
Abstract
Stress associated with the COVID-19 pandemic and the measures implemented to prevent its spread dramatically shifted our social networks, interactions, and contexts, all of which influence the assessment of one's subjective well-being (SWB). Drawing on data collected from 1,318 adults between April and May 2020, we used structural equation modeling to analyze the relationship between pandemic-related stress and SWB (life satisfaction, positive affect, negative affect), and examined how these relationships vary across age. Pandemic-related stress was associated with lower life satisfaction and higher negative affect. However, no evidence of age moderation emerged. Subsequent analysis examined different aspects of social resources as potential mediating variables. Loneliness fully mediated the relationship between stress and life satisfaction, while social support demonstrated evidence of partial mediation. Further, loneliness and social support partially mediated the relationship between stress and negative affect. Findings suggest that pandemic-related stress impacts SWB, and social resources help explain these impacts.
As Coronavirus Disease 2019 (COVID-19) spread globally, high priority was placed on the virus’ prevention and containment while the potential psychosocial implications of the pandemic were overlooked (Ornell et al., 2020). Research on prior epidemics, however, has shown that impacts on mental health may have a more substantial, longer-lasting effect on individuals than the virus itself (Ornell et al., 2020; Reardon, 2015; Shigemura et al., 2020). Research on the COVID-19 pandemic has also documented social and behavioral impacts such as lower trust in individuals and social institutions (Kar et al., 2023), including those providing information about COVID-19 (Khankeh et al., 2022), as well as individual differences in engagement with health protective behaviors associated with stress and fear of COVID-19 illness (Kukreti et al., 2024; Liu & Arledge, 2022). In sum, the “collective trauma” experienced during the pandemic (Garfin et al., 2020, p. 355) may adversely and differentially impact psychological well-being, warranting further investigation into this relationship. Thus, the purpose of the current study is to explore the associations between pandemic-related stress and subjective well-being (SWB) using data collected during the first peak of the pandemic in the U.S. and to examine age as a moderator of these associations. We then test the mediating influence of three social resources, specifically loneliness, social isolation, and social support, in the relationship between pandemic-related stress and SWB.
COVID-19 Pandemic-Related Stress and SWB
Among the many conceptualizations used to describe SWB, the three-factor model – comprising both cognitive-judgmental (i.e., life satisfaction) and affective/mood processes (i.e., positive and negative affect) – is among the most common (Busseri & Sadava, 2011). Importantly, high SWB is associated with a myriad of positive outcomes including better physical and mental health across the lifespan (Diener et al., 2018). The onset of the COVID-19 pandemic may have had detrimental effects on SWB because individuals experienced sudden fear and uncertainty coupled with radical changes in how they lived, worked, and socialized. Over 90% of U.S. residents were under stay-at-home orders in April 2020, which greatly heightened risk for negative psychological outcomes such as anxiety, depression, post-traumatic stress disorder, and disrupted SWB (Brooks et al., 2020; Mervosh et al., 2020). Blasco-Belled et al. (2020) hypothesized that exposure to daily negative emotions, in addition to feelings of uncertainty, fear, and loss of social interactions experienced because of the pandemic would impact one's subjective evaluation of life satisfaction. Researchers across several countries, including the United Kingdom, Switzerland, France, and Singapore, reported declines in life satisfaction during the pandemic, even after initial lockdown measures were eased (Brülhart & Lalive, 2020; Foa et al., 2020; Recchi et al., 2020). Estimates from China also demonstrated that the onset of the pandemic led to a 74% reduction in well-being, as measured by positive and negative affect (Yang & Ma, 2020), providing evidence supporting the negative impact of the COVID-19 pandemic on SWB. And, in their study of German adults between March and May 2020, Zacher and Rudolph (2021) found higher stress appraisals to be associated with lower life satisfaction and positive affect, and greater negative affect.
However, findings regarding the impacts of macro-level stressors, including the COVID-19 pandemic, on SWB are inconsistent. Although there is some evidence that such stressors are deleterious to SWB and exacerbate other mental health issues (e.g., Cheng et al., 2020; Paredes et al., 2021, Zacher & Rudolph, 2021), others have found no impact of macro-level stressors on SWB (e.g., Bonanno et al., 2006; Lau et al., 2008). These latter findings are consistent with the theory of SWB homeostasis, which posits that resilience emerges from the active maintenance of SWB within a homeostatic range (Cummins & Lau, 2004). Due to these inconsistent findings, we first tested the associations between pandemic-related stress and SWB.
COVID-19 Impacts on Older Adults
Although older adults typically report levels of SWB similar to those reported by younger adults (Braun et al., 2017; Lyubomirsky et al., 2005), the COVID-19 pandemic may have had unique physical, psychological, and social impacts on older adults due to differing levels of risk of infection and consequently different levels of fear of contracting COVID-19. A one-year longitudinal study of Taiwanese older adults found that those who perceived themselves to be at increased risk of infection reported greater fear of COVID-19 at baseline (Li et al., 2021) and follow-up, with higher levels of fear exhibited during more severe outbreak periods (Kuo et al., 2021). A follow-up study examining fear of COVID-19 cross-nationally in a sample of older adults in Iran and Taiwan reported higher COVID-19-related fear in the Iranian sample, underscoring the importance of considering the influences of broader macro-level contextual factors on older adults SWB (Pakpour et al., 2021). Recent work has also found that material deprivations (e.g., poor nutrition) using indicators such as socioeconomic status further exacerbated COVID-19-related mental distress in older adults (Vicerra, 2022; Vicerra et al., 2022).
Older adults were not only the most vulnerable to being infected with the pathogen, which made social distancing vital; they were also at heightened risk of being socially isolated. Older adults were already more susceptible to loneliness and social isolation prior to the pandemic due to diminishing social networks because of normative and age-related events in later life (e.g., bereavement, retirement, worsening health) (Coyle & Dugan, 2012). The generally lower levels of technology proficiency in this population further hindered older adults’ ability to remain socially engaged through virtual means during the pandemic (Sixsmith et al., 2022). Thus, it is possible that older adults may have experienced greater pandemic-related stress and/or greater declines in SWB compared to younger adults due to the age-related health and social implications of the COVID-19 pandemic.
However, research examining the psychosocial impacts of the pandemic in a U.S.-based sample aged 18 to 92 reported that age was negatively associated with stress, depressive symptoms, anxiety, and loneliness (Minahan et al., 2021), suggesting that older adults may be more resilient to the unique challenges presented by the pandemic. Findings from Spain similarly show older adults’ psychosocial resilience to the COVID-19 pandemic: despite being more worried about the pandemic, older adults adapted better to lockdown and reported greater life satisfaction, resilience, happiness, and adaptive coping than younger adults (Morales-Vives et al., 2020). Given potential age-related differences in individuals’ psychosocial responses to the pandemic, we examined whether the relationship between COVID-19-related stress and SWB varied across age.
Social Resources as Mediators
Van Tilburg et al. (2020) propose three pathways by which the COVID-19 pandemic may impact well-being: 1) reduced frequency of social contact; 2) personal losses, such as diminished activity participation, loss of social contacts, and bereavement; and 3) media consumption. Lockdown and social distancing measures may also have potentially long-standing impacts on social functioning – including through suppressed social interactions and loss of social bonds (Okruszek et al., 2020). Because social resources are a robust predictor of subjective assessments of quality of life across adulthood (Villas-Boas et al., 2019), drastic changes in social contact resulting from pandemic-related measures may help explain the pandemic's impact on SWB. Prior research supports that access to social resources during the early days of the pandemic impacted individuals’ well-being. Krendl and Perry (2021), for example, found that participants who experienced decreased closeness to their social network reported greater increases in depressive symptomology, irrespective of loneliness. Further, Zacher and Rudolph (2021) found that the use of social resources as coping mechanisms (e.g., emotional support) was significantly associated with higher positive affect and lower negative affect.
The onset of pandemic-related containment measures changed the structure and nature of individuals’ social resources. For example, research examining Google trends showed that the search volume for the term ‘loneliness’ was the highest ever recorded between February and March 2020 since Google began documenting search trends in 2004 (Banerjee et al., 2020). In older adults, higher levels of loneliness significantly predicted increases in depressive symptoms (Krendl & Perry, 2021). Prior work examining the effects of pandemic-related stress on mental health found that social support mediated the relationships between pandemic-related stress and depression, anxiety, and loneliness (Minahan et al., 2021). Additionally, social isolation has been linked to experiences of loneliness, and both loneliness and social isolation influence stress appraisals, which in turn, may adversely impact physical health, anxiety, and depression (Golden et al., 2009; Kearns et al., 2015). A 2023 report issued by the U.S. Surgeon General indicated that the mortality impact of social isolation was similar to that caused by lack of exercise, obesity, and smoking (Murthy, 2023). This highlights the importance of social resources for physical health and underscores the need to examine how social resources influence the perceptions and impacts of stress.
Furthermore, Cacioppo et al. (2011) described resilience as “the capacity to foster, engage in, and sustain positive relationships and to endure and recover from life stressors and social isolation” (p. 44), suggesting that resilience may, in part, be contingent on one's social resources. Although social isolation poses a risk to health and well-being, the presence, availability, and perception of support from one's social network may protect against poor psychosocial outcomes. Those who are socially isolated, living alone, and/or have limited access to and use of the internet may be disproportionately at risk for experiencing the negative impacts of social isolation. Alternatively, those with strong support may have sufficient resources to combat psychological distress (Cacioppo & Cacioppo, 2018). Thus, the current study examines the role of social resources – namely social support, social isolation, and loneliness – as mediating influences in the relationship between pandemic-related stress and SWB across age.
The Current Study
The Transactional Model of Stress and Coping (Lazarus & Folkman, 1984) proposes that stress arises due to complex and dynamic transactions between an individual and their environment and suggests that individuals evaluate the significance of stressors (primary appraisal) and their own perceived resources (e.g., social resources) to manage emotions or confront the stressor at hand. Using this model as a guiding theoretical framework, the current study seeks to expand upon previous research on pandemic-related stress by examining its associations with SWB across age, and to explore how social resources further influence this relationship. Gaining a greater understanding of the differential role that age and social resources play in the relationship between pandemic-related stress and SWB can inform the development of targeted interventions aimed at fostering coping and resilience during and in the aftermath of major life events (Lau et al., 2008), such as the COVID-19 pandemic.
The current study had three specific aims. First, we sought to examine the relationship between pandemic-related stress and SWB (defined here as life satisfaction, positive affect, and negative affect) among adults during the first peak of the pandemic in the U.S. Second, we examined whether age moderated these relationships to better understand age-related differences in individuals’ psychosocial responses to the pandemic. Finally, in line with Van Tilburg et al.'s (2020) hypothesis that the pandemic may impact well-being through reduced social contact and/or personal losses (e.g., loss of participation in social activities, loss of social contacts) we tested three social resources, namely social support, social isolation, and loneliness, as mediators of the relationship between pandemic-related stress and SWB.
We hypothesized that greater stress associated with the COVID-19 pandemic would be associated with lower life satisfaction and positive affect, and positively associated with negative affect. Our analysis of age moderation in this relationship was exploratory because of the mixed findings in the existing literature regarding age-related differences in pandemic-related stress, coping, and SWB. We also hypothesized that individuals’ social resources, namely social support, social isolation, and loneliness, would mediate the relationship between higher pandemic-related stress and disrupted SWB based on Van Tilburg et al. (2020)'s theoretical proposal.
Method
Participants
Participants (N = 1,354) aged 18–92 were recruited to participate in an online survey examining social distancing and psychological well-being through social media posts and ResearchMatch.org, an online registry of prospective research participants. To be eligible to participate, individuals confirmed that they were at least 18 years old, fluent in English, and provided informed consent. Data were collected during the first peak of the COVID-19 pandemic in the U.S., corresponding to the initial implementation of social distancing measures; all data were collected between April 1, 2020 and May 17, 2020. The survey contained items to ensure that participants were attending to the survey (e.g., “For psychometric purposes, please select ‘All of the time’”). After examination of responses to these items, data from 36 participants (2.7%) were excluded due to failing one or more of these attention checks. The resulting analytic sample comprised 1,318 participants (Mage = 52.42, SD = 17.76). The majority of participants identified as female (77.01%) and White (86.95%). Participant characteristics and descriptive statistics for the study variables are presented in Table 1.
Participant Characteristics and Descriptive Statistics for Study Variables.
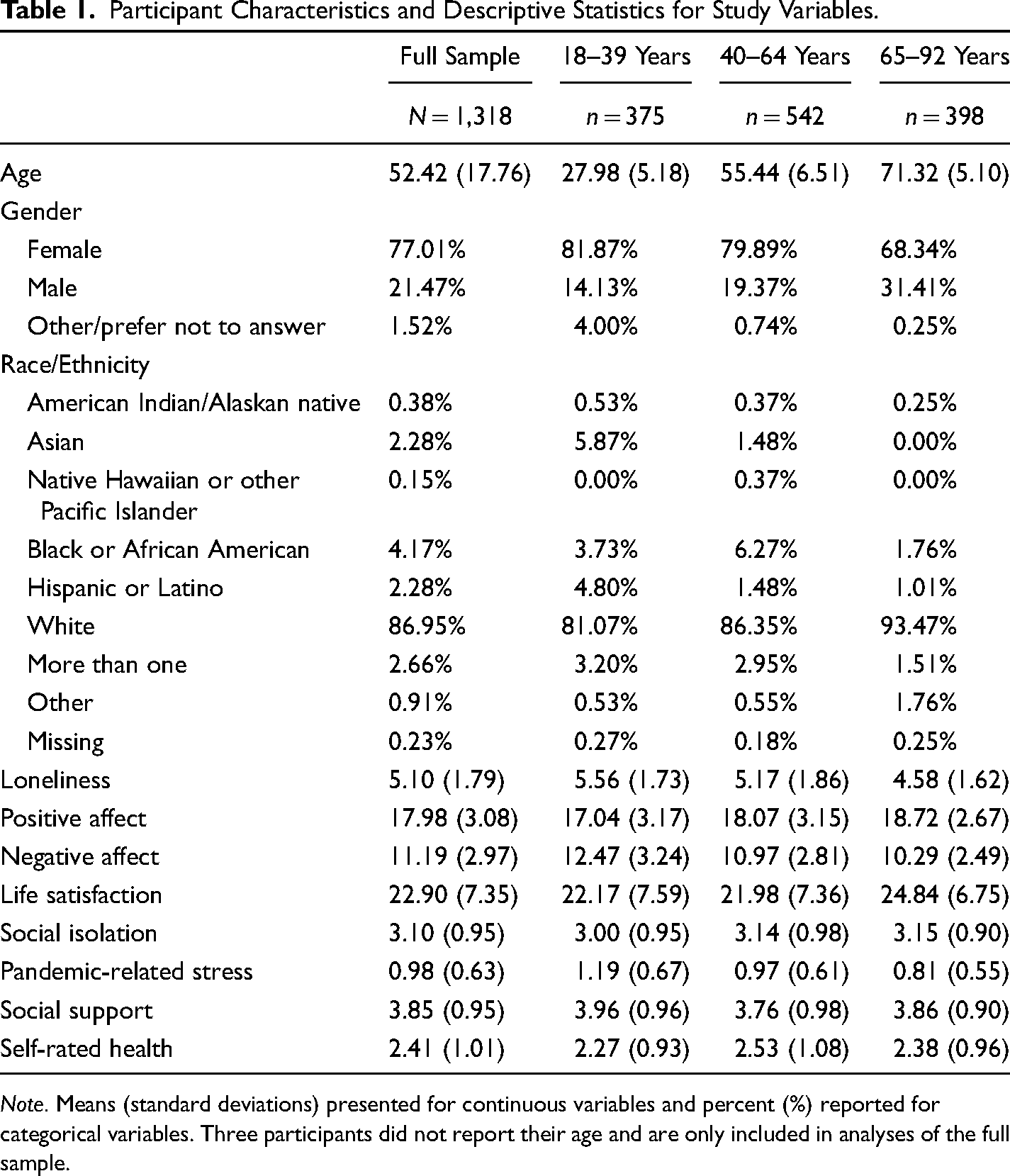
Note. Means (standard deviations) presented for continuous variables and percent (%) reported for categorical variables. Three participants did not report their age and are only included in analyses of the full sample.
Procedure
Data were collected through the Qualtrics survey platform. The survey included measures of loneliness, social contact, social support, pandemic-related stress, coping, subjective well-being, anxiety, depression, health locus of control, and sociodemographic characteristics. Participants were also asked to respond to open-ended items asking about their experiences with social distancing (e.g., “How has social distancing changed your daily life?”) as well as how long they had been engaged in social distancing. Participants were given the option to enter a raffle for one of two $100 gift cards as compensation for their time by entering their email address into a separate survey. The study was approved by the Fordham University Institutional Review Board; additional details regarding the study design can be found elsewhere (Minahan et al., 2021).
Measures
Study measures are described below. Cronbach's alphas for the current sample for each scale are presented in the diagonal of the correlation matrix (Table 2).
Zero-Order Correlations Among Study Variables.
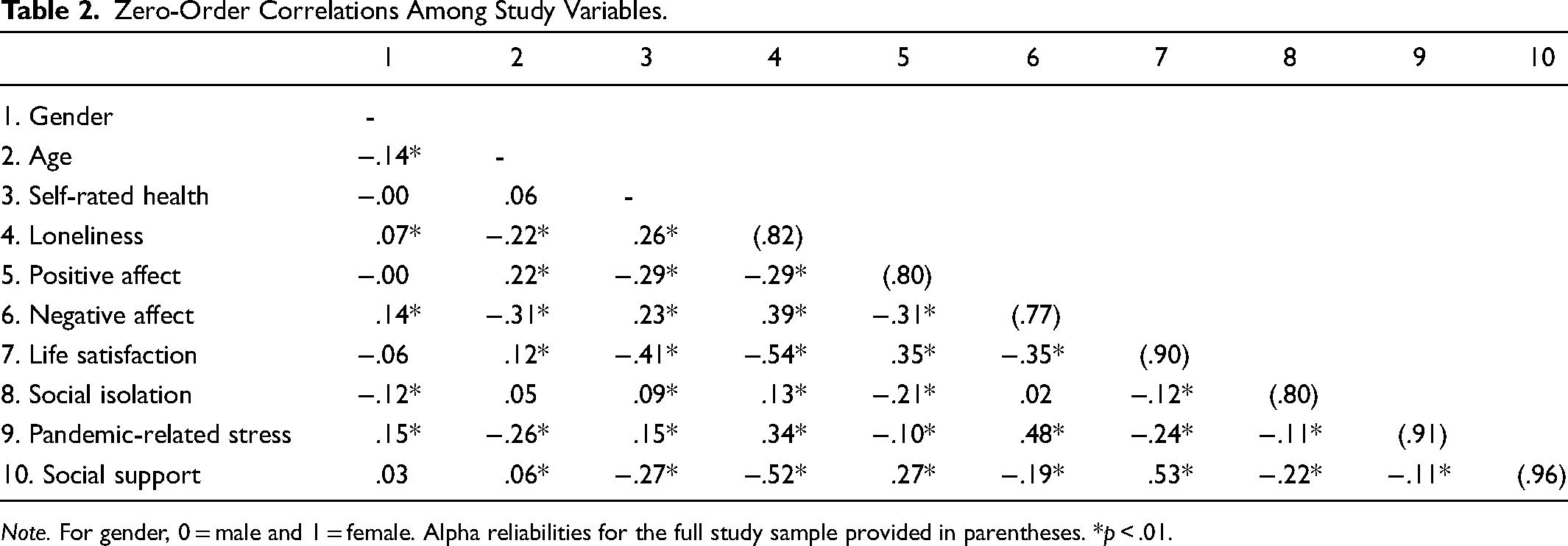
Note. For gender, 0 = male and 1 = female. Alpha reliabilities for the full study sample provided in parentheses. *p < .01.
Pandemic-Related Stress
The Impact of Events Scale – Revised (IES-R; Weiss & Marmar, 1997), a measure of posttraumatic stress, was used to assess participants’ COVID-19 pandemic-related stress “during the past seven days with respect to the Coronavirus Pandemic.” Participants were instructed to respond to 22 items such as “I thought about it when I didn't mean to” and “I tried not to think about it” on a five-point Likert scale (0 = not at all to 4 = extremely). A total score was calculated as the mean of responses to all 22 items with higher scores indicating higher levels of pandemic-related stress. The IES-R has high reliability and validity in both clinical and community samples (Creamer et al., 2003) and has been validated for use as a self-report measure of posttraumatic stress following the COVID-19 pandemic (Aljaberi et al., 2022).
Life Satisfaction
Life satisfaction was measured with the Satisfaction with Life Scale (SWLS; Diener et al., 1985). The SWLS asks participants to evaluate their life satisfaction in response to five items (e.g., “So far I have gotten the important things I want in life”) on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). Responses are summed with higher scores representing higher life satisfaction. The reliability and validity of the SWLS has been demonstrated in diverse populations (Pavot & Diener, 2009).
Positive and Negative Affect
A shortened version of the Positive and Negative Affect Schedule (PANAS-SF; Thompson, 2007; Watson et al., 1988) was used to measure affect. The PANAS-SF is a 10-item scale comprising five positive (e.g., “inspired”) and five negative (e.g., “afraid”) adjectives. Participants rated the extent to which they generally felt this way on a five-point Likert scale (1 = very slightly or not at all to 5 = extremely). Responses to the positive and negative items were summed, resulting in a positive affect score and a negative affect score, with higher scores on both corresponding to higher levels of positive or negative affect, respectively. The PANAS-SF is considered a reliable and valid measure of affect (α = .75 for positive affect and .76 for negative affect, eight-week test-retest reliability of r = .84; Thompson, 2007).
Loneliness
The Three-Item Loneliness Scale (Hughes et al., 2004), derived from the Revised UCLA Loneliness Scale (Russell et al., 1980), asks participants to rate how often (1) they lack companionship, (2) feel left out, and (3) feel isolated from others, on a three-point scale (1 = hardly ever to 3 = often). Responses are summed with higher scores indicating higher levels of loneliness. The psychometric properties of the Three-Item Loneliness scale, including reliability, internal consistency, and discriminant and convergent validity, are well-established across diverse samples (Hawkley et al., 2020; Hughes et al., 2004; Lin et al., 2022).
Social Isolation
Social isolation was measured by asking participants about their relationships with their children, family, and friends. Four items assessed the composition of their social networks (e.g., “Do you have a husband, wife or partner with whom you live?”). Four items measured the closeness of these relationships (e.g., “How many of these family members would you say you have a close relationship with?”), and 15 items assessed the ways in which participants maintain contact with their social networks (e.g., “How often do you speak on the phone?”; “How often do you communicate by Skype, Facebook, or other social media?”) (Schuster et al., 1990; Turner et al., 1983). Participants responded to these items on a six-point Likert scale (1 = three or more times a week to 6 = less than once a week or never; Smith et al., 2017). A social isolation score was calculated as the mean of the 15 items assessing the frequency of contact, with higher values corresponding with less frequent social contact (i.e., higher social isolation). Given their nature, these items are not intended to have a high degree of internal consistency (Smith et al., 2013).
Social Support
The Medical Outcome Study–Social Support Survey (MOS-SSS; Sherbourne & Stewart, 1991) comprises 18 items asking participants to rate how often each type of support is available to them on a five-point Likert scale (1 = none of the time to 5 = all of the time). These items assess four dimensions of social support: emotional/informational support (e.g., “Someone to confide in or talk to about yourself or your problems”), tangible support (e.g., “Someone to help with daily chores if you were sick”), affectionate support (e.g., “Someone who shows you love and affection”), and positive social interaction (e.g., “Someone to do something enjoyable with”). A total score is calculated as the mean of responses to all 18 items. This scale has been shown to be highly reliable and valid (Sherbourne & Stewart, 1991).
Demographic Variables and Covariates
Participants completed items measuring self-reported sociodemographic characteristics including age (“what age did you turn at your last birthday?”) and gender identity. Health was measured by one item asking, “How would you rate your health at the current time?” with answer options ranging from excellent (coded as 1) to poor (coded as 5). These variables were included in analyses as covariates. Gender was dichotomized into male (n = 283) and female (n = 1,015) since the number of individuals who reported being gender-variant/non-conforming (n = 15) or other (n = 4) were too few to include in the analyses. Participants’ race/ethnicity was also included as a covariate in all analyses, however, because the majority of participants (87%) were White, race was also treated as a binary variable (White/non-White) to ensure adequate statistical power.
Data Analytic Method
Structural equation modeling with AMOS 25.0 (Arbuckle, 2017) was used to examine the relationship between pandemic-related stress and the three facets of subjective well-being (positive affect, negative affect, and life satisfaction). The subjective well-being outcomes were modeled with latent variables; the predictor variable (pandemic-related stress), mediator variables (social isolation, loneliness, and social support), and covariates (age, gender, race/ethnicity, self-rated health) were included as observed variables. Model fit was assessed with several fit indices including chi-square (χ2), chi-square ratio (χ2/df), the root mean square error of approximation (RMSEA), and the comparative fit index (CFI). For chi-square, chi-square ratio, and RMSEA, values closer to zero indicate a better model fit. Specifically, RMSEA values < .06 indicate a good fit, and values < .08 indicate an acceptable fit (Browne & Cudeck, 1993; Hu & Bentler, 1999). For the CFI, higher values are indicative of a better model fit, with values ≥ .95 (Hu & Bentler, 1999) indicating a good fit and values ≥ . 90 (Kline, 2011) indicating an acceptable fit.
Age moderation analyses were conducted by dividing the sample into three subsamples reflecting younger adults (ages 18–39 years), middle-aged adults (40–64 years), and older adults (65–92 years) and examining whether the magnitude of the relationship between the predictor and the outcome variable differed across age. Age cut-offs are arbitrary, but there is precedent for using these specific age ranges. Age 40 is often used in research to denote the beginning of middle-age (e.g., Lachman et al., 2015). Age 65 is the age in the United States at which individuals may begin to qualify for full Social Security benefits, and is often used to denote the lower threshold of older age (e.g., Shenkin et al., 2017). Furthermore, these specific age cut-offs are consistent with previous work using these data (Minahan et al., 2021).
Before making comparisons across age, it is important to provide evidence of invariance of the latent constructs across the three age groups so that differences across groups can be interpreted unambiguously (Horn & McArdle, 1992). Thus, before examining age moderation, we evaluated the fit of a three-factor model comprising life satisfaction, positive affect, and negative affect. Configural invariance (i.e., invariant factor structure across groups; Horn et al., 1983) was assessed by evaluating the overall fit of the model across the three age groups. Metric invariance (i.e., invariant factor loadings; Horn & McArdle, 1992) was evaluated by examining the difference in fit between a constrained model (in which the magnitudes of each respective unstandardized factor loading were constrained to be equal across the three age groups) and the unconstrained configural invariance model. Because χ2 is sensitive to sample size, a change in CFI may provide a better assessment of difference in fit. Cheung and Rensvold (2002) suggest that a change in CFI greater than .01 is indicative of a substantially different fit between the models.
All mediation analyses were conducted in AMOS with 5,000 bootstrap samples. Bootstrapping methods in AMOS require no missing data, thus missing data (less than .02%) were addressed with linear interpolation. Baron and Kenny (1986) recommend that mediation analyses are appropriate only when the independent variable is a significant predictor of the dependent variable. Thus mediation analyses were not conducted unless pandemic-related stress was a significant predictor of the outcome variable.
Full-information maximum likelihood estimation was used to deal with missing data, except for the mediation analyses in which linear interpolation was used. A p value of .01 was used for the analyses.
Results
Zero-order correlations among study variables are presented in Table 2 for the full sample. Consistent with our hypotheses, higher pandemic-related stress was significantly associated with lower positive affect (r = −.10) and life satisfaction (r = −.24), as well as higher negative affect (r = .48). Older age was positively associated with greater levels of positive affect (r = .22) and life satisfaction (r = .12), and negatively associated with greater levels of negative affect (r = −.31).
Preliminary analyses were conducted to evaluate configural invariance of a three-factor model comprising life satisfaction, positive affect, and negative affect across the three age groups (younger, middle-aged, and older). The configural invariance model fit the data well (χ2 = 777.032, df = 261; χ2/ df =2.98; CFI = .938, RMSEA = .039). Subsequently, constraining the magnitudes of the unstandardized coefficients to be invariant across the three age groups to examine metric invariance of the three-factor model did not result in a worse fit; there was a minimal decrease in the CFI (Δ in CFI = .004), and there was also a minimal decrease in the RMSEA (.039 reduced to .038), in which lower values indicate a better fit. These findings provide evidence of measurement invariance and support making comparisons across the age groups for the moderation analyses.
Positive Affect
The influence of pandemic-related stress on positive affect was first examined in the total sample. In this model (model fit: χ2 = 367.58, df = 25; χ2/ df =8.51; CFI = .868, RMSEA = .102), in which age, gender, race, and self-rated health were included as covariates, pandemic-related stress was not a significant predictor of positive affect (β = −.01). To examine whether age moderated the relationship between pandemic related-stress and positive affect, the sample was divided into three age groups reflecting young (ages 18–39, n = 375), middle-aged (ages 40–64, n = 542), and older adults (ages 65–92, n = 398). Pandemic-related stress was not a significant predictor of positive affect in any age group (standardized coefficients ranged from .00 to −.06) indicating that age did not moderate the relationship. Because there were no significant relationships, mediation analyses were not conducted.
Life Satisfaction
In the total sample, pandemic-related stress was a significant predictor of life satisfaction (β = −.16; model fit: χ2 = 212.64, df = 25; χ2/ df = 8.51; CFI = .946, RMSEA = .083), even after controlling for age, gender, race, and self-rated health. Age was not a significant moderator in this relationship, as evidenced by overlapping 95% confidence intervals across age groups for the coefficients reflecting the relationship between pandemic-related stress and life satisfaction (βs = −.16, −.12, and −.26, ps < .01, in the younger, middle-aged, and older adult groups, respectively). Overlapping confidence intervals indicate that the magnitude of the coefficients does not differ across the age groups.
Follow-up analyses were conducted to examine whether the significant relationship between pandemic-related stress and life satisfaction is mediated by the social resource variables. Because there was no evidence of age moderation, these mediation analyses were conducted across the full sample.
The standardized coefficients for the mediation analyses, when the life satisfaction construct was the dependent variable, are presented in Table 3. The model in which loneliness was added as a mediator fit adequately (model fit: χ2 = 331.42, df = 33; χ2/df = 10.04; CFI = .947, RMSEA = .083). Loneliness completely mediated the relationship between pandemic-related stress and life satisfaction; the magnitude of the relationship diminished from −.20 (p < .01) to −.04 (ns). The indirect effect was significant (−.17, p < .01).
Standardized Estimates from Mediation Models Examining Effects of Pandemic-Related Stress on Life Satisfaction via Social Resource Variables.
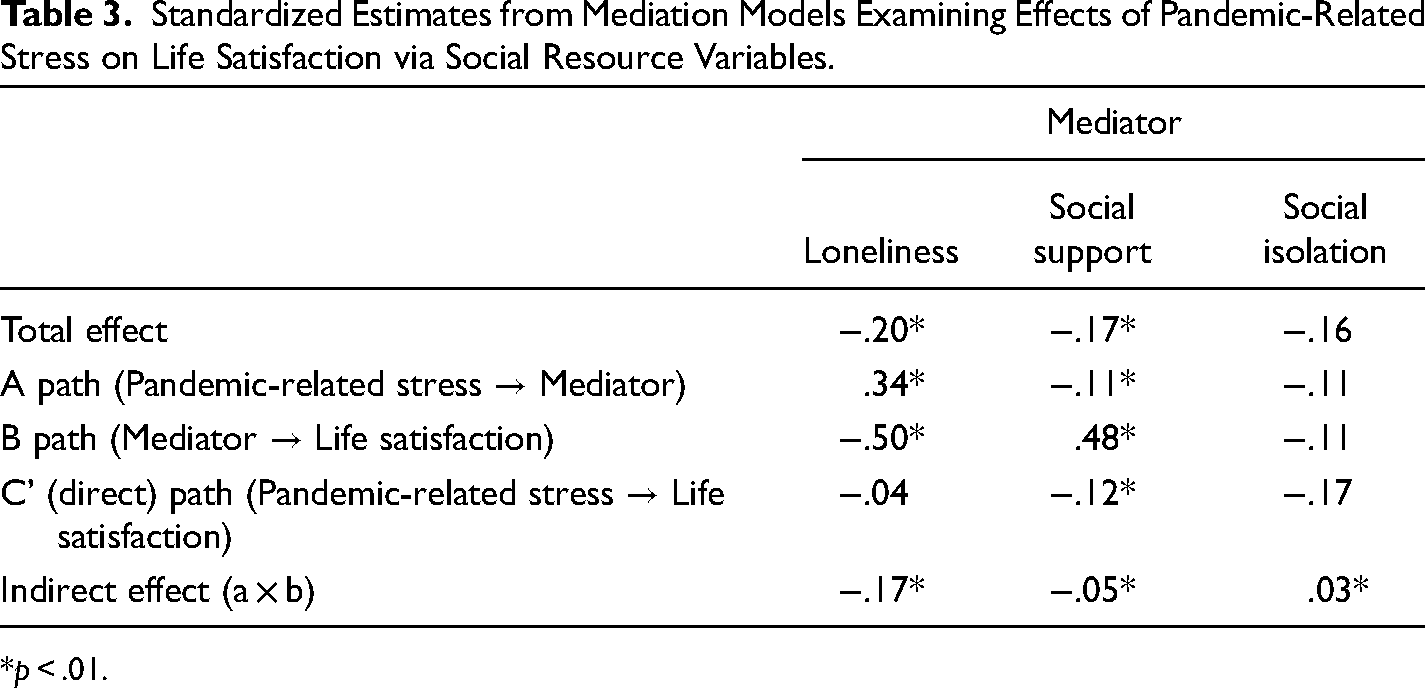
*p < .01.
When social support was entered into the model as a mediator (χ2 = 338.68, df = 33; χ2/df = 10.26; CFI = .944, RMSEA = .084), the relationship between pandemic-related stress and life satisfaction diminished in magnitude from −.16 (p < .01) to −.12 (p < .01) but was still significant. The indirect effect was significant (−.05, p < .01), indicating that social support was a partial mediator of the pandemic-related stress-life satisfaction relationship (see Table 3).
When social isolation was included in the model as a mediator (χ2 = 249.63, df = 33, χ2/df = 7.56; CFI = .957, RMSEA = .071), the standardized coefficients changed from −.16 (p < .01) to −.17 (p < .01), and the indirect effect (.03, p < .01) was significant (see Table 3).
Negative Affect
In the total sample, pandemic-related stress was a significant predictor of negative affect, even after controlling for age, gender, race, and self-rated health (β = .46; model fit χ2 = 215.72, df = 25, χ2/ df = 8.63; CFI = .926, RMSEA = .076). The predictive validity of pandemic-related stress was not significantly moderated by age, as demonstrated by the overlapping confidence intervals for the standardized coefficients from pandemic-related stress to negative affect (.43, .48, and .56, all ps < .01) across young, middle-aged, and older adult subsamples, respectively.
Because pandemic-related stress significantly predicted negative affect, follow-up analyses were conducted to examine the social resource variables as mediators. Mediation analyses were again conducted with the total sample since there was no evidence of age moderation. Results are presented in Table 4.
Standardized Estimates from Mediation Models Examining Effects of Pandemic-Related Stress on Negative Affect via Social Resource Variables.
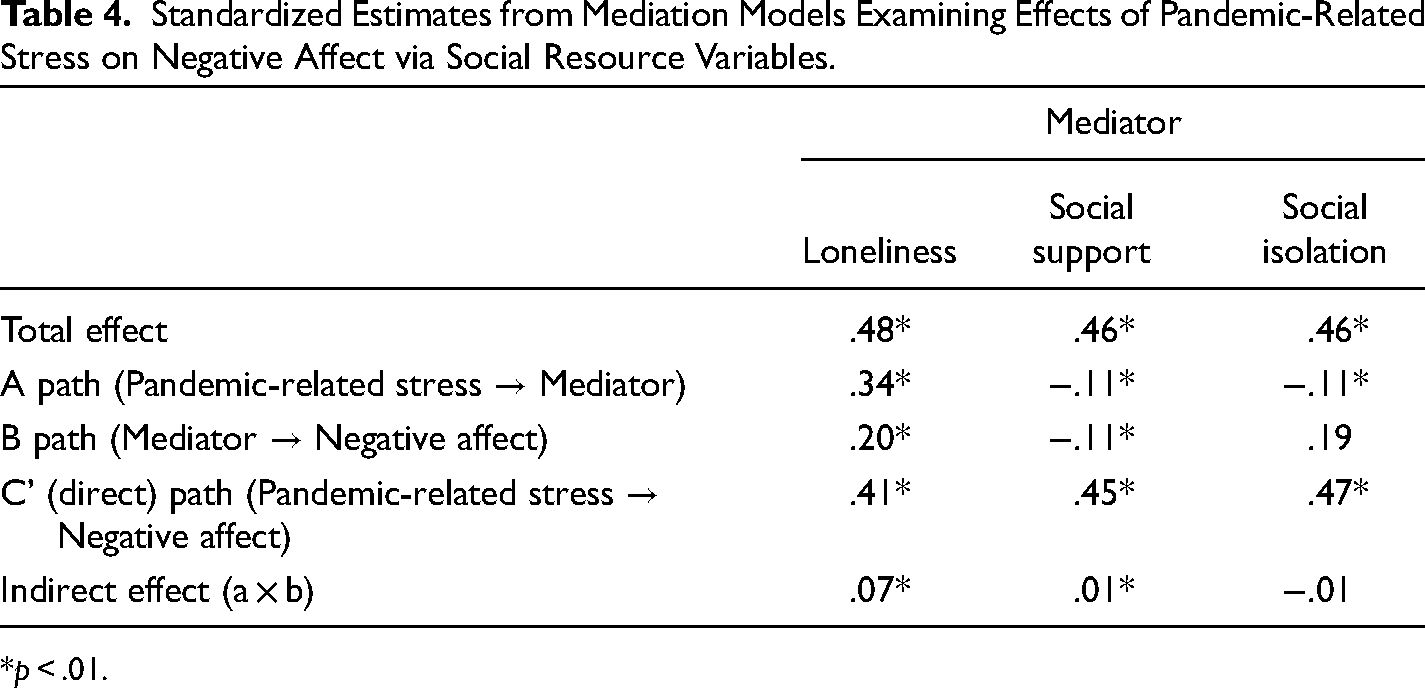
*p < .01.
Including loneliness as a mediator in the model (model fit: χ2 = 369.58, df = 33, χ2/df = 11.19; CFI = .885, RMSEA = .089) slightly reduced the magnitude of the relationship between pandemic-related stress and negative affect. Specifically, the standardized coefficient was reduced from .46 (p < .01) to .41 (p < .01). The indirect effect was significant (.07, p < .01).
When social support was included as a mediator (model fit: χ2 = 343.54, df = 33; χ2/df = 10.41; CFI = .886, RMSEA = .085) in the model, the standardized coefficient between pandemic-related stress and negative affect was reduced from .46 (p < .01) to .45 (p < .01). The standardized indirect effect was small but significant (−.01, p < .01).
Social isolation did not mediate the relationship between pandemic-related stress and negative affect; the standardized coefficient increased slightly from .46 (p > .01) to .47 (p < .01) (model fit: χ2 = 263.26; df = 33; χ2/df = 7.98; CFI = .913, RMSEA = .073), and the standardized indirect effect was not significant (−.01, ns).
Discussion
The negative mental health impacts of COVID-19 pandemic-related stress on adults are well-documented (e.g., Banerjee & Rai, 2020; Minahan et al., 2021; O’Connor et al., 2021). The purpose of the current study was to build on this existing research by specifically exploring the impact of pandemic-related stress on SWB and examining how social resources may serve as mediating influences in this relationship among a sample of adults living in the U.S. during the first wave of the pandemic. Our results showed that stress associated with the COVID-19 pandemic predicted lower life satisfaction and higher negative affect, but was unrelated to positive affect, which is partially consistent with prior research. Zacher and Rudolph (2021), for example, reported that higher perceived stress was associated with lower life satisfaction, positive affect, and greater negative affect, and Macdonald & Hülür (2021) found that loneliness and negative affect increased, while positive affect decreased, over time during the period when shelter-in-place orders were enacted. That we did not detect an association between pandemic-related stress and positive affect in the structural model is noteworthy because previous work suggests that positive affect may be adaptive in promoting positive coping in response to stress (Blasco-Belled et al., 2020).
Additionally, our findings show that age did not significantly moderate the relationship between pandemic-related stress and SWB despite older adults being uniquely at risk for both physical exposure to the pathogen and diminishing social bonds. Although this is consistent with the theory of SWB homeostasis (Cummins & Lau, 2004), our findings add to a growing body of research documenting older adults’ resilience in response to stress within the unique context of the COVID-19 pandemic. There are several hypotheses regarding older adults’ resilience. For example, Lind et al. (2021) posit that older adults are better at finding meaning in challenging times and use memories of past challenges through which they have persevered to help regulate their negative emotions and direct their behavior, thus allowing them to effectively cope with the implications of the pandemic.
When examining the relationship between social resources and SWB, we found that both social support and loneliness were associated with the three facets of SWB in the expected directions. Subsequent mediation analyses examined whether the variance in the relationship between pandemic-related stress and the SWB outcomes of life satisfaction and negative affect could be attributed to the social resource variables. Results showed that loneliness fully mediated the relationship between pandemic-related stress and life satisfaction, and partially mediated the relationship between pandemic-related stress and negative affect. Social support partially mediated the relationship between pandemic-related stress and both life satisfaction and negative affect. Social isolation did not mediate the relationship between pandemic-related stress and negative affect. And, while there was a significant indirect effect via social isolation on life satisfaction, the total effect was slightly smaller than the direct effect, thus social isolation did not meaningfully explain the effect of pandemic-related stress on life satisfaction. As discussed by Killgore et al. (2020), there was a “significant surge” in loneliness in April 2020, the levels of which exceeded the cut-off for high levels of loneliness in 43% of the respondents in their study. Our findings provide additional support to the growing body of literature linking the importance of social connectedness to health and well-being outcomes, and suggest that loneliness can help explain the negative effects of pandemic-related stress on SWB, particularly life satisfaction (e.g., Blasco-Belled et al., 2020; Foa et al., 2020; Okruszek et al., 2020).
Consistent with the literature underscoring the importance of social support (e.g., Cacioppo & Cacioppo, 2018; Cornwell & Waite, 2009; Hsu & Tung, 2010; Nemeroff et al., 2010), our results showed that access to social support partially explained the effects of pandemic-related stress on life satisfaction and negative affect. Although related constructs, loneliness and social support are distinct from social isolation and reflect different dimensions of individual differences in the literature (e.g., Beller & Wagner, 2018; Coyle & Dugan, 2012). As is customary, social isolation comprised an objective assessment of frequency of contact whereas loneliness and social support incorporated a subjective assessment. The finding that loneliness and social support partially mediate the relationship between pandemic-related stress and SWB suggests that one of the ways in which the COVID-19 pandemic negatively impacts well-being is through reduced social interactions and individuals’ perceptions of the quality of their social support network (Van Tilburg et al., 2020). Although this finding is promising because it suggests that decreasing loneliness and increasing social engagement may protect SWB despite the stress associated with the pandemic, it is simultaneously concerning as one of the long-lasting implications of the measures put in place to mitigate the spread of COVID-19 (e.g., social distancing, shelter-in-place orders) may be impoverished social bonds (Okruszek et al., 2020).
From a practical perspective, these findings suggest that increased attention should be placed on identifying methods for creating and maintaining interpersonal relationships and social interactions, which are crucial for health and well-being. Although there are a myriad of interventions designed to facilitate social support and mitigate loneliness, findings regarding their effectiveness pre-pandemic are mixed (for a review, see Poscia et al., 2018). Internet-based interventions are one avenue through which to promote social connectedness, but online interventions aiming to decrease loneliness have largely focused on older adults, and empirical evaluations of these interventions have demonstrated only small effects (Jarvis et al., 2020). Our findings suggest that increasing social contact may be an effective way to combat negative affect and improve life satisfaction resulting from pandemic-related stress, highlighting the need for interventions targeting social connectedness and engagement among all adults.
Interventions leveraging the popularity of social media and social networking sites may be efficient and effective ways to increase social contact because the vast majority of adults in the U.S. use social media (Auxier & Anderson, 2021) and there is evidence that older adults’ use of social networking sites is associated with greater quality of life in terms of mental health (Siah et al., 2023). Research conducted among older adults in the U.S. prior to and during the onset of the pandemic reports increased physical isolation as a result of lockdown measures, but no change in digital isolation, suggesting that older adults are able to use social media and networking sites to maintain social connectedness when barriers to in-person contact are present (Peng & Roth, 2022). Given that technology-based interventions can effectively target loneliness and social isolation (Poscia et al., 2018), additional efforts to connect adults to such technologies – including social media and social networking sites – should be implemented. Furthermore, interventions aimed at increasing the perceived quality of social interactions on social media and social networking sites may also help older adults develop and maintain social bonds, thereby decreasing feelings of loneliness without simultaneously increasing the amount of time individuals spend on social media.
Limitations and Conclusions
The current findings should be considered in the context of this study's limitations, which include its cross-sectional nature and the homogeneity of the sample. Although we accounted for participants’ gender and race in all analyses, the majority of our sample identified as female and/or White which may limit the generalizability of these findings. This is an important consideration given the disproportionate impact the COVID-19 pandemic has had on women (Zamarro & Prados, 2021; Zhang et al., 2021) and communities of color (van Dorn et al., 2020), and research identifying racial/ethnic differences in stress appraisals (Brown et al., 2020). Despite these limitations, this study provides novel data about the impacts of COVID-19-related stress on SWB, as well as the role of social factors in mediating this relationship. Research on prior epidemics suggests that the mental health impacts of macro-level stressors such as the COVID-19 pandemic are likely to outlast the physical threat of illness (Ornell et al., 2020; Reardon, 2015; Shigemura et al., 2020), making the study of SWB an important line of inquiry as discussions focus on recovery from the pandemic. Our findings indicate that pandemic-related stress is associated with lower levels of life satisfaction and greater negative affect, and that increasing social support and reducing loneliness may be effective ways to promote SWB, suggesting that increased social contact may be particularly important for preserving SWB among individuals experiencing high levels of pandemic-related stress.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Approval
APA ethical standards were followed and all procedures were approved by the Fordham University Institutional Review Board.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institute on Aging, (grant number K99AG073509, R00AG073507).