
Abstract
This study examines the association between yoga practice and multidimensional health outcomes among older adults in India using nationally representative data from LASI Wave 1 (2017–2018). The analysis includes 28,482 individuals aged 60 years and above. Yoga participation was categorized by frequency, and its association with cognitive function, social engagement, physical activity, sleep quality, depressive symptoms, functional health, and life satisfaction was assessed. Older adults who practiced yoga demonstrated better cognitive performance, greater social participation, higher life satisfaction—particularly among daily practitioners—improved sleep quality, and higher levels of physical activity. Daily yoga practice was also associated with fewer depressive symptoms and functional limitations. However, yoga participation across all frequencies was linked to increased reports of pain. A mixed dose–response pattern suggests that more frequent practice is associated with more favorable physical and mental health outcomes. These findings support integrating yoga-based interventions into public health strategies to promote healthy aging in India.
Introduction
India's population is undergoing a steady demographic transition towards aging (Agarwal et al., 2016). Aging is associated with progressive declines in physical and mental health, including reductions in balance, muscle strength, flexibility, gait speed, and overall stability (Borah et al., 2008; Dsouza et al., 2014; Khanuja et al., 2018; Mohammed et al., 2021; Wang et al., 2024; Yang et al., 2018). These changes increase the risk of impaired mobility, falls, injuries, and functional disability, often resulting in loss of independence and increased need for institutional care (Bartosch et al., 2020; Davis et al., 2011; Muneera et al., 2023; Sasidharan et al., 2020; Srivastava & Muhammad, 2022; Stewart Williams et al., 2015; Thakkar et al., 2022). In addition, older adults frequently experience shifts in social roles, relationships, and self-perception, contributing to a higher prevalence of depression and poorer psychological well-being (Ohrnberger et al., 2017). These challenges highlight the growing need for accessible and effective strategies to promote healthy aging.
Yoga, a widely practiced mind–body intervention in India, has gained attention for its potential to be associated with multiple dimensions of health among older adults. Existing evidence suggests that yoga is associated with improvements in balance, flexibility, muscle strength, sleep quality, and overall physical functioning as well as reductions in depressive symptoms (Mooventhan & Nivethitha, 2017; Sivaramakrishnan et al., 2019). Randomized controlled trials have further demonstrated benefits in physical performance and quality of life following structured yoga interventions (Ganesh et al., 2022). Additionally, yoga has been associated with cognitive improvements, particularly in attention, memory, and executive functioning (Gothe & McAuley, 2015; Hariprasad et al., 2013). Yoga, particularly chair and Kundalini styles, may enhance cognition, mood, and balance among individuals with mild cognitive impairment or dementia; however, existing evidence is limited by a high risk of bias and requires more rigorous validation (Karamacoska et al., 2023). Additionally, qualitative evidence from India indicates improvements in self-reported physical and emotional health, along with reductions in sedentary behavior among older adults participating in yoga-based practices (Gour et al., 2020).
Beyond physical and cognitive health, yoga may also provide psychosocial benefits. Group-based yoga interventions have been shown to reduce loneliness and enhance social engagement and self-esteem among older adults (Panigrahi et al., 2023). Evidence also indicates modest but meaningful reductions in depressive symptoms and anxiety, although findings remain mixed across studies and populations (Brinsley et al., 2021; Verzili et al., 2023; Wu et al., 2023). Furthermore, yoga-based interventions such as chair yoga and integrative yoga therapy have demonstrated effectiveness in reducing pain and improving functional outcomes in specific clinical populations, including those with osteoarthritis (Choudhary et al., 2019).
Despite this growing body of evidence, most studies on yoga and aging are based on small, localized samples or specific intervention settings such as yoga centers, clinics, or old-age homes. These studies often focus on a limited set of health outcomes, restricting their generalizability. There is a lack of large-scale, population-based research examining the association between yoga practice and multiple dimensions of health among older adults, particularly in the Indian context.
Using nationally representative data from the Longitudinal Ageing Study in India (LASI Wave 1), this study addresses this gap by examining how the frequency of yoga practice is associated with multidimensional health outcomes, including cognitive function (CS), physical health, and psychosocial well-being among older adults in India.
Methods
Data
The study utilized data from the LASI-Wave 1, a nationwide survey conducted between 2017 and 2018 involving 72,250 participants aged 45 years and above. LASI is a comprehensive initiative aimed at understanding aspects of population aging, along with the economic, social, and health factors involved. This is the first and only longitudinal survey in India that is representative on a national scale and focuses on the aging population within the country. Respondent units were determined using a multistage stratified area probability cluster sampling design implemented in the survey. A four-stage sampling approach was employed in urban areas, while a three-stage method was used in rural areas. The report detailing the survey includes an in-depth methodology that describes all elements of the survey design, data collection methods, ethical considerations, and measures for quality control (IIPS et al., 2020). The LASI wave 1 survey collected data from 73,396 older adults aged 45 and older across the country. The data of 6,537 (8.91%) individuals did not match after merging the Individual file with the biomarker file, and 37,924 individuals were excluded due to their age below 60 years. An additional 453 individuals (1.4%) failed to provide data on all yoga and other covariates. The final sample, comprising 28,482 participants with complete item responses, was used for the study (Supplemental Table S1).
Measures
Health-Related Outcome Variables
Cognition
CS was evaluated across five comprehensive areas, including memory (both immediate and delayed word recall), orientation (awareness of time and place), arithmetic skills (such as backward counting, serial sevens, and calculation techniques), executive function (assessed through paper folding and pentagon drawing tasks), and object naming, which was compiled from the cognition module of the Health and Retirement Study (IIPS et al., 2020). A thorough description of the various cognitive domains measured in the LASI can be found in Supplemental file 1. The summary score can vary from 0 (indicating severe impairment) to 43 (indicating high CS) (Supplemental Table S2).
Social Activity
Engaging in social activities is crucial due to their numerous benefits for individuals’ well-being and overall satisfaction. LASI inquiries about how often an individual engages in each of the following seven activities: (1) going to the movies, (2) dining out, (3) visiting a park or beach, (4) playing cards or games, (5) spending time with relatives or friends, (6) attending cultural performances or shows, and (7) participating in religious functions or events (outside of home). The response options are as follows: Daily (6), Several times a week (5), Weekly (4), Several times in a month (3), At least once a month (2), Rarely or once a year (1), and never or not applicable (0). The score ranges from 0 to 42, with higher scores reflecting greater social engagement.
Life Satisfaction
The life satisfaction of older adults was assessed using five statements: (a) In many ways, my life is nearly perfect; (b) my living conditions are outstanding; (c) I am content with my life; (d) up to now, I have achieved the important things I desire in life; and (e) if I had the chance to relive my life, I would change very little. Participants were instructed to respond using a scale of seven: “strongly disagree (1),” “somewhat disagree (2),” “slightly disagree (3),” “neither agree nor disagree (4),” “slightly agree (5),” “somewhat agree (6),” and “strongly agree (7).” The total score can range from 5 to 35, with higher scores indicating greater life satisfaction. The scale demonstrated good internal consistency in the present sample (Cronbach's α > 0.80), consistent with previous studies using LASI data.
Centre for Epidemiologic Studies Depression Scale (CES-D)
The CES-D scale originally consists of 20 items, whereas the LASI utilized a shortened 10-item version with four response categories. This shorter version features seven negative symptoms (trouble concentrating, feeling sad, low energy, fear of something, feelings of loneliness, being bothered by things, and everything feeling like a struggle) and three positive symptoms (feeling happy, hopeful, and satisfied). The choices for responses included rarely or never (less than 1 day), sometimes (1 or 2 days), often (3 or 4 days), and most or all of the time (5–7 days) concerning the week prior to the interview. For the negative symptoms, the scoring system was as follows: rarely or never (<1 day) received a score of 0, sometimes (1 or 2 days) received a score of 1, often (3 or 4 days) received a score of 2, and most or all of the time (5–7 days) received a score of 3. Conversely, the scoring for positive symptoms was reversed. The total score varies between 0 and 30, where higher scores indicate a stronger presence of depressive symptoms. In the current sample, the CES-D showed strong internal consistency (Cronbach's α ≈ 0.78).
Handgrip Strength
Grip strength is closely linked to health and mortality results. The LASI assessed grip strength in kilograms with the use of a handheld dynamometer (Smedley's Hand Dynamometer). Health researchers took two measurements of grip strength for each hand (dominant and non-dominant). In this analysis, we focused on the grip strength of the dominant hand.
Sleep Problem
Sleep problems were assessed using a composite score based on five items: difficulty falling asleep, nighttime awakenings, early morning awakening, feeling unrefreshed, and daytime napping. Each item was scored from 0 (never) to 3 (often), and summed to create a continuous score, with higher values indicating poorer sleep quality.
ADL/IADL Problem
Activities of daily living (ADL) and instrumental activities of daily living (IADL) were measured using 13 items (6 ADL and 7 IADL), each coded as 0 (no difficulty) or 1 (difficulty), and summed to generate a continuous score, where higher values indicate greater functional limitation.
Physical Activity
In the LASI, data was gathered regarding moderate and vigorous physical activities and the frequency of these activities. For moderate physical activity, participants were inquired about their participation in moderately intensive tasks such as cleaning the house, washing clothes, collecting water, drawing water from a well, gardening, walking at a moderate speed, cycling at a steady pace, and performing floor or stretching exercises. Respondents were asked about their involvement in running or jogging, swimming, going to a gym or fitness center, cycling, heavy lifting, chopping, agricultural work, fast cycling, cycling with loads, and digging with a spade or shovel as examples of intense activity.
Pain
In the LASI, every participant was inquired about whether they frequently experience pain. The answers were noted as yes (1) or no (0).
Predictor/Exposure Variable
The LASI is the inaugural national study to gather information about yoga practice, meditation, asana (physical postures), pranayama (breathing techniques), and related mind–body practices among older adults aged 45 and older across all states and Union Territories of India. Due to survey design, these were treated as a combined measure of mind–body practices. Participants were asked questions such as “have you participated in activities like yoga, meditation, asana, pranayama, and related practices,” as well as how often they engage in these activities. The frequency of yoga, meditation, asana, and pranayama was categorized as every day, >1/week, 1/week, 1–3/month, and hardly ever or never.
These practices represent commonly adopted, non-sectarian forms of yoga in community settings in India and typically emphasize gentle physical postures, breathing regulation, relaxation, and meditative awareness. These methods exemplify widely embraced, non-religious styles of yoga, generally focusing on gentle physical poses, breathing control, relaxation techniques, and mindfulness. These practices are easily accessible to older adults and are frequently engaged in for overall health, stress alleviation, and functional well-being, rather than dedicating to a particular traditional school of yoga.
Covariates
The socio-demographic variables included age (as a continuous measure); sex (male or female); place (rural, urban); marital status (currently married, widowed, and others, including divorced, separated, or never married); religion (Hindu, Muslim, or other); social categories (scheduled caste [SC] or scheduled tribe [ST], other backward classes [OBC], and others); education level (no formal education, less than 5 years, 5–10 years, and 10 years or more); monthly per capita expenditure (MPCE) quintiles, ranging from the poorest to the richest; and employment status (never worked, ever worked, working). Health-related behaviors, such as smoking status (yes, no, or never) and alcohol consumption history (yes, no, or never), were included in the research.
Statistical Analysis
Descriptive statistics and bivariate analysis were utilized to illustrate the sociodemographic and health characteristics of older adults. A chi-square test was employed to determine the significance level of the bivariate associations. Additionally, both linear and binary multivariate logistic regression analyses were carried out to evaluate the associations between yoga, meditation, asana, pranayama, and related practices with various health outcome variables, while adjusting for factors such as age group, sex, residence, marital status, caste, religion, education, living conditions, MPCE, employment status, smoking habits, and alcohol consumption. Linear regression models were used for continuous outcome variables (e.g., cognition, life satisfaction, sleep score, ADL/IADL score, and handgrip strength), while logistic regression models were applied to binary outcomes (e.g., presence of pain). This approach ensures appropriate estimation based on the distribution and measurement scale of the dependent variables.
Model adequacy was evaluated by using standard diagnostic procedures. For linear regression models, residual diagnostics and multicollinearity were assessed using the variance inflation factor (VIF) values. For logistic regression, model performance was evaluated using the area under the receiver operating characteristic curve (AUC), and results are reported with 95% confidence intervals to ensure robustness and interpretability of the estimates.
All regression models had consistently low VIF values (1.44–1.48), well below the conventional cutoff of 5, indicating no evidence of multicollinearity and confirming the stability of the estimated models (Supplemental Table S3). The pain prediction model demonstrated moderate discrimination (AUC = 0.6486; 95% CI: 0.6422–0.6551), suggesting performance better than chance but limited predictive strength. At the 0.50 cutoff, the model showed high specificity (85.0%) but low sensitivity (31.5%), indicating better identification of non-cases than true pain cases. Overall, the model is statistically robust but has modest classification performance, particularly in detecting cases of pain (Supplemental Table S4).
The equation of linear regression can be written as follows:

The formula used in logistic regression is:

Results
Socio-Economic and Demographic Profile of Older Adults
Table 1 shows the characteristics of the sample of 28,482 respondents, comprising 13,728 (47.4%) males and 14,754 (52.6%) females. The mean age of the participants was 68.7 years. Approximately, 71.6% of the population lived in rural areas, 62.0% were married, 82.7% were Hindu, 45.7% belonged to the OBC, more than half (56.5%) had no formal education, 41.6% shared a home with a spouse and children, 31.6% were working, 40.5% smoked, and 14.8% had a history of alcohol consumption. Only a small proportion of participants belonged to the wealthiest quintile. Participation in yoga and related practices among elderly individuals in India is notably linked to various socio-demographic and lifestyle factors. Individuals who are engaged in these practices tend to be younger, mainly male, live in cities, and typically have higher socioeconomic status and education levels, along with a reduced tendency to smoke. Furthermore, elements such as housing situations and marital status influence these practices, suggesting a potential role of social support in the adoption of health-promoting behaviours.
Weighted Sample Characteristics by Involvement in Activities Like Yoga, Meditation, Asana, Pranayama, LASI Wave 1 (n = 28,482).
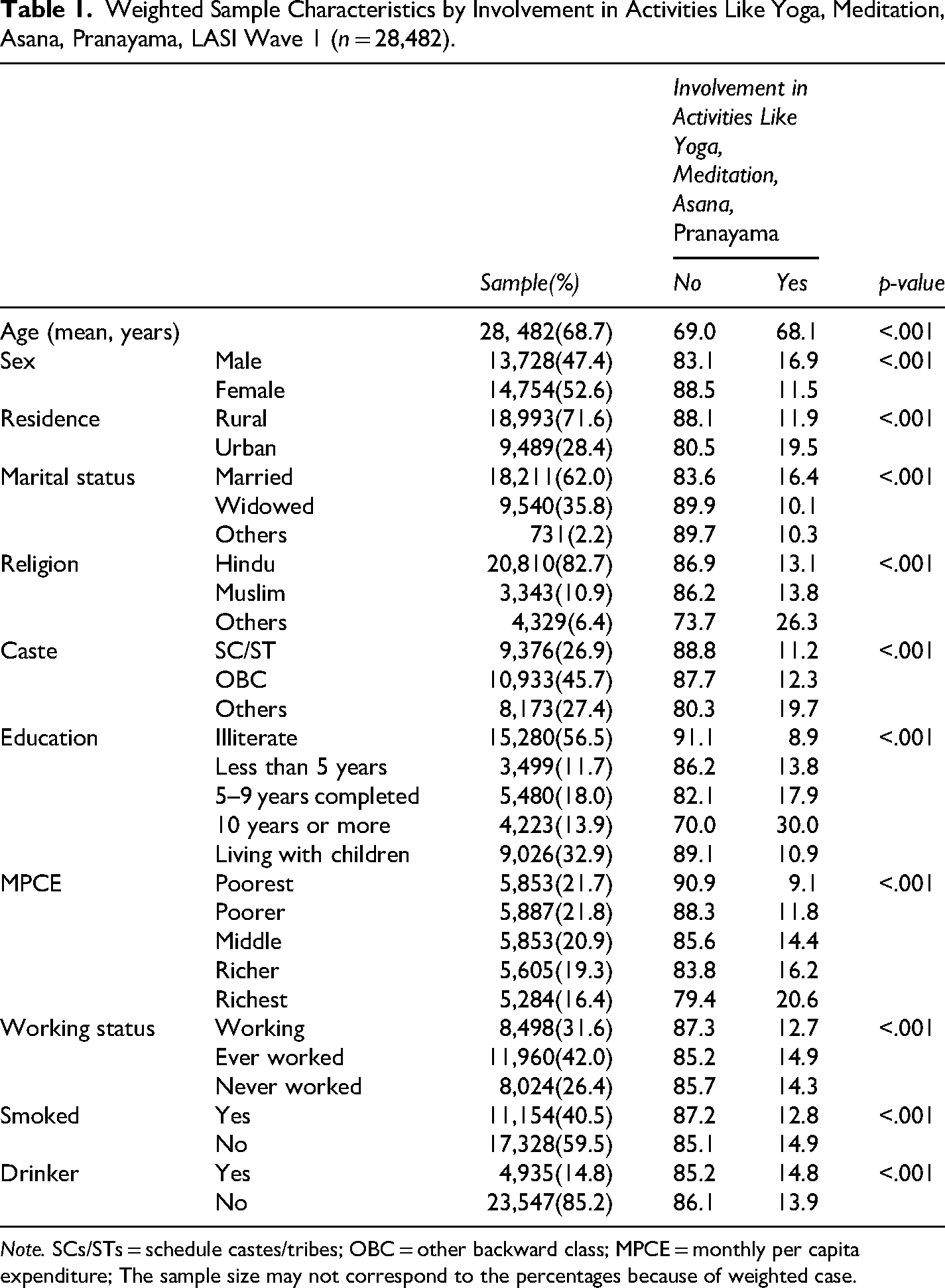
Note. SCs/STs = schedule castes/tribes; OBC = other backward class; MPCE = monthly per capita expenditure; The sample size may not correspond to the percentages because of weighted case.
Table 2 presents a comparative analysis of health indicators among older adults based on their yoga practice and frequency of practice. All indicators show statistically significant differences, with yoga practitioners performing better on nearly all measures—especially cognition, social activity, life satisfaction, and strength. The yoga group demonstrated better cognitive functioning, greater social engagement, higher life satisfaction, higher physical activity, greater muscle strength, fewer depressive symptoms, fewer functional limitations, but slightly more sleeping problems, and a higher prevalence of pain. Cognition and social activity are highest among daily practitioners. Depressive symptoms (CES-D) are lowest among daily practitioners. Handgrip strength and physical activity are also better with frequent yoga practice. Pain showed an unexpected pattern with most yoga practitioners reporting higher levels of pain; however this may reflect greater body awareness, or a reverse causality (i.e., individuals experiencing pain may adopt yoga as a coping strategy).
Yoga, Frequency of Yoga and Health Indicators Among Older Adults, LASI Wave 1, 2018–2019.
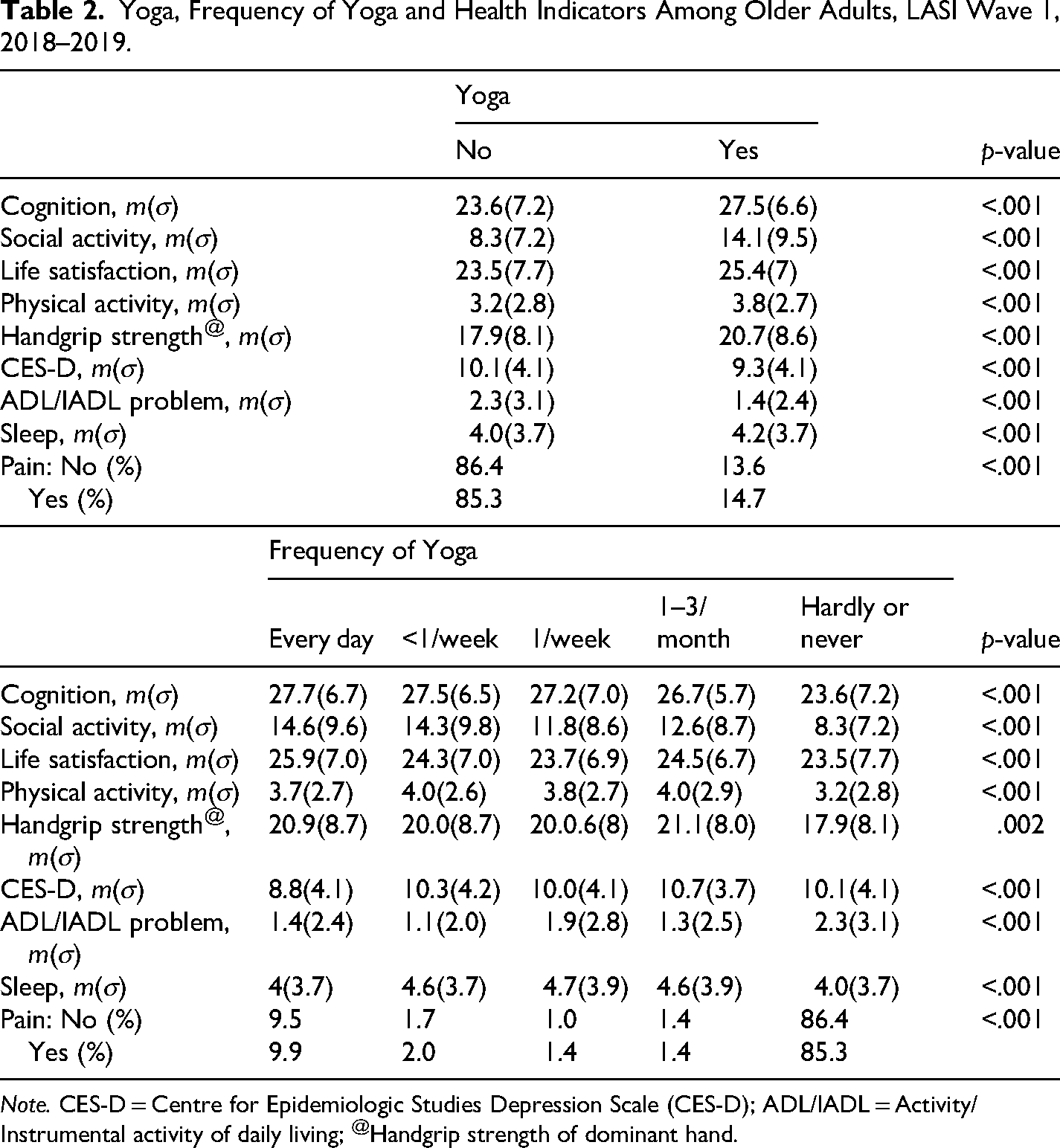
Note. CES-D = Centre for Epidemiologic Studies Depression Scale (CES-D); ADL/IADL = Activity/Instrumental activity of daily living; @Handgrip strength of dominant hand.
Supplementary Figure S1 demonstrates substantial state-level variation in the practice of yoga, meditation, asanas, and pranayama among older adults in India. Bivariate maps indicate that regions with a higher prevalence of yoga generally exhibits more favorable health outcomes, including better cognition, higher levels of physical activity, greater social interaction, improved life satisfaction, and enhanced functional capability. However, inconsistent trends were observed for pain and sleep-related outcomes. Higher prevalence of yoga practices was concentrated in relatively urbanized, socioeconomically advanced, and culturally yoga-oriented states (e.g., Delhi, Maharashtra, Karnataka, Kerala, Uttarakhand, and Himachal Pradesh), whereas lower prevalence was more common in economically disadvantaged and predominantly rural states (e.g., Bihar, Jharkhand, Chhattisgarh, and Odisha).
Yoga, Meditation, Asana, Pranayama, and Health status
Table 3 displays the regression findings that illustrate the association between yoga-related activities (such as yoga, meditation, asana, and pranayama) and various health metrics in older adults in India, based on data from LASI Wave 1 (2017–2018). The findings are presented as β coefficients (with 95% confidence intervals) from multivariate models that have been adjusted for several socio-demographic and lifestyle variables. Yoga participation was associated with improved health across nearly all domains, especially in cognition, social engagement, physical exercise, and sleep quality. No consistent association was observed for depressive symptoms (CES-D), and there is a minor increase in reported pain. The most significant improvement in CS is observed among those who practice 1 time/week (β = 1.35), although those who engage in daily and >1/week also demonstrate significant benefits. A mixed and non-linear dose–response pattern was observed. A consistently positive association between yoga practice and social engagement was observed across all frequencies, with peak impact at >1/week and daily. When it comes to life satisfaction, only daily engagement demonstrates a strong positive association, whereas other frequencies either show insignificant results or indicate negative outcomes. A robust, positive association exists across all frequencies for physical activity, with significant results for daily and practices >1/week. Improvements in grip strength are seen across all frequencies except for those practicing >1/week, with the most notable benefits reported at 1–3/month (β = 1.35). Daily practice decreases symptoms of depression (β = −0.25), whereas practicing yoga less frequently (>1/week, 1–3/month) could potentially elevate depressive symptoms (positive β). Both daily and >1/week practice significantly reduces functional problems. All frequencies of yoga practice improve sleep, though the greatest improvements are seen in those who practice 1–3/month and >1/week. There is a modest increase in pain reported at all frequencies, especially among individuals who practice weekly (β = 0.38).
Association of Involvement in Activities Like Yoga, Meditation, Asana, Pranayama and its Frequency With Health Indicators Among Older Adults in India, LASI Wave 1, 2017–2018.
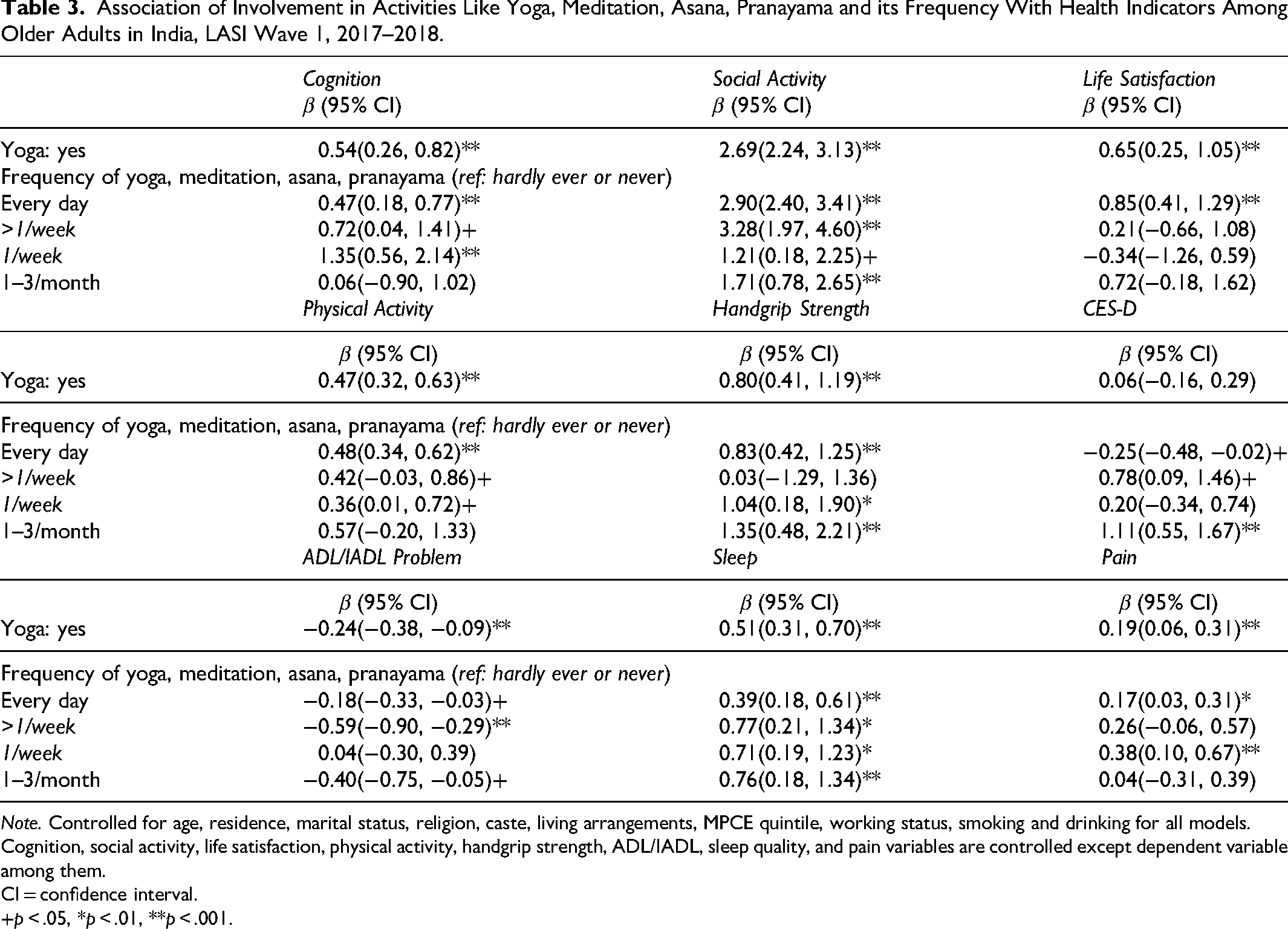
Note. Controlled for age, residence, marital status, religion, caste, living arrangements, MPCE quintile, working status, smoking and drinking for all models. Cognition, social activity, life satisfaction, physical activity, handgrip strength, ADL/IADL, sleep quality, and pain variables are controlled except dependent variable among them.
CI = confidence interval.
+p < .05, *p < .01, **p < .001.
Discussion
Using nationally representative data from older adults in India, this study examined the association between participation in yoga and related mind–body practices—and their frequency with multiple dimensions of health. The findings indicate that yoga engagement, particularly at higher frequencies, is associated with better CS, greater social participation, improved sleep quality, higher physical activity, stronger grip strength, and fewer functional limitations. However, associations with depression were mixed, and yoga practitioners reported a higher prevalence of pain.
The positive association between yoga practice and CS is consistent with previous research suggesting that mind–body interventions may help preserve cognitive health in later life (Bhattacharyya et al., 2021; Hariprasad et al., 2013; Hoy et al., 2021). However, the present study indicates a non-linear relationship between yoga frequency and cognitive outcomes, where benefits are observed across frequencies but do not increase proportionally. This pattern may reflect heterogeneity in practice type, duration, and individual health status. Potential mechanisms include improved cerebral blood flow, reduced stress, and enhanced attentional control (Gothe et al., 2014; Hariprasad et al., 2013). At the same time, residual confounding—such as education and socioeconomic status—may partly explain these associations. Future research should consider domain-specific cognitive analyses to better understand these relationships.
Consistent with prior evidence, yoga participation was positively associated with physical functioning and strength. Improvements in grip strength and physical activity suggest that yoga may contribute to maintaining mobility and independence among older adults (Ko et al., 2023; Sivaramakrishnan et al., 2019). These findings align with intervention-based studies demonstrating gains in balance, flexibility, and muscular strength, which are critical for fall prevention and functional autonomy (Bartos et al., 2022; Park & McCaffrey, 2012). Additionally, the observed associations with life satisfaction and social engagement reinforce the broader psychosocial benefits of yoga, particularly when practiced regularly (Prashanth et al., 2024; Woodyard, 2011).
The relationship between yoga and depressive symptoms was less consistent. While daily practice was associated with modest improvements, less frequent engagement showed weaker or mixed associations. This suggests that regular and sustained practice may be necessary to achieve mental health benefits, a finding supported by prior systematic reviews (Chobe et al., 2020; Cramer et al., 2017; Gour et al., 2020; Ko et al., 2023; Lee et al., 2019). Variability across studies may reflect differences in measurement approaches, intervention intensity, and population characteristics.
A notable and unexpected finding is the higher reporting of pain among yoga practitioners, which contrasts with much of the existing literature indicating pain reduction benefits in India (Deepeshwar et al., 2018; Sharma & Ghai, 2024) and globally (Cramer et al., 2013; Deepeshwar et al., 2018; Ko et al., 2023; Sharma & Ghai, 2024; Wieland et al., 2017). Several explanations may account for this discrepancy. First, reverse causality is likely, as individuals experiencing pain may adopt yoga as a therapeutic strategy. Second, increased body awareness among practitioners may lead to greater reporting of pain. Third, inappropriate or unsupervised practice may contribute to discomfort, particularly among older adults with pre-existing conditions (Ko et al., 2023). Cultural factors and reporting biases may also play a role. Importantly, the cross-sectional design limits the ability to determine the directionality of this association. Moreover, selection bias may also exist in yoga studies, as they typically involve healthier individuals, which results in an overestimation of yoga's benefits and an underrepresentation of its negative effects in the elderly population (Sivaramakrishnan et al., 2019).
The study also highlights the importance of considering the frequency and intensity of engagement in understanding the health benefits of yoga. The mixed dose–response patterns suggest that while frequent practice is generally beneficial, the relationship is complex and varies across health domains. Social and contextual factors, including access to yoga, cultural norms, and individual health conditions, may further influence these associations.
Limitations
Despite its strengths, including a large and nationally representative sample, this study has several limitations. Most importantly, the cross-sectional design precludes causal inference, and the observed associations cannot establish whether yoga leads to improved health outcomes or whether healthier individuals are more likely to engage in yoga. Additionally, yoga, meditation, pranayama, and asana were assessed as a combined measure, limiting the ability to isolate their independent effects. The reliance on self-reported data introduces potential recall and reporting biases. Furthermore, the absence of detailed information on the type, duration, and quality of yoga practice along with preexisting health problems limits a more nuanced interpretation of the findings.
Conclusion
This study shows that participation in yoga and related mind–body practices is associated with better physical, cognitive, and psychosocial health among older adults in India. Using LASI Wave 1 data, regular—particularly daily practice was associated with improved cognition, social engagement, physical activity, grip strength, sleep quality, and functional ability, with mixed but generally positive trends for mental health. The higher reporting of pain among practitioners may reflect reverse causality, greater body awareness, or unsupervised practice. Given the cross-sectional design and reliance on self-reported measures, causal interpretations are limited. Overall, yoga appears to be a culturally relevant and scalable approach to support healthy aging, though longitudinal and intervention studies are needed to confirm these associations and guide safe implementation.
Supplemental Material
sj-docx-1-ahd-10.1177_00914150261456740 - Supplemental material for Mind–Body Practice and Healthy Aging: The Role of Yoga in Physical and Mental Well-Being Among Older Adults
Supplemental material, sj-docx-1-ahd-10.1177_00914150261456740 for Mind–Body Practice and Healthy Aging: The Role of Yoga in Physical and Mental Well-Being Among Older Adults by Alok Roy and Bhaswati Das in The International Journal of Aging and Human Development
Footnotes
Ethics Approval and Consent to Participate
Not applicable, the study is based on secondary data. For this study, no patient could be identified or contacted, and no ethics approval was required by individual researchers to undertake this study. The LASI data was collected under the approved ethical consideration of the Indian Council of Medical Research (ICMR) guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.