
Abstract
Caregiving may prove either beneficial or harmful for caregiver well-being, depending on the circumstances surrounding care provision. Using data from the two most recent waves of the National Survey of Midlife Development in the United States (MIDUS, 2004–2014; N = 1,100), we examine whether providing care for an adult at both time points (i.e., 8–10 years apart) is associated with changes to self-esteem over the ten-year period, in comparison with providing care at only one time point, or not at all. We also examine moderation by caregivers’ age, parental status, and gender. Findings indicated (1) caregiving at both waves was associated with decreases in self-esteem among younger and midlife adults, but this effect weakened and even reversed with age; and (2) caregiving at both waves was associated with increased self-esteem among participants without children, but not among those with children. We discuss implications for identifying caregivers at greatest risk of diminished well-being.
In the U.S., family members are the most common providers of care for others who need assistance (Schulz & Eden, 2016). One in five adults (21.3%) provides care to an adult or child with health and/or functional care needs per year, equaling roughly 53 million Americans (AARP & National Alliance for Caregiving, 2020). Rates of care for family members rise sharply in early adulthood and peak in one's 30s, when adults are often providing care for children or working simultaneously (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019). The average length of time as a caregiver for an adult is 4.5 years, though an increasing proportion of U.S. caregivers provide care for 5 years or longer (AARP & National Alliance for Caregiving, 2020). This suggests that both repeated and longer-term commitments to care provision may be increasingly common across adulthood.
Providing care can have both positive and negative consequences for mental and physical health (Pinquart & Sörensen, 2003). Further, providing care for longer periods of time is typically associated with reporting more emotional stress (AARP & National Alliance for Caregiving, 2020). Most prior research in this area has examined the implications of caregiving for negative aspects of well-being (e.g., depression), yet little work has examined the potential consequences for positive aspects of well-being such as self-esteem (Pinquart & Sörensen, 2003). Although caregiving can be burdensome and stress-inducing, it also has the potential to benefit some caregivers’ self-esteem by inciting the caregiver to feel good about him/herself or appreciate life more (Lin et al., 2012). Self-esteem reflects individuals’ sense of value to others and their feelings of worthiness (Thoits, 1989, 2011). It is also associated with other measures of well-being (Cohen et al., 2002; Stokes, 2019; Thoits, 2011) as well as biological health (Stokes, 2020). The limited research available suggests the association between providing care and self-esteem is negative but often dependent on other demographic characteristics (Aggar et al., 2011; Kim, 2017).
We extend the caregiving literature by considering self-esteem as an important outcome, especially during mid-life when caregiving is a common part of the life course. We extend the caregiving and self-esteem literature by considering three important demographic characteristics (age, parental status, and gender) as potential moderators. We also take into consideration the role of time, as the benefits and/or harms of caregiving may accumulate gradually over time, or may not reveal themselves until after a critical threshold has been reached. We use data from the two most recent waves of the National Survey of Midlife Development in the United States (MIDUS, 2004–2014) to examine the unique associations between caregiving statuses and self-esteem over a 10-year period.
Background
The size of the caregiver population continues to grow over time, especially as the population ages (AARP & National Alliance for Caregiving, 2020). Caregiving occurs throughout the life course and is most common during early and middle adulthood (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019). Providing care during midlife has the potential to affect other life course outcomes as well, due to competing responsibilities present during this life stage, including parenting and balancing one's own aging processes (Pavalko, 2011).
Caregiving and Self-Esteem
Current caregiving scholarship focuses heavily on the costs and negative implications of caregiving for care providers (Lin et al., 2012; Pinquart & Sörensen, 2003). Caregivers often suffer costs to their overall mental health through feelings of burden (Pinquart & Sörensen, 2003) or depression (Bom et al., 2019; Lin et al., 2012). Yet caregiving may also offer a sense of meaning and purpose for the caregiver (Cohen et al., 2002; Noonan & Tennstedt, 1997), thereby improving caregivers’ feelings about themselves and their life (Lin et al., 2012). Mixed results regarding the influence of providing care on well-being raise the question of whether the impact of caregiving may vary based on the duration of care provision and repeated periods of providing care, because the burdens of caregiving may be cumulative and chronic rather than acute.
We focus on self-esteem because it serves as an emotional coping mechanism that is protective of mental and physical health throughout adulthood (Thoits, 2011). Indeed, although self-esteem is generally stable in adulthood (e.g., Wagner et al., 2015), it is susceptible to social relationships and experiences (e.g., Stokes, 2019; Thoits, 2011). Moreover, self-esteem is also linked with downstream harm to mental, physical, and biological health outcomes (Kim & Thomas, 2019; Stokes, 2019; 2020; Thoits, 2011). Insofar as caregiving burdens undermine self-esteem over time (Aggar et al., 2011), they may likewise prove harmful to other aspects of both mental and physical health (Stokes, 2020; Thoits, 2011), global appraisals of the quality of life (Kim et al., 2007), or a loss of sense of self (Skaff & Pearlin, 1992). However, care may also bolster self-esteem, as providing care for others may provide the caregiver with a sense of purpose and feeling valued (Noonan & Tennstedt, 1997).
Current caregiving research generally finds a negative association with self-esteem, but samples tend to be small, localized, or focus on providing care for people with specific ailments (e.g., cancer) or on one specific category of caregivers (e.g., spouse). For instance, among a sample of 108 care providers for an adult with a disability who visited a rehabilitation center, care stress was associated with negative implications for the caregiver's self-esteem (Kim, 2017). In another study of 448 caregivers for a person with cancer, caregiving was positively associated with self-esteem for men but negatively associated with self-esteem for women (Kim et al., 2007). Among a sample of caregivers for an older adult with dementia, spouses were more likely to experience a negative effect on self-esteem than adult children (Chappell et al., 2015). Taken together, these studies suggest that the overall implications of caregiving on self-esteem within a broader population of adults may be negative, but results are not conclusive, and effects also appear to differ by contextual factors.
Caregiving, the Life Course, and Cumulative Effects
Caregiving is pervasive across the life course, and entering into—and out of—multiple caregiving roles may serve as pivotal life transitions for the caregiver (Elder et al., 2015). At age 15, people can be expected to participate in an unpaid caregiving role (including caring for small children, someone who is ill, disabled, or elderly) for over half of their remaining life (Ophir & Polos, 2021). One in six (17.2%) adults aged 45 and older who do not currently provide care or assistance to a friend or family member with a health problem or disability expect to do so in the next two years (CDC, 2018). Although short bouts of providing care are more common than long-term care provision, roughly three in 10 current caregivers have provided care for an adult for five years or more, with adults ages 50–64 comprising the largest percentage of these caregivers (AARP & National Alliance for Caregiving, 2020).
Additionally, duration of caregiving and transitions into and out of providing care may impact caregivers in distinct ways (Kaufman et al., 2019). For instance, entering into and out of caregiving roles may lead to immediate and acute changes in well-being (Uccheddu et al., 2019). Generally, the psychosocial outcomes of transitioning into a care role are negative (e.g., Zwar et al., 2020). Conversely, the burdens of caregiving may build slowly over time, manifesting only after extended periods of care provision. Indeed, caregivers who provide for longer periods of time generally have worse outcomes than caregivers who provide for shorter periods of time (AARP & National Alliance for Caregiving, 2020). Studies that investigate long-term caregiving and self-esteem are limited, however. One small study of partners caring for someone with cancer finds that the magnitude of self-esteem decline is small over a six-month post-discharge period (Nijboer et al., 2000). The present study examines caregiving status and self-esteem over an 8–10-year period, to further examine the shorter and longer-term implications of caregiving for adults’ well-being.
Moderating Roles of Age, Parental Status, and Gender
The extent to which caregiving presents a burden to family members is likely dependent upon other contextual factors, as well (Pearlin et al., 1990). For example, caregiving may prove harmful among adults in the early and middle stages of midlife, as these caregivers are likely to be balancing their important aging processes (e.g., saving for retirement and maintaining their own health) as well as other competing care roles, such as parenting. Yet these same contextual factors may instead serve as a resource, leading to fewer negative consequences for the caregiver (Pearlin et al., 1990).
Age may be an especially important moderator in the association between caregiving and self-esteem, as care is common across early and middle age. However, current findings in this area are mixed. Midlife as a whole is a pivotal stage in the life course, not only filled with periods of stability and continuation of some roles but also the potential for changes and transitions as a person ages (Elder et al., 2015; Lachman, 2015). Becoming a caregiver can, therefore, have an especially negative impact on younger caregivers who are balancing more competing roles and responsibilities, while also establishing their own independence and life (Seltzer & Li, 2000). Yet in a small study of partners caring for cancer patients, negative changes in self-esteem over time were greatest among older adults (65+) compared to younger (under 65) caregivers (Nijboer et al., 2000). However, emotional strain from caregiving may be similar among caregivers of all ages (Koumoutzis et al., 2020). Likewise, self-esteem is generally stable throughout the years of midlife and early old age but is susceptible to the influences of social ties and stressors as well, and particularly so in midlife and oldest-old age (Stokes, 2019; Thoits, 2011). Thus, the intersection of caregiving responsibilities—and, crucially, providing care at multiple points in the life course—with age may be critical for understanding variation(s) in the implications of caregiving for well-being across the life course.
Caregiving during midlife also presents challenges because many adults also become parents and take on childcare responsibilities during this period. Findings regarding balancing childcare alongside caring for an adult are also mixed. In a study of working caregivers, “sandwiched” employees report more stress than those caring for only one generation (Halinski et al., 2018). In a study of 327 cancer outpatients and their adult daughter caregivers, having care responsibilities for children or grandchildren alongside their other care duties was associated with increased ratings of self-esteem (Bachner et al., 2009). However, other work finds no difference in well-being among those balancing different forms of care (Daatland et al., 2010). Overall, the literature in this area is notably thin (Rubin & White-Means, 2009). In other words, not all life course transitions that may moderate the effects of caregiving on well-being are well-aligned with chronological age. Competing responsibilities, such as care for a child, can emerge at different points in the life course for different individuals, if they arise at all. By examining both age and parental status as potential moderators, we aim to disentangle the unique contributions of the life course (e.g., age) and competing responsibilities (e.g., parental status) to the caregiving–well-being link.
Lastly, caregiving is a highly gendered experience, with women far more likely to be caregivers for family members than men across the life course, except at the oldest ages (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019). Although both men and women can expect to spend over half of their life providing care in some form, women are more likely to provide intensive, high-level care for a family member compared to men (Ophir & Polos, 2021). Yet men's care roles are changing within each successive cohort and men increase their participation in care provision as they age (Lopez-Anuarbe & Kohli, 2019). Overall, findings on the effects of care provision on well-being for men and women are mixed (Pinquart & Sorensen, 2006), and research on well-being for men who provide care is quite limited (Lopez-Anuarbe & Kohli, 2019). Further, beyond gender differences in the likelihood and intensity of caregiving, men and women may also differ regarding which caregiving roles they enter into and which duties they are tasked with (Patterson & Margolis, 2019).
Current Study
We extend previous research on caregiving by connecting separate literature on the implications of caregiving for well-being and on social influences on self-esteem. We also examine caregiver characteristics that may moderate the effects of caregiving on self-esteem. Specifically, our study has the following aims:
First, we aim to examine whether caregiving status at either or both time points is associated with changes in self-esteem over an 8–10-year span, using a nationally representative sample of mid-life adults in the U.S. (Aim 1). Further, we aim to determine whether any caregiving status differences concerning self-esteem vary according to age (Aim 2), parental status (Aim 3), or gender (Aim 4). Taken together, exploration of these four aims will contribute to our understanding of the circumstances under which caregiving may be particularly influential—for better or for worse—for care providers’ self-esteem.
Methods
Data and Sample
Data for this study were drawn from the two most recent waves of the National Survey of Midlife Development in the United States (MIDUS, 2004–2014). MIDUS began in 1995–1996 with Random Digit Dialing (RDD) to gather a national probability sample of over 7,000 non-institutionalized, English-speaking Americans, ages 25–74 (Ryff et al., 2017). Telephone interviews were conducted, with additional questions included in a Self-Administered Questionnaire (SAQ). Follow-up surveys were administered in 2004–2005 (wave 2) and 2013–2014 (wave 3). Questions concerning both caregiving (telephone interview) and self-esteem (SAQ) were added to MIDUS at wave 2 and repeated at wave 3; therefore, the analytic sample was comprised of MIDUS participants who completed the telephone interview and the SAQ at both wave 2 and wave 3. A total of 1,805 participants completed the telephone interview and SAQ at wave 2, of whom 1,100 (60.94%) completed the telephone interview and SAQ again nearly a decade later at wave 3. These 1,100 participants formed our analytic sample. Additional information concerning attrition is included in Supplemental Table 1.
Measures
Outcome
Self-esteem was measured using a seven-item mean-score scale (Rosenberg, 1965). Sample items included “I take a positive attitude toward myself” and “At times I feel that I am no good at all.” Response options ranged from 1 (strongly agree) to 7 (strongly disagree), with higher values indicating greater self-esteem (α = .76). The Cronbach's alpha exhibits acceptable, although not excellent, internal consistency. However, the Rosenberg (1965) self-esteem scale remains a gold-standard measure and is the most commonly used measure of self-esteem, which allows our findings to be compared with extant research concerning self-esteem in adulthood (see Orth, Robins, & Widaman, 2012; Stokes, 2019). Self-esteem was set to missing at each wave if participants answered fewer than half of the scale items. For analysis, self-esteem was measured as a change score.
Predictors
Caregiving status. Participants were asked at each wave whether they had “personally cared for a period of one month or more to a family member or friend because of a physical or mental condition, illness, or disability.” Caregiving status was coded using four dichotomous indicators: Provided no care at T1 or T2 (reference), provided care at T1 only, provided care at T2 only, and consistently provided care at T1 and T2.
Age. Age was measured as a continuous variable, in years, and was mean-centered for analysis.
Parental status. MIDUS asked participants to list how many living children they have, including “biological, adopted, step and foster children living with you or elsewhere” and to include any living children the participant has fathered or given birth to (Ryff et al., 2017). Parental status was measured using dichotomous indicators for Has living children and Does not have living children (reference).
Gender. Gender was self-reported and measured using dichotomous indicators for Female and Male (reference).
Covariates
To protect against potential confounding, control measures were included for marital status, social integration, neuroticism, education, employment status, income, self-rated health, race, and Hispanic ethnicity. Marital status was measured using dichotomous indicators for married (reference), divorced/separated, widowed, and never married. Social integration was measured using a three-item mean-score scale (Keyes, 1998). Neuroticism was measured using a four-item mean-score scale (Lachman & Weaver, 1997). Educational attainment was measured using dichotomous indicators for less than a high school degree (reference), high school degree, some college, college degree, and some education beyond college. Employment status was measured using dichotomous indicators for employed (reference), not employed, and retired. Income was measured on a 42-point scale ranging from 1 (less than $0) to 42 ($200,000 or more) and was standardized for analysis. Self-rated health was measured as a continuous variable ranging from 1 (poor) to 5 (excellent). Race was measured using dichotomous indicators for White (reference), Black, and Other Race. Lastly, a dichotomous indicator Hispanic ethnicity was included (reference = Not Hispanic).
Analytic Strategy
We used change-score (CS) modeling to address our research questions (Allison, 1990; Johnson, 2005). Thus, the outcome was measured as a change in self-esteem from wave 2 to wave 3, while covariates were measured at baseline (wave 2). CS modeling implicitly accounts for all stable between-person variation in the outcome and can also produce more intuitive and less biased results than lagged dependent variable (LDV) modeling (Allison, 1990; Johnson, 2005). In the present case, LDV modeling produced the same significant findings of interest as the CS approach presented below.
The majority of participants (85.64%) provided complete data on all measures included in the analysis. Missing data diagnostics did not indicate any clear patterns of missingness. Therefore, in order to protect against potential bias from listwise deletion, we used multiple imputations by chained equations to address missing data (Royston, 2005), with a total of 10 data sets estimated. Significant results of interest were unchanged in models using listwise deletion.
Our analysis included the following steps: Model 1 included the main effects of all focal predictors and covariates. Model 2 added an interaction between age and caregiving status to Model 1. Model 3 added an interaction between parental status and caregiving status to Model 1. Model 4 added an interaction between gender and caregiving status to Model 1. Lastly, Model 5 included the main effects of all focal predictors and covariates, along with all significant interactions identified in Models 2 through 4.
Results
Descriptive statistics for all measures are reported in Table 1. Overall, self-esteem was fairly high at both time points (M = 5.45 at wave 2 and M = 5.37 at wave 3, on the 1–7 scale). However, self-esteem did decline significantly over the 9-year period (M = −0.08, p < .01). This relatively modest level of change on average also masks greater variability in self-esteem in this sample. For instance, nearly 1 in 4 (22.8%) participants exhibited an increase or decrease of at least one-point on the seven-point scale between time points. Additionally, while the majority of participants reported no caregiving at either time point (76.91%), there was considerable variation among caregivers, with 10.36% providing care at both wave 2 and wave 3, 3.64% providing care only at wave 2, and 9.09% providing care only at wave 3. Moreover, the majority of participants were female (54.27%), married (69.13%), and had children (87.00%). Notably, female participants were significantly overrepresented (p < .001) in all three caregiving groups, including providing care at baseline only (72.31%), providing care at follow-up only (60.43%), and consistently providing care at both baseline and follow-up (62.14%). Lastly, the mean age at baseline was 55.84 years, indicating that the average participant experienced the years of late midlife and early older age during the course of this study.
Descriptive Statistics, National Survey of Midlife Development in the United States, 2004–2014 (N = 1,100).
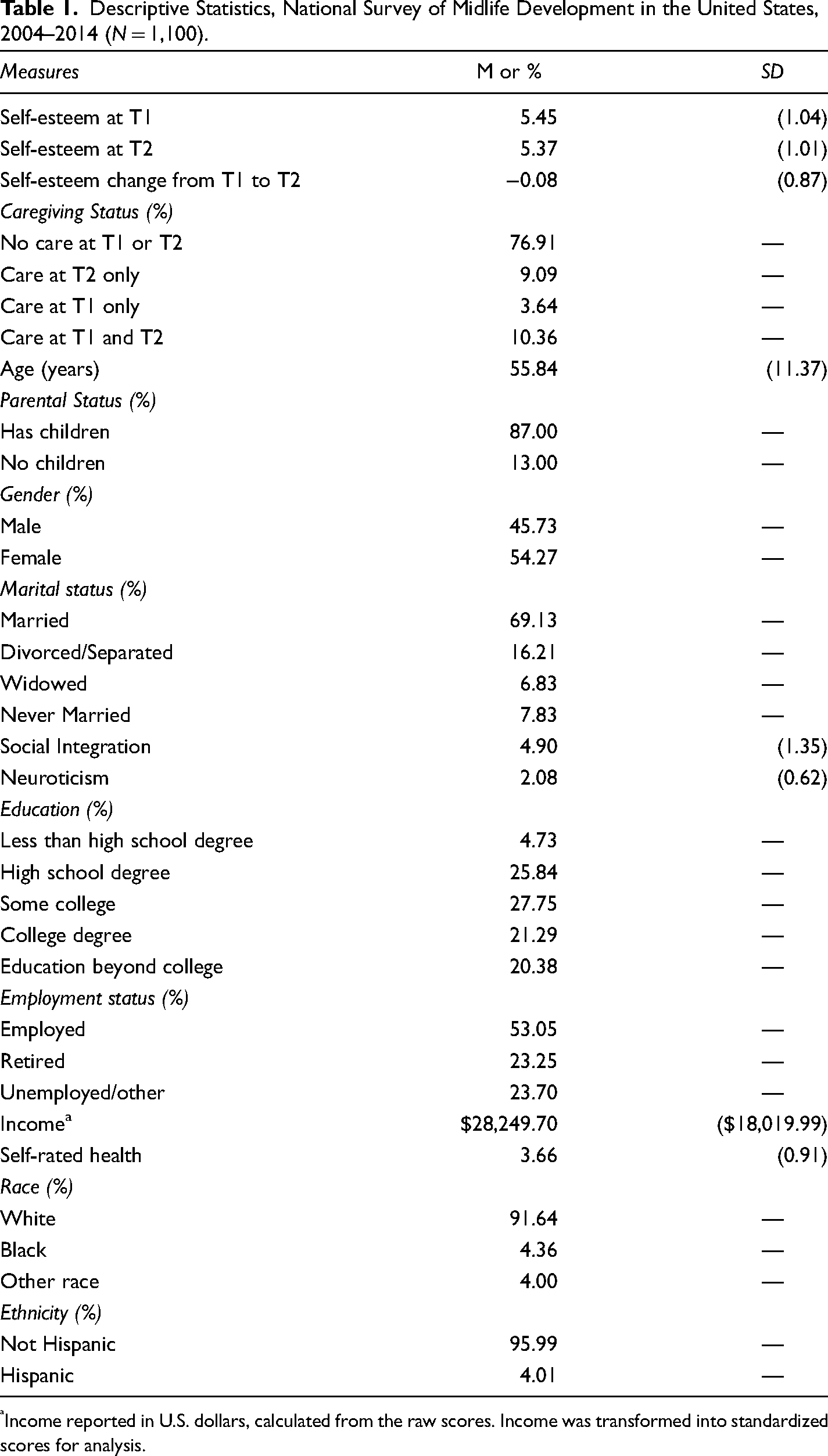
Income reported in U.S. dollars, calculated from the raw scores. Income was transformed into standardized scores for analysis.
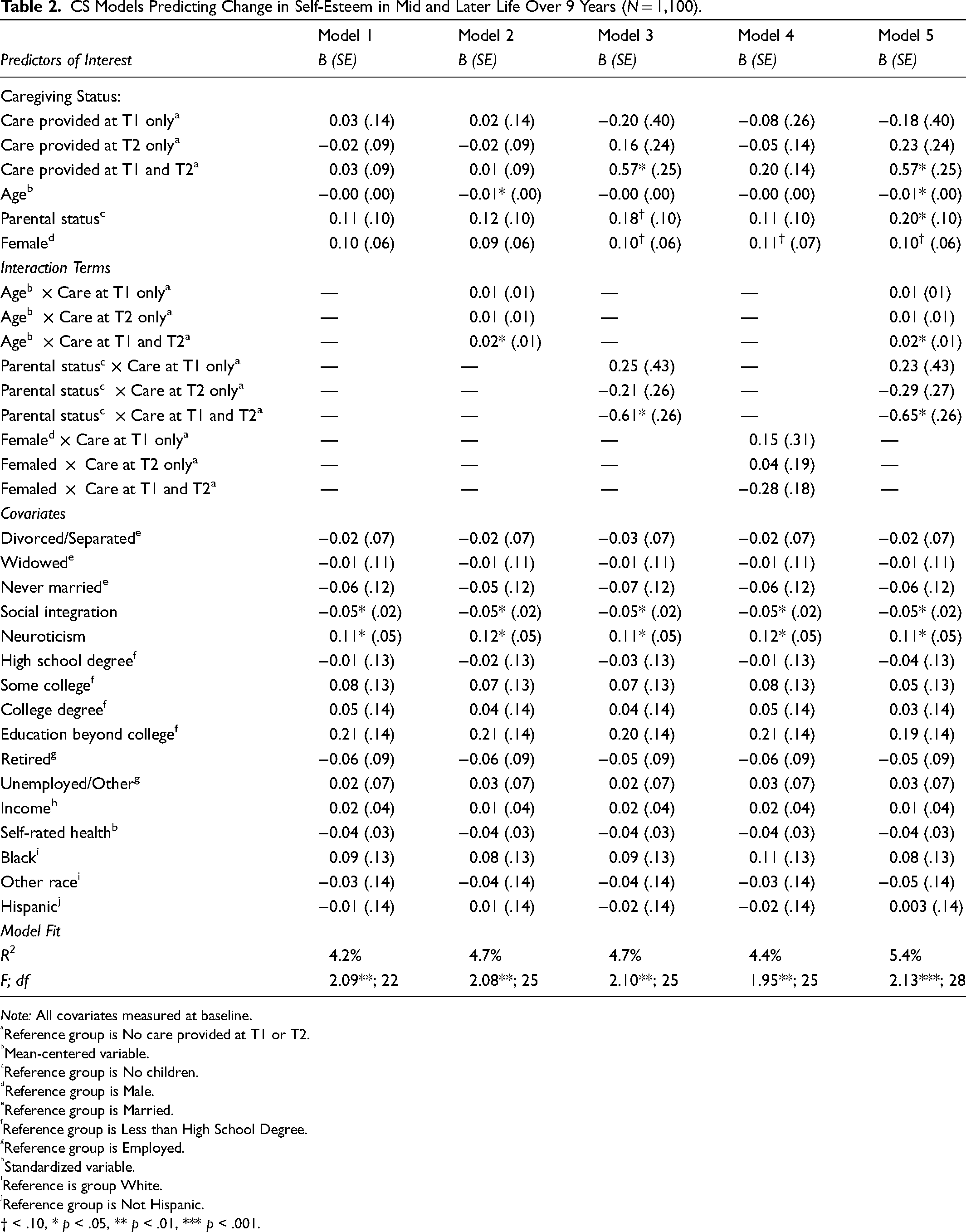
The results of our analytic CS models are presented in Table 2. In the main effects of Model 1, there were no significant differences in self-esteem change among the caregiving status groups. Moreover, neither age (B = −0.00, p = .20), parental status (B = 0.11, p = .24), nor female gender (B = 0.10, p = .10) was significantly linked with change in self-esteem. Among covariates, only baseline social integration (B = −0.05, p < .05) and neuroticism (B = 0.11, p < .05) were associated with significant changes to self-esteem.
CS Models Predicting Change in Self-Esteem in Mid and Later Life Over 9 Years (N = 1,100).
Note: All covariates measured at baseline.
Reference group is No care provided at T1 or T2.
Mean-centered variable.
Reference group is No children.
Reference group is Male.
Reference group is Married.
Reference group is Less than High School Degree.
Reference group is Employed.
Standardized variable.
Reference is group White.
Reference group is Not Hispanic.
† < .10, * p < .05, ** p < .01, *** p < .001.
Model 2 added interaction terms between the caregiving status groups and individuals’ age to Model 1. The main effects of caregiving status remained nonsignificant, indicating no overall group differences in self-esteem change at average age (55.84 years at baseline). However, the main effect of age became negative and significant (B = −0.01, p < .05) indicating greater declines in self-esteem at older ages among those who provided no care at baseline or follow-up (the reference group). Further, the moderation analysis revealed a significant interaction between age and the consistent caregiving group (B = 0.02, p < .05). This interaction indicates that providing care at both baseline and follow-up is more harmful for self-esteem at younger ages and less harmful at older ages. Supplemental analyses (not shown) centering on age at 30 years and 80 years produced main effects for the consistent caregiving group that was negative and significant (B = −0.46, p < .05) and positive and significant (B = 0.35, p < .05), respectively. This demonstrates that consistent caregiving was associated with greater declines in self-esteem compared with no caregiving at younger ages, yet with smaller declines or even increases in self-esteem compared with no caregiving at older ages. No other coefficient significance levels were altered from Model 1.
Model 3 added interaction terms between the caregiving status groups and parental status to Model 1. The main effects of providing care at one point in time (whether at baseline or follow-up) but not at another remained non-significant, while the main effect of consistent caregiving (i.e., providing care at both time points) was positive and significant (B = 0.56, p < .05). This indicates that, among those with no children, participants who provided consistent care experienced greater increases—or smaller decreases—in self-esteem than those who provided no care at either wave. Further, the moderation analysis revealed a significant negative interaction between parental status and the consistent caregiving group (B = −0.61, p < .05), indicating that the comparative benefit of providing consistent caregiving for self-esteem was contingent upon childless status. No other coefficient significance levels were altered from Model 1.
Model 4 added interaction terms between the caregiving status groups and gender to Model 1. None of the interaction terms was significant, and no coefficients differed in significance compared with Model 1. Model 5 simultaneously added to Model 1 the significant interaction terms identified separately in Models 2 and 3. The inclusion of the nonsignificant interaction terms identified in Model 4 did not alter the findings of interest, and these were excluded for parsimony. The main effects of providing care at only one time point (whether at baseline or follow-up) remained nonsignificant, while the main effect of consistently providing care at both time points was positive and significant (B = 0.57, p < .05). Because of the multiple interaction terms, this coefficient refers to consistent caregivers without children at age 55, compared with their 55-year-old childless counterparts who provided no care at either time point. The main effect of age was negative and significant (B = −0.01, p < .05), indicating an increasing decline in self-esteem with age among consistent noncaregivers. Again, a significant interaction between age and consistent caregiving status (B = 0.02, p < .05) revealed that this age-based decline did not apply to the consistent caregiving group but rather implies that caregiving burdens are most harmful to self-esteem among younger caregivers. Further, the main effect of parental status was rendered positive and significant (B = 0.20, p < .05) and can be interpreted as the comparative benefit to self-esteem of having children among those who consistently provided no care. The significant negative interaction between parental status and the consistent caregiving status remained (B = −0.65, p < .05) and highlights the particular burden of long-term caregiving for those with children. No other coefficient significance levels were altered from Model 1.
R2 for the models presented was fairly modest (5.4% in Model 5). However, this is in part due to the use of a change-score outcome, which limits variance only to within-person change in the outcome between time points, rather than a combination of within-person change and between-person differences. For example, R2 for the same Model 5 using LDV rather than CS modeling was 46.4%. Moreover, the majority of covariates included in the CS models were not statistically significant; a model including only the predictors of interest and the interaction terms explains 3.0% of the variance in the change-score outcome, indicating that the majority of variance explained in the models presented was due to the caregiving status measures and the contextual moderators themselves. Given the relative stability of self-esteem during adulthood (e.g., Wagner et al., 2015), the models presented here display meaningful—if still modest—explanatory results.
Discussion
In the U.S., family members are frontline caregivers for others who need assistance (AARP & National Alliance for Caregiving, 2020; Schulz & Eden, 2016), and caregiving is a common experience across the life course (Ophir & Polos, 2021). Considering that the likelihood of providing care for another person peaks in early mid-adulthood and remains relatively high during midlife (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019), it is important to understand the impact of caregiving during this life course stage as it can have implications for one's own aging process and well-being. We extend the previous literature in three distinct ways: 1) by inquiring how providing care in midlife is associated with self-esteem, an important psychosocial outcome; 2) by addressing the distinction between providing care at multiple time points across nearly a decade, versus care provision at one or another discrete point in time; and 3) by examining the moderating effects of age, parental status, and gender.
Overall Results
A majority (76.91%) of adults in our sample did not provide personal care for a period of one month or more to a family member or friend because of a physical or mental condition, illness, or disability. Among those who did provide care, one out of 10 (10.36%) provided care at both waves and the remaining respondents transitioned into or out of care roles, providing care at one wave but not the other. Self-esteem remained fairly high across our 10-year study period, though there was a significant decline as respondents aged. We did not find an overall effect of caregiving—whether at one time point or at both—on change in self-esteem. This lack of findings may be due to the broad nature of the caregiving measurement, or the extended gap between survey waves. However, it may also be due to the diverse nature of caregiving experiences, and the potential for circumstances such as age, parenting, and gender to determine whether and when caregiving matters for self-esteem.
Moderation by Age
In models interacting age with caregiving status, we find that providing care across both waves was significantly—and positively—associated with self-esteem among participants in their mid-50s. Moreover, the significant interaction reveals that the benefits of long-term caregiving accrue with age and are lowest—or even negative—at younger ages. This finding further emphasizes the importance of midlife as a pivotal period in the life course (Elder et al., 2015; Lachman, 2015), and the influence of caregiving on well-being. Engaging in consistent caregiving across the 10-year study period appears more detrimental to self-esteem at younger ages, but this association lessens as respondents’ age. The finding for early midlife adults aligns with other work that shows detrimental effects of providing care at younger ages (Seltzer & Li, 2000) but is in contrast to work that suggests that older adults experience more negative consequences to their self-esteem (Nijboer et al., 2000) or that emotional strain may be similar among caregivers of all ages (Koumoutzis et al., 2020). Differences in findings across studies are likely due to samples used, as well as the measurement of care. A lack of significant moderation concerning those who provided care at one but not both waves may suggest that transitioning into and out of care roles is more common and even normative at these ages, or that the care needs and requirements in those cases were more immediate and less long-lasting.
Moderation by Parental Status
Respondents’ parental status also revealed itself to be an important factor. Among respondents with no children, providing consistent care was associated with greater increases in self-esteem compared to respondents who did not provide any care. Because caregiving is a common occurrence across the life course (Ophir & Polos, 2021) and especially so during early and middle adulthood (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019), providing care in midlife may provide a sense of purpose. Indeed, among those without children, care provision may instill a sense of being needed and valued; among those with children, it may represent an additional and unwanted burden.
Interestingly, age and parental status findings remain significant when accounting for both, indicating that although age and parental status are related, they have distinct moderating effects on self-esteem. Both life course (i.e., age) and competing responsibilities (i.e., parental status) affect the role and influence of care provision on adults’ well-being. Combining care roles, for children and for an adult, compound effects and have the potential to accumulate negative effects on self-esteem.
Moderation by Gender
Informal caregiving in the U.S. is predominantly performed by women, and this held true in the present sample (Dukhovnov & Zagheni, 2015; Patterson & Margolis, 2019). Indeed, women were more likely than men to be in each of the three caregiving status groups. This speaks to the continuation of gendered norms and expectations surrounding caregiving, even as more recent cohorts have exhibited somewhat greater gender equity in this domain (Lopez–Anuarbe & Kohli, 2019; Ophir & Polos, 2021). However, associations of caregiving with self-esteem did not vary by gender.
Importantly, even in the absence of significant moderation by gender, the implications of our findings for care providers remain highly gendered. First, because women are more likely to be caregivers—including at both time points—than men, they also face greater exposure to the potentially harmful stresses of consistent caregiving, whether due to long-term care provision to a single recipient or due to repeated engagement in caregiving roles over time. Moreover, although female caregivers did not differ from their male counterparts concerning age, there were notable gender differences in parental status: Among all three caregiving statuses together (χ2 = 11.08 p < .01) and among the consistent caregiving group specifically (χ2 = 5.56, p < .05), women caregivers were significantly more likely to have living children than men caregivers were (92% vs. 77% among all caregivers; 93% vs. 78% among consistent caregivers). This indicates that female caregivers, and particularly those who reported providing care at both time points, are at heightened risk of the “double burden” presented by the competing roles of parent and caregiver.
Effect Sizes and Practical Implications
The R2 and coefficient values presented here suggest only moderate effects, yet the context of the analysis is crucial for assessing their practical importance. First, because the outcome is a change-score, coefficients refer only to within-person changes in self-esteem, rather than to between-person differences in self-esteem (as with cross-sectional analysis) or to a combination of the two (as with random effects models). That our predictors of interest exhibit significant effects at all suggests the potential for causal influences. Moreover, given that self-esteem is often relatively stable in adulthood (Wagner et al., 2015) and that diminished self-esteem can lead to a series of other downstream harms to mental and physical health (Stokes, 2020; Thoits, 2011), these significant associations between caregiving status and change to self-esteem—including the contextual factors that shape these influences—represent important information for practitioners and policymakers interested in reducing caregiver burden and its consequences. Lastly, although some of the significant coefficients themselves are only of moderate size (e.g., B = 0.57 for consistent caregiving among those with no children (Model 3), B = 0.02 for the interaction between consistent caregiving status and age (Model 2)), in context they appear quite meaningful. For instance, in a recent longitudinal study of self-esteem that used the same data set and employed random effects modeling, the significant coefficients for Black race (vs. White; B = 0.27, p < .001), Hispanic ethnicity (vs. not Hispanic; B = 0.20, p < .05) and College degree (vs. Less than high school; B = 0.16, p < .01) were notably smaller than that for consistent caregiving among nonparents in this study, even though random effects model coefficients incorporate both within-person change and between-person difference components. Further, the seemingly small coefficient for the interaction between consistent caregiving status and age takes on added significance when considering the 50-year age range of the MIDUS sample. The nonsignificant main effect for consistent caregiving status at age 55 (B = 0.01, Model 2) becomes 0.21 at age 65, 0.41 at age 75, and so on. These again demonstrate effect sizes comparable to or greater than race/ethnicity and education differences in self-esteem over time (e.g., Stokes, 2019), despite referring to within-person change between waves alone and not to average between-person differences in self-esteem. In sum, despite the apparently moderate effect sizes presented in this study, the context provided by previous literature on self-esteem in adulthood makes clear the practical importance of the effects of this size.
Limitations and Future Research
This study has a number of limitations worth noting. First, the measure of caregiving is very broad; however, caring can encompass a variety of experiences (AARP & National Alliance for Caregiving, 2020; Schulz & Eden, 2016). Further, MIDUS data do not provide the number of care recipients respondents have or the precise relationships with those care recipients. Future research should incorporate more fine-grained measures, as the effects of caregiving may vary according to such circumstances (Pinquart & Sörensen, 2003). For instance, more detailed information concerning specific caregiving duties, whether one serves as a primary or secondary caregiver for the care recipient, and a direct assessment of multiple caregiving roles would provide useful information for future studies. Moreover, qualitative research would be well-suited to better understanding caregivers’ experiences and perceptions of their caregiving role(s), including the extent to which these shape feelings of self-worth and being valued by others. Second, the sample is limited to two waves across a 10-year period, which may restrict our ability to understand more complex trajectories of both caregiving and self-esteem. Future research should analyze data collected over shorter intervals, to better reveal patterns and consequences of short-term and long-term care provision. Third, and relatedly, our operationalization of “consistent care provision” is based on respondents providing care at both time points, but we are unable to determine whether care was consistently provided during the intervening years, or whether the care recipient is the same at both time points. Although both of these alternatives imply a greater and longer-term engagement in caregiving than providing care at only one time point (or not at all), the inability to distinguish between them in the present data limits interpretation. Future research should examine whether the “cumulative burdens” of caregiving suggested by our findings accrue over time during long-term caregiving relationships, or emerge as a result of multiple different caregiving experiences. Lastly, although drawn from a nationally representative sample at baseline, the majority of our sample is White, non-Hispanic. As the aging population in the U.S. becomes more diverse, future research should aim to analyze racial and ethnic differences in these trends.
Conclusion
Despite these limitations, the present study makes a number of contributions to the literature on caregiving and well-being throughout mid- and later life. This study provides insights into the association between caregiving and self-esteem using nationally representative data from the U.S. We contribute a nuanced understanding of how the relationship between providing care and self-esteem may vary by important caregiver characteristics, particularly age and parental status. Our results have implications for understanding how caregiving may have distinct impacts on caregivers under different circumstances. In particular, caregivers balancing multiple care provision roles (e.g., with children), and those providing extensive care at younger ages appear at the highest risk of poor well-being; conversely, older adults providing consistent care and caregivers without children of their own may derive benefits to well-being from their engagement in care provision. Policies and programs that effectively identify caregiver populations most at-risk for deleterious outcomes could aid in reducing caregiver burden and improving mental and physical health among the caregiver population.
Supplemental Material
sj-docx-1-ahd-10.1177_00914150221128976 - Supplemental material for Caregiving and Self-Esteem in Mid and Later Life: Is There Variation by Age, Parental Status, and Gender?
Supplemental material, sj-docx-1-ahd-10.1177_00914150221128976 for Caregiving and Self-Esteem in Mid and Later Life: Is There Variation by Age, Parental Status, and Gender? by Jeffrey E. Stokes and Sarah E. Patterson in The International Journal of Aging and Human Development
Footnotes
Acknowledgments
Thank you to Alison C. Rataj and Lilian Tran for their assistance. This work was supported by the National Institute on Aging of the NIH (T32AG000221). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH or their employer. Publicly available data from the MIDUS study was used for this research. Since 1995 the MIDUS study has been funded by the John D. and Catherine T. MacArthur Foundation Research Network and the National Institute on Aging (P01-AG020166; U19-AG051426). An early version of this paper was presented at the 2021 Population Association of America conference.
Author Contributions
J.E.S. and S.E.P. planned the study; J.E.S. performed all statistical analyses; and J.E.S. and S.E.P. wrote the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.