and standard multiple regression analysis were used to estimate the relationship among variables and to predict the effects of social, demographic, and economic variables as well as psychological, physical health, and daily life/instrumental variables on life satisfaction. The t test for independent samples and analysis of variance were also used to test whether life satisfaction differed according to demographic and economic characteristics of older adults.
Ethical Considerations
The Turkish Health Survey 2012 was used with the permission of the TUIK.
Results
Descriptive Findings
The summary statistics on sociodemographic and economic characteristics and health status of respondents were provided in Tables 1 and 2. The mean life satisfaction associated with each independent variable is also reported in these tables. With the exception of the life satisfaction scores of the users and nonusers of hearing aids, all other life satisfaction scores of the respondents’ sociodemographic and economic characteristics were found to be statistically different (p < .05). The mean life satisfaction scores were found to be lower (indicating higher life satisfaction) among those who were residing in urban areas, less than 75 years old, male, married, with higher education, working in any income-generating job, covered by health insurance, and having relatively higher income (Table 1).
The results indicated that better health status was related to higher life satisfaction because the mean life satisfaction scores were better among those with relatively better self-reported health status, no chronic disease, and no home accident. Older adults who had eyeglasses or contact lenses and did not need hearing aids also reported higher life satisfaction (Table 2).
Findings on Factor Analyses
A factor analysis run for the nine variables in the physical and psychological discomfort section produced nine first-order factors that were integrated into three second-order factors. The results indicated that two of nine variables in the physical and psychological discomfort section (feeling worn out and feeling tired) crossloaded with more than one factor. Thus, these two items were dropped from the analysis as the retained factors had strong (.60 or better) loadings on each of the factors (Costello & Osborne, 2005), and a new factor analysis was run. The new results also showed that physical and psychological discomfort variables might be grouped under three factors that could also be named as (a) Life satisfaction was derived from the three variables of “feelings of full of life, energy, and happiness,” (b) Feeling of depression was derived from the three variables of “feeling downhearted and depressed, nervous, and melancholy,” and (c) Social withdrawn was derived from a single variable that was feeling withdrawn (Table 3).
The data met the criteria for the Kaiser–Meyer–Olkin measure of sampling adequacy (0.743) as well as Bartlett’s test of sphericity (χ2 = 5209.22, df = 21, p < .001). Cronbach’s alpha coefficients for derived life satisfaction and feeling of depression variables were found to be as high as .79 and .68, respectively. These findings indicated good internal consistency. The Cronbach’s alpha coefficient for a social withdrawn feeling was not calculated because a social withdrawn feeling was used as measured. Three factors accounted for 72.51% of the total variance (Table 3).
The mean life satisfaction score among older adults was found to be 2.94, which can be described as moderate. However, respondents stated that they felt highly depressed (
The functionality of older adults in doing their daily life and instrumental activities was measured separately via 11 variables. Rather than using all these variables as separate independent variables, the researchers agreed to construct variables. Employed factor analysis yielded two factors for 11 variables, and these were named as personal care competency and household functionality (Table 3). Goodness of fit statistics belonged to factor analysis for daily life, and instrumental activity variables indicated the data met the criteria for the Kaiser–Meyer–Olkin measurement of sampling adequacy (0.942) as well as Bartlett’s test of sphericity (χ2 = 30779.87, df = 55, p < .001). The Cronbach’s alpha coefficients for personal care competency and household functionality were .94 and .91, respectively. These coefficients indicated good internal consistency. Two factors accounted for 77.69% of the total variance (Table 3).
The means of personal care competency and household functionality suggested that respondents, in general, did not face much difficulty in doing daily personal care activities (
The third factor analysis run for four variables measuring the physical health of older adults produced two factors: physical functionality and chewing. Three of four variables measuring mobility, vision, and hearing ability were grouped under one factor, while chewing ability that might be an indicator of oral health was found to be as a separate factor. According to goodness of fit statistics, the data met the criteria for the Kaiser–Meyer–Olkin measure of sampling adequacy (0.707) as well as Bartlett’s test of sphericity (χ2 = 1813.92, df = 6, p < .001). The Cronbach’s alpha coefficient for physical functionality was .66, indicating moderate internal consistency. The Cronbach’s alpha coefficient for chewing ability was not calculated because this ability was used as measured in the data. Two factors accounted for 70.66% of the total variance (Table 3).
The mean of physical functionality was found to be 1.74 (± 0.61), suggesting that respondents faced some difficulties in their physical health. The findings also suggested that older adults had witnessed more serious problems with their chewing ability (2.17 ± 0.95; Table 3).
Results of Correlation and Multiple Regression Analyses
Correlation Coefficients Among Variables.
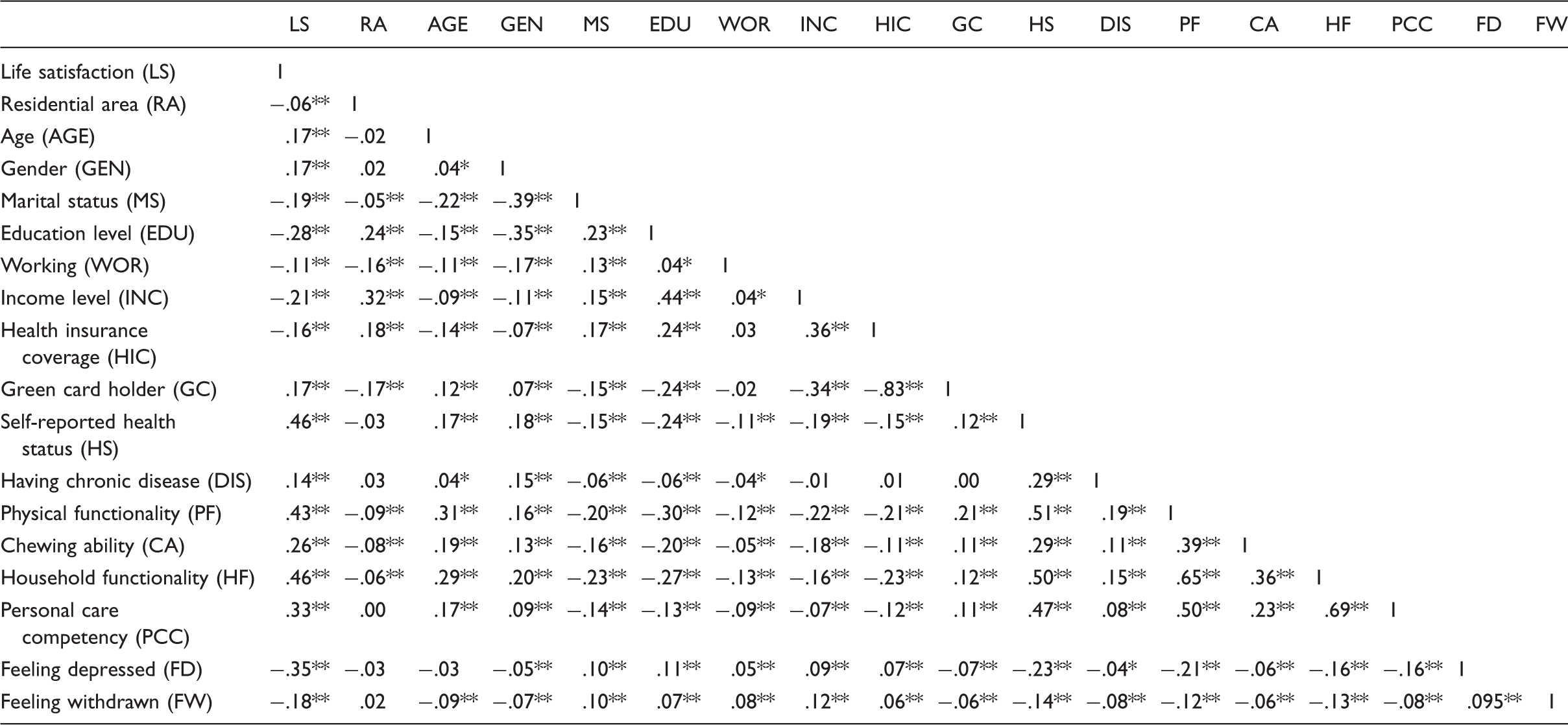
p < .01. *p < .05.
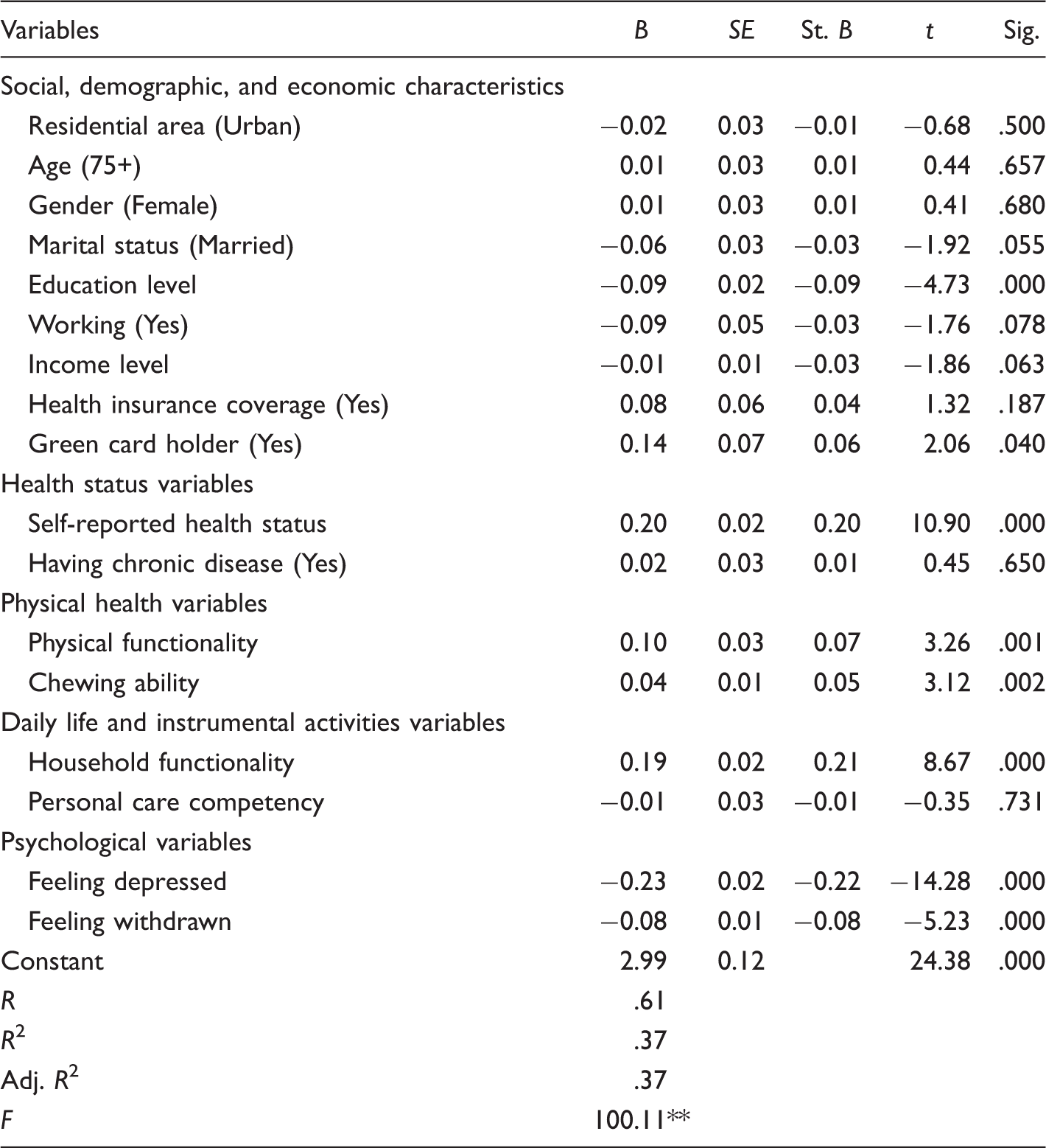
Results of Multiple Regression on the Determinants of Life Satisfaction of Older Adults.
p < .05.
Discussion
According to the results of this study, life satisfaction of older adults in Turkey can be described as moderate because the mean life satisfaction score (
In this study, the effects of health status on life satisfaction were estimated by using variables measuring different aspects of health to determine any relationship between health status and life satisfaction among older adults. Feelings of depression and feeling social withdrawn were found to be relatively high among the respondents in this study. However, personal care competency and household functionality were found to be somewhat better (Table 3). In addition, the results showed that being covered by a green card, having worse self-reported health status, lower physical functionality, and greater feelings of depression and social withdrawn were significant factors that lessened life satisfaction (Table 5). These results are consistent with other studies on the determinants of life satisfaction among older adults (Altay & Avcı, 2009; Banjare et al., 2015; Borg et al., 2006; Efklides, Kalaitzidou, & Chankin, 2003; Melendez, Tomas, Oliver, & Navarro, 2009; Onishi et al., 2010; Pinto & Neri, 2013; Zhang & Liu, 2007). A significant negative effect on life satisfaction was discovered for study participants who were covered by the green card program, a program for those living below the poverty level in Turkey. This finding suggests a close and expected relationship between life satisfaction and poverty.
In previous studies (Banjare et al., 2015; Katz, 2009; Melendez et al., 2009; Pinto & Neri, 2013), physical activity has usually been found to be an important determinant of life satisfaction among older adults. Maintaining their physical functions increases the capacity of an older person to move independently, doing daily life activities such as toileting, clothing, using the phone, shopping, and performing other personal care and household activities. Fulfilling these functions independently indicates autonomy, which is always reflected in the older person’s life satisfaction (Borg et al., 2006; Melendez et al., 2009; Onishi et al., 2010; Subasi & Hayran, 2005). Our study also showed better physical functionality was among the most significant determinants of better life satisfaction (Table 5).
Based on the literature, one can conclude that there is a close relationship between good physical health and higher life satisfaction. A study by Pinto and Neri (2013) found that functional performance, including low handgrip strength and low gait speed were statistically associated with lower life satisfaction. Another study found that an individual’s physical ability/disability including vision, hearing, walking, chewing, speech, and memory are important factors that influence life satisfaction for both males and females (Banjare et al., 2015). Our results showed that better physical functionality, chewing ability, and household functionality (meaning older adults did not have difficulty in doing their daily activities and household work as well as having better dental health) had a significantly positive effect on life satisfaction. The results of regression analysis indicated that the bivariate significant relationship (Table 4) diminished when the effects of all other independent variables were considered because the regression results did not reveal a statistically significant effect of better personal care functionality on higher life satisfaction (Table 5). All results related to the effect of physical health on life satisfaction were as expected and consistent with the relevant literature.
The positive relationship between better psychological health and life satisfaction is also well known. Psychological health is generally related to overall subjective well-being. Feeling worthless, tired, exhausted, powerless, lonely, useless, and losing one’s functions, as well as being brokenhearted, depressed, angry, anxious, and melancholy, are, in themselves, major indicators of psychological or mental discomfort. These are major obstacles that can negatively affect the life satisfaction of older adults. Physical health such as the ability to do daily living activities and socioeconomic factors such as education level or poverty are also important influences on psychological health. Problems in these areas may cause psychological or mental discomfort such as depression and withdrawal (Banjare et al., 2015; Borg et al., 2006; Gregersen et al., 2015; Joshanloo, 2016; Zhang & Liu, 2007). The results on constructed variables measuring psychological health of older adults revealed that increased feelings of withdrawal and depression decreased the level of life satisfaction (Table 5). This finding was supported by the findings of other studies showing a significant relationship between better psychological health and better life satisfaction (Borg et al., 2006; Efklides et al., 2003; Onishi et al., 2010; Zhang & Liu, 2007).
Many studies have found a significant relationship between life satisfaction and social, demographic, and economic characteristics of older people (Chen, 2001; Fernández-Ballesteros et al., 2001). An especially common finding that reflects better life satisfaction is the positive effect of a higher level of education and being married (Johnson, Pitt-Catsouphes, Besen, Smyer, & Matz-Costa, 2008; Melendez et al., 2009; Oshio, 2012; Subasi & Hayran, 2005). A higher education level is expected to have a positive effect on life satisfaction because people with a higher education also tend to have a better social-relations network, self-confidence, and living conditions. Older married couples experience an especially high level of satisfaction because they are able to support one another. All these factors positively affect older people’s psychological and emotional health status, hence their life satisfaction. The present study also revealed consistent findings with the relevant literature by showing greater life satisfaction in older adults with higher education levels and those who were married (Table 5).
Although this study indicated that life satisfaction might be related to some sociodemographic characteristics (Table 1), other studies in Turkey and elsewhere have suggested that these factors might not have an effect on the life satisfaction of older adults (Altay & Avcı, 2009; Altinparmak, 2009; Banjare et al., 2015; Joseph et al., 2014; Melendez et al., 2009; Subasi & Hayran, 2005). In addition to these findings, age, residential area, gender, working in an income-generating career, and income level were social, demographic, and economic characteristics whose effects on life satisfaction were found to be statistically nonsignificant according to regression analysis results (Table 5). Yet, the results on correlation coefficients provided in Table 4 suggested that there was a statistically significant relationship between life satisfaction and social, demographic, and the economic characteristics of older adults.
Conclusion
There are many published as well as new emerging studies in the related literature about the life satisfaction of older adults. However, the number of studies aiming to examine life satisfaction and its determinants among older people in Turkey is limited. This study, using data that are nationally representative, revealed that life satisfaction among older people was affected by a number of social, health, and economic characteristics. The results of this study will contribute to the debate concerning the expected and unexpected relationships between life satisfaction and many predictors among older people. The findings also emphasize the necessity of developing ways to increase the life satisfaction of older people by focusing on their health-care needs as well as other social, physical, and psychological needs.
It is likely that the increasing older population in Turkey will impose more financial, social, and health burdens in coming years. Before the negative effects of these factors impact Turkey’s older adult population, social and health policy makers should become engaged in making vital decisions that will lessen the likely social, health, and financial consequences and improve the life satisfaction of older adults.
Based on the findings of this current study, the following recommendations are suggested to improve the life satisfaction of Turkey’s older adults in the future:
Develop local and national policies enabling older adults to become active in their communities. These policies should be coordinated under the framework of national aging policies that bridge health, social, and economic policies and must be updated to adapt to changing conditions and policies. Provide health and social services for older adults who can no longer carry out the activities of daily living due to their diminishing functional capabilities. Local and government institutions, and families and relatives, should be seen as an important part of these services. Lessen the burden of poverty on older adults with lower income levels by providing social and health-care services coordinated by government and nongovernment agencies at the national and local levels. Develop overall policies based on the concept: aging in their own environment with the goal of healthy aging and increased life satisfaction among older adults.
Limitations of the Study and Recommendations for Further Research
This study has mainly four limitations. First, the study was a retrospective one, with the usual limitations of inaccurate recall of past events and possible contamination by current events. Second, results of this study cannot be generalized to all older people in Turkey. Third, it does not allow to make causal inferences because this study design is cross-sectional in nature. Fourth, although this study used a nationally representative and a rich data set allowing the researchers to test the effects of different social, demographic, and economic variables including individual- and some community-level factors on life satisfaction, it was not able to test the effects of social and health policy-related measures such as financial or aids in kind that had been directed to older adults in need. It is recommended that researches in the future be conducted to examine the effects of policy-related measures to increase life satisfaction and to find the root causes of problems that are more likely to decrease life satisfaction of older adults.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.