
Abstract
Objectives
This study examines the effects of frequency of visits, monetary, and in-kind support provided to older parents on the depressive symptoms of adult children.
Method
This study drew secondary data from the China Health and Retirement Longitudinal Study Follow-up Questionnaire. A total of 629 older children aged 55 years and older (M = 59.80, standard deviation = 3.90) met the inclusion criteria. The dependent variable—depressive symptoms—was measured with the Center for Epidemiological Studies Depression scale.
Results
Approximately 22% of participants reported clinically significant levels of depressive symptoms. Hierarchical regression analyses found that more frequent visits and monetary support to older parents were related to lower levels of depressive symptoms in older children.
Conclusion
Providing monetary support to parents may help mitigate a major concern of parents: health-care costs. Older children’s altruistic behaviors meet legal and cultural expectations in Chinese society, contributing to family intimacy and thereby their own mental health outcomes.
The number of Chinese older adults aged 60 years or older reached over 200 million, accounting for 15.6% of the total Chinese population in 2014; the number will reach 434 million and make up 31% by 2050 (Zhu & Fan, 2017). With the prolonged life expectancy, and limited availability of family caregivers in contemporary China due to China’s One-Child Policy (Zhang & Goza, 2006), older adults tend to live longer in “empty-nest households” and face risks of chronic diseases alone (Pan, Jones, & Pothier, 2017). Taking care of older parents is expected in traditional Chinese culture due to the value of filial piety. It remains largely unchanged and shapes intergenerational relationship (Z. Lin & Pei, 2016). Adult children are expected to be primary caregivers no less than spouses (Chappell & Kusch, 2007). Although faced with challenges due to failing physical strength and cognitive ability in the old age, adult children who entered the old age themselves (i.e., the young old) must take the responsibility of providing support to their old parents (the old-old group) to meet these cultural expectations. Moreover, functional limitations of the old-old group—the possible loss of spouses and the shortage of formal aging services in mainland China—can result in the old-old group relying heavily on the instrumental, economic, or emotional support provided by their children who are young-old. This reliance may be accentuated in rural China where filial piety values are more prevalent and aging service resources are less available (Cong & Silverstein, 2008).
Literature on parent–children bond has largely focused on whether receiving support from adult children would affect the well-being of older adults (X. Chen & Silverstein, 2000; Cong & Silverstein, 2008). However, little research has examined Chinese adult children who are approaching old age and tasked with providing support to their parents. The young-old group may provide majority of support to the frail old-old group, which is the fastest growing subpopulation in China. The number of the old-old group (aged 80 years or older) was 24 million in 2014, will double by 2030, and reach 108 million in 2050 (National Aging Office of China, 2016).
Supportive behaviors of older children benefit the old-old group and themselves by promoting balanced intergenerational relationships and adhering to cultural expectations. Moreover, the Elder Rights Protection Law (2013) in mainland China was recently revised to stipulate that adult children would face financial penalties if they failed to provide financial, emotional, and instrumental support to their older parents or fail to visit them frequently. This study only investigated older children with non-coresident older parents in China. Non-coresident parents receive less support from children than their coresident counterparts (Giles & Mu, 2007). In addition, 75.2% of married children do not coreside with their parents (Social Science Survey Center at Beijing University, 2012). The aim of this study is to identify whether providing support (frequency of visits and economic support) to non-coresident older parents would affect the level of depressive symptoms of Chinese older children.
Frequency of contact between older parents and children is often used as a proxy for intergenerational support (Mancini & Blieszner, 1989), which is believed to influence parents’ well-being. But some studies found that simple contacts with children had little influence on older parents’ psychological well-being in western countries (e.g., J. Lin, Chang, & Huang, 2011; Mancini & Blieszner, 1989). One possible explanation is that intergenerational support encompasses a quality of interaction that cannot be simplified as “two generations keeping in touch with one another” (J. Lin et al., 2011, p. 49). However, in this article, we kept the frequency of visits as a proxy for social support offered by adult children in line with Chinese cultural values. Visiting parents and its association with psychological well-being in older adult children has yet to be examined.
The effects of support from children on the well-being of Chinese older adults have been well-documented in the literature. Whether such effects are positive or not depended on several factors such as gender, coresidence status, type of support, and parents’ cultural appraisal of support (Cong & Silverstein, 2008). It is generally accepted that daughters undertake more caregiving responsibilities than sons (Laditka & Laditka, 2000). Daughters are more likely to help with parents’ activities of daily living (ADLs; Lee, Dwyer, & Coward, 1993) while sons are more likely to assist with instrumental activities of daily living (IADLs) or pay for home care services for parents (Couch, Daly, & Wolf, 1999). Unmarried adult children provide more support than married ones (Cong & Silverstein, 2008).
Regarding types of support, emotional support benefited the well-being of Chinese older adults, outweighing the effect of financial support (e.g., Krause, Liang, & Gu, 1998). However, findings about the effect of receiving instrumental support on the well-being of Chinese older adults are mixed. Receiving instrumental support was found to exert negative or no impact on older adults’ well-being, largely because instrumental assistance is associated with older adults’ loss of self-efficacy and power in the family system (X. Chen & Silverstein, 2000).
Researchers have noticed that older adults are more involved in providing support than receiving support (e.g., Sheppard, 1991). Providing emotional and instrumental support (e.g., meal preparation) to children (X. Chen & Silverstein, 2000; Silverman, Hecht, McMillin, & Chang, 2008) or others (Chao, 2011) had positive effects on Chinese older adults’ well-being (e.g., depression, morale). Providing physical support to children (Silverman et al., 2008) or others (Chao, 2011) has negative effects. Similarly, providing financial support to children had a negative influence (C. Chen, 2000; X. Chen & Silverstein, 2000). One reason is that many Chinese older adults have already transferred most of their assets to adult children; additional financial assistance to children may cause them financial and mental strain (C. Chen, 2000).
Empirical studies have examined the relationship between social support (particularly support received from/provided to adult children) and the well-being of older parents. But how providing support to older parents influences depressive symptoms of Chinese old adult children is not clear yet. The old adult children group deserves attention, because they may depend on their younger children for financial or daily assistance as they age. On the other side, their parents, the old-old group, may heavily rely on them, for meeting their long-term care needs.
Providing care to the old-old group may exhaust their older children’s financial resources and physical strengths, and take a toll on their mental health. But whether providing support to the old-old group has positive effects on older children’s life remains unclear. J. Lin et al. (2011) offered some insight into this issue. They posited that the provision of support to the old-old by the young-old group contributed to a balanced and reciprocal life within a three-generation family system (i.e., adult children, the young-old group, and the old-old group; J. Lin et al., 2011). The young-old group may be more or less likely rely on their children in China. Such reliance may make the young-old group feel dependent, resulting in negative effect on their mental health (e.g., Cong & Silverstein, 2008). For the “sandwich generation” (i.e., the young-old group), “feeling dependent” may be simply offset by “feeling needed.” Providing support to the old-old may help the young-old group regain power in their family and promote mutual trust and interdependence in the three-generation family. Moreover, older children may feel obligated to take care of their older parents, as expected by filial norms in China and mandated by Chinese law. Following Chinese law and fulfilling cultural expectations may have a positive effect on the mental health of the young-old group. Besides, the young-old group may also see themselves as role models (modeling the Confucian ideal of filial piety) for their young children and hope the latter would do the same when they reach old-old age. But the above propositions are not empirically tested. It is also necessary to distinguish the types of support young-old group provide and examine their respective effect on their mental health. By doing so, we may disentangle the complex relationship between the provision of support and mental health for the “sandwich generation.” In this article, we focused on the effect of frequency of visits and economic support to non-coresident older parents on the depressive symptoms of older children.
Altruism theory posits that providing support to older parents is a philanthropic endeavor that may benefit adult children (Grundy, 2005). The acts of giving could be interpreted “as reciprocation for past transfers from the parents or as transmission of a cultural value of intergenerational support” and are respected and valued by the cultural group (Grundy, 2005, p. 237). Therefore, benefiting older parents’ well-being may have positive repercussions for adult children’s well-being (De Jong Gierveld & Dykstra, 2008). These lines of reasoning suggest two hypotheses for this study of Chinese old adult children: (a) more visits to parents would be associated with lower levels of the depressive symptoms among older children and (b) providing monetary/in-kind support to parents would be associated with lower levels of depressive symptoms among older children.
Methods
This cross-sectional study used data from the China Health and Retirement Longitudinal Study (CHARLS) Follow-up Questionnaire. CHARLS is a nationally representative longitudinal survey of Chinese middle-aged and older adults (over 45 years of age) that is designed to provide insights into the aging population in China. CHARLS used multistep probability sampling strategy, selecting 450 rural/urban communities in 28 provinces according to geographic locations and gross domestic product per capita. A detailed description of the CHARLS is available elsewhere (e.g., Zhao, Hu, Smith, Strauss, & Yang, 2014). The CHARLS Follow-up Questionnaire was administered via face-to-face interviews (N = 13,169) between June 2011 and March 2012. The follow-up survey collected information on demographics, family structure, health status, health care, insurance, work, assets, and housing.
To be eligible for the present study, older children had to be aged 55 years and older and have at least one living parent who did not coreside with them at the time of survey. If both parents were alive at the time of interview, we randomly selected one for analysis. The application of these criteria resulted in a sample of 629 for the study.
Measures in CHARLS
Depressive Symptoms
The 10-item Center for Epidemiological Studies Depression scale was used to assess the dependent measure, level of depressive symptoms (Wolinsky et al., 2009). Respondents were asked to rate the frequency of depressive symptoms in the past week on a 4-point Likert-type scale, ranging from 1 (Rarely or none of the time) to 4 (Most or all of the time). The total possible scores range from 10 to 40 with higher scores indicating higher levels of depressive symptoms.
Social Support
Three dimensions of social support were assessed: frequency of visits, monetary support, and in-kind support (e.g., food, clothes) provided by older children to their non-coresident parents. Older children were asked to rate their frequency of visits to their parents on a scale running from 1 (almost never) to 9 (almost every day). Older children also indicated the total amount of monetary support and in-kind support (in Chinese Yuan) provided to parents in the past year. Both types of support were log-transformed (ln + 1) to approximate a normal distribution.
Control variables included known risk factors of depression such as health status and demographic traits (Cong & Silverstein, 2008). Health variables include parents’ general health status, older children’s self-rated health status, and physical functioning. Parent general health status was rated by respondents on a 5-point Likert-type scale ranging from 1 (poor) to 5 (excellent). Older children’s self-rated health was measured by a single question asking participates to indicate their health status on a similar 5-point scale (1 = poor, 5 = excellent).
Physical functioning was assessed with the 5-item ADL and the 6-item IADL (Lawton & Brody, 1969). Regarding the ADL, respondents were asked to indicate their difficulties in dressing, bathing, eating, getting (in/out of) bed, and using the toilet, using a 4-point rating scale (1 = No, I don’t have any difficulty, 4 = I cannot do it). Regarding the IADL, respondents are asked to indicate their difficulties of doing household chores, preparing hot meals, shopping for groceries, making phone calls, taking medications, and managing money, using the same 4-point scale. Higher scores on the ADL and IADL indicate more difficulties performing physical functioning.
Demographic traits included living proximity between non-coresident older parents and older children, parents’ age, education, and marital status. Living proximity was coded “1” if living in the same or an adjacent dwelling/courtyard or in the same village/neighborhood; otherwise, it was coded “0.” Older children’s age, gender, education, hukou status (household registration status in China), number of brothers, number of sisters, number of children, relative income, and marital status were assessed as well. Hukou status was dichotomously coded (1 = rural household residential status; 0 = urban household residential status).
Analytic Strategies
Analyses were run using the Statistical Package for the Social Sciences software, version 22.0. Descriptive analyses were conducted to determine the sample characteristics and the prevalence rate of depression among older children. As less than 5% of missing values were identified across study variables, listwise deletion method was used. Bivariate correlations were computed among variables of interest. Linear regression models were fitted to test the effects of the three types of provided social support provided on older children’s level of depressive symptoms, controlling health status, and demographic traits. We entered older children’s demographic traits in Model 1, older children’s health status in Model 2, parent-related variables in Model 3, and social support variables in Model 4.
Results
As illustrated in Table 1, older children’ average age was 59.80 years (standard deviation [SD] = 3.90). The mean respondent had approximately two brothers, two sisters, and two children. Approximately 40% of the sample was male, more than 80% were married, less than 1% had a college education, and less than 13% had poor health status. The majority reported rural hukou status (74.1%) and indicated their living standard was the same or better compared to their neighbors (68.8%).
Characteristics of Sample Participants (N = 629).
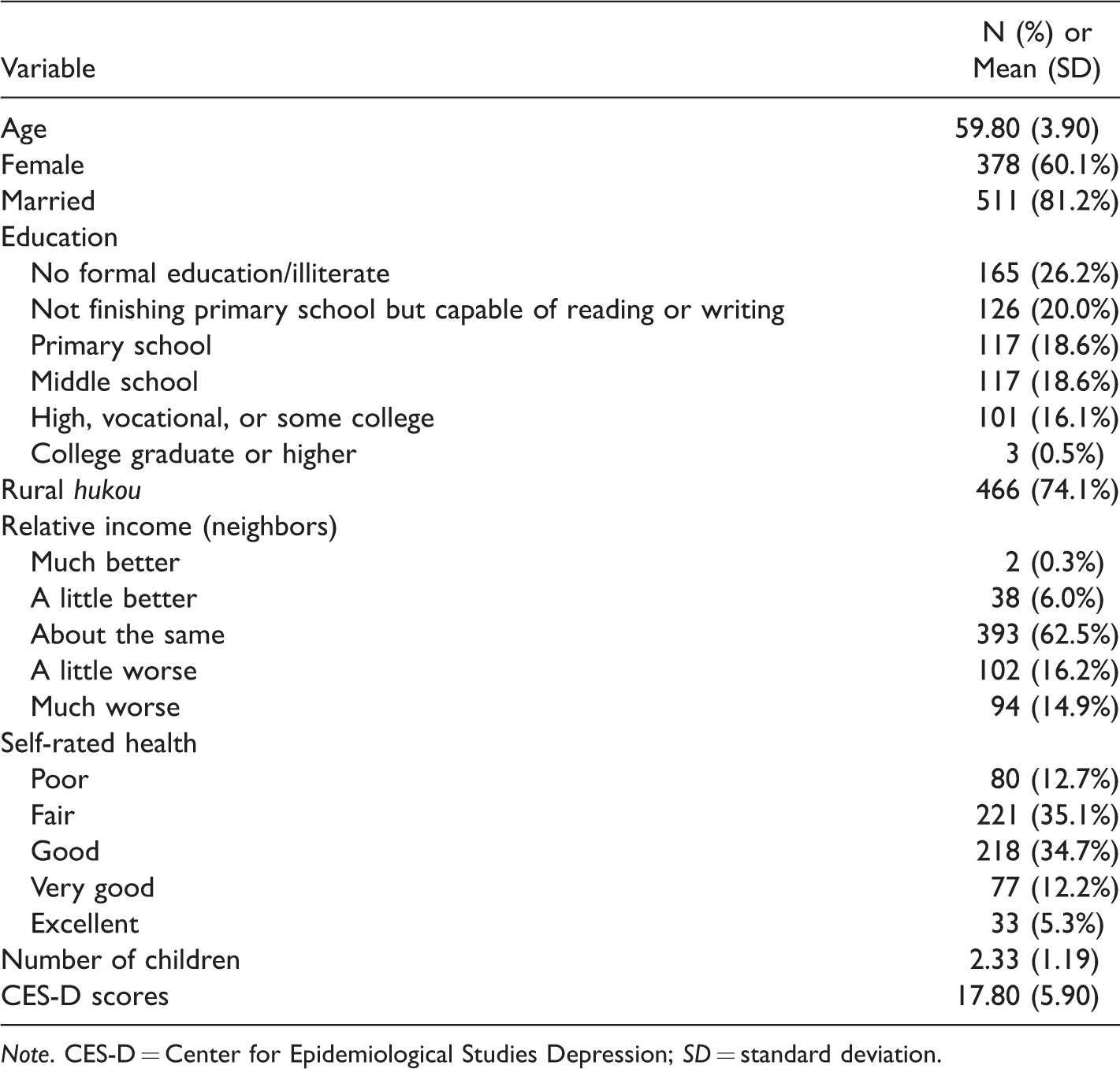
Note. CES-D = Center for Epidemiological Studies Depression; SD = standard deviation.
Respondent parents’ average age was 84.79 years (SD = 7.77). Regarding parents, 73% were widowed, 27% had poor health status, and less than 1% had a college education. About half of older children reported visiting their parents once a month, half provided no monetary support, and about 40% provided no in-kind support during the past year. On average, older children provided 553 Chinese Yuan (about 90 U.S. dollars) directly to older parents and 396 Yuan (about 64 U.S. dollars) in goods or services to older parents in the past year. About 22% of participants reported clinically significant levels of depressive symptoms using a cut-off score of 20 or higher.
Bivariate analyses indicated significant associations among the variables of interest. Depressive symptoms were positively associated with older children’s rural hukou (r = .12, p < .01), being female (r = .23, p < .01), lower levels of education (r = .19, p < .01), more children (r = .10, p < .01), being unmarried (r = .13, p < .01), more ADL difficulties (r = .14, p < .01), more IADL difficulties (r = .27, p < .01), poorer self-rated health (r = .36, p < .01), and relatively lower income (r = .29, p < .01). Depressive symptoms were also positively associated with parents’ lower levels of education (r = .05, p < .10) and poorer health status (r = .21, p < .01). Sons provided more monetary support than daughters (t = 4.18, p < .01). Providing less monetary support and in-kind support, along with less frequent visits to parents, were associated with more depressive symptoms among older children.
We constructed two-step linear regression models to test the two study hypotheses. Statistically significant control variables in the bivariate level were entered into regression models. Regression results (see Table 2) suggested that being female, younger age, lower levels of relative income, rural hukou, more IADL difficulties, and poorer self-rated health were related to more depressive symptoms among older children. Parents’ poorer health status was the only parent-related variable that was significantly related to depressive symptoms among older children. Frequency of visits to parents and providing monetary support were significantly related to the dependent measure in the final model.
Results of Hierarchical Multiple Regression Analysis.
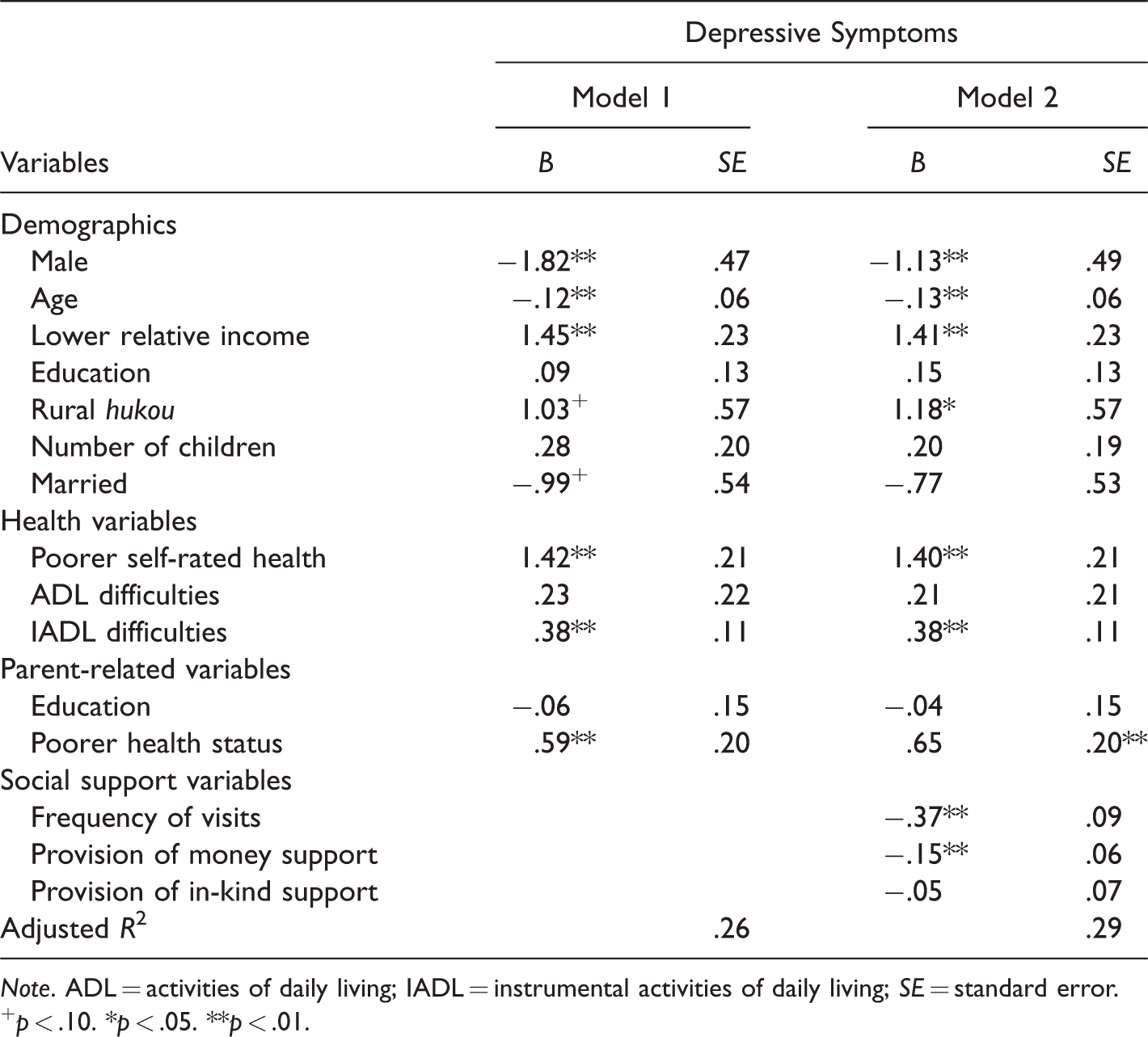
Note. ADL = activities of daily living; IADL = instrumental activities of daily living; SE = standard error.
+p < .10. *p < .05. **p < .01.
The final model, which controlled for potential confounding variables, yielded significant predictors of depression. Higher levels of visitation (B = −.37, SE = .09, p < .01) and monetary support (B = −.15, SE = .06, p < .05) were significantly associated with lower levels of depressive symptoms among older children. Providing more in-kind support was not associated with depressive symptoms. Adjusted R2 went up from 26% in the first model to 29% in the final model, which means the added three independent variables improved model power and explainability. Hypothesis 1 was supported while Hypothesis 2 was partially supported.
Discussion
In traditional Chinese culture, filial obligations fall heavily on the oldest son or the coresident son (Bian, Logan, & Bian, 1998). However, coresidence is no longer a dominant model of intergenerational support in contemporary China, as most married couples choose to live separately from parents (China Family Panel Studies, 2012). Thus, non-coresident support plays an increasingly important role in modern China. With the increased life expectancy in aging China, the young-old group is not merely the passive recipients of support from their own adult children but also the active providers of support to their old-old parents. Prior literature focused on the associations between social support (particularly support received from/provided to adult children) and the well-being of older parents, but overlooked the social support provided by older children to their parents and its ramifications for older children. This study addressed this literature gap by focusing on non-coresident Chinese older children.
The prevalence rate of depression among the young-old group in this study was 22%. This rate is similar to previous research conducted by Chou, Ho, and Chi (2006) with Chinese older adults, aged 60 years or older, using the Geriatric Depression Scale-Short Form (19.6% among those not living alone, 28.7% among those living alone). It is also close to the 20.8% rate obtained by Feng et al. (2013) among rural Chinese older adults, aged 60 years and older, using the same measurement. The target group in this study was older adults aged 55 years and older with a nonresident living parent. The uniqueness of this population, along with the differences in measurement and sampling, may help explain the relatively small discrepancies in reported prevalence rates.
Our first hypothesis was supported—more frequent visits to parents were significantly associated with lower levels of depressive symptoms among older children. This finding contradicts prior studies that found no significant relationship between visitation and depression among older adults in Western countries (e.g., J. Lin et al., 2011; Mancini & Blieszner, 1989). The Elder Rights Protection Law (2013) in China mandates that adult children visit their older parents. But in reality, this law is difficult to enforce. In practice, the statute likely acts more as a social cue, reminding adult children to take an active role in their parents’ lives. Accordingly, we suspect that this statute serves to reinforce filial cultural norms in a manner that functions to increase older children’s propensity to visit their parents. In turn, the sense that one is fulfilling legal and cultural norms may result in lower levels of depressive symptoms.
Another explanation can be drawn from the altruism theory. Older children’s altruistic behaviors are seen as reciprocations for past contributions by parents and such behaviors transmit the cultural value of intergenerational support (Grundy, 2005). Meeting cultural expectations, reciprocating parents’ earlier contributions, and transmitting the cultural value of intergenerational support may benefit the mental health of the young-old group. In addition, the social interactions associated with visitation help detect the emotional and instrumental needs of parents as well as facilitate mutual understanding. The resulting family intimacy may contribute to positive mental health outcomes among older adult children.
Our second hypothesis was partially supported. Providing monetary support to parents was associated with lower levels of depressive symptoms among older children. However, there was no relationship between the provision of in-kind support and depressive symptoms. Transferring money to their older parents meets the financial needs of older parents and has positive repercussions for adult children’s mental health. For many older parents, particularly in rural China, monetary support is the most needed type of support (Jin, Guo, & Feldman, 2015). In 2014, more than 23% of Chinese older adults (48,950,000) lived below the World Bank’s absolute poverty line (1.9 USD per day) and about 36% of rural Chinese older adults live below this line (Zhu & Fan, 2017). The poverty rate of the old-old group (aged 80 years and older) is about 10% higher than that of the young-old group (Zhu & Fan, 2017). The old-old group urgently needs monetary support to cover medical expenses. Researchers found that the health status of the old-old was worse than the young-old in rural China, but they used less medical resources because they simply cannot afford medical care (Feng et al., 2013). The old-old group had lower hospitalization rate and less inpatient/outpatient expenses than the young-old group (Yan & Chen, 2010). In other words, providing monetary support to the old-old group, instead of in-kind support, may address one of parents’ major concerns: health-care costs. Thus, older children may consider providing monetary support as an expression of filial piety and compliance with Chinese law. Such actions may benefit older children by fostering a decrease in their own depressive symptoms.
The second explanation is that providing in-kind support may have some influence on parents’ daily life, but its effects may be superseded by monetary support or frequent visits. For instance, some older parents can produce food by fishing, farming, or purchasing food with children’s monetary support. Some older children may provide in-kind support such as bringing fruits or gifts. However, such support is common in other social exchanges and may not engender as much as positive affect toward older children. This may explain the nonsignificant associations between in-kind support and older children’s depressive symptoms.
Older children’s IADL difficulties and lower levels of self-rated health were identified as correlates of depressive symptoms. This finding is consistent with previous studies that reported a positive association between physical health and mental health in China (L. W. Li, Liu, Xu, & Zhang, 2016) and other countries (Huang et al., 2010). Older parents’ poor health status may increase caregiving burden, thereby increasing the risks of depression.
Several limitations of this study should be noted. This study did not examine all dimensions of intergenerational relationships, which are inherently complex and multifaceted. The young-old group may provide support to their children or even grandchildren and receive support from older parents and children as well. The effects of such relationships on the well-being of three or four generations should be examined in future studies. As a secondary data analysis, the study was limited by the variables available. Thus, it was not possible to examine all types of support (e.g., physical support) or older parents’ subjective appraisal of such support. A more comprehensive inquiry into support types and quality is recommended for future studies.
Conclusion
In aging China, the young-old group does not merely receive intergenerational support but also actively provides support to their older parents. Frequent visits and monetary support to older parents considered filial acts are in compliance with Chinese law. In turn, such actions may contribute to lower levels of depressive symptoms in older adult children.
Policymakers and health professionals should not underestimate the value of the support provided by older children to their parents, particularly when a national long-term care policy is not in place. In addition, more effort is needed to address the needs of this aging “sandwich generation” (the young-old group). Despite literature on the negative impact of family caregiving, this study suggests that this population may benefit from fulfilling a supportive role for their older parents. Still, this positive aspect of caregiving should be first acknowledged and then maintained through innovative interventions or programs that promote family support (frequent visits and monetary support) to older parents might hold promise. Future research might build upon this study by examining factors involved in complex intergenerational support systems among multigenerational Chinese families (i.e., grandchildren, adult children, the young-old, and the old-old).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.