
Abstract
Stereotype embodiment theory states that individuals who hold negative aging stereotypes may internalize them, and thus view their own aging process as negative. This study aimed to evaluate how older adult men may be influenced by their adherence to masculinity standards, such as men are expected to be strong and independent, in older adulthood. A sample of 439 heterosexual men aged 55 and older living in the southern United States was analyzed, finding that participating in masculine behaviors moderated the relationship between negative perceptions of aging and depression. Participants who reported often participating in masculine behaviors and a negative perception of aging had higher levels of depression. Participating in masculine behaviors did not moderate the relationship between depression and positive perceptions of aging. This suggests that masculinity is an important factor to consider for the well-being of older adult men, particularly when paired with a negative perception of aging.
Public Significance Statement
Little research has been done regarding factors that put older adult men at risk for depression, although theories suggest hegemonic masculinity may contribute. In an online survey of older men living in the southern U.S., those who reported often participating in masculine behaviors and hold negative attitudes toward aging had the highest reports of depression symptoms.
Introduction
The aging experience can differ depending on the beliefs or values an individual holds. Older adult men may have a unique experience of aging due to hegemonic masculinity standards that suggest men should be strong, independent, and providers (Pattyn et al., 2015; Smith et al., 2007). The research about older adult men is sparse, being limited to understanding that physical health plays a major role in how men feel and age (Hudson, 2018). Beyond health there is much to be examined, such as masculinity, as to what is a major component to well-being in older men. This study aims to explore the relationship between masculinity beliefs and attitudes toward aging, and their impact on the mental well-being of older adult men.
Ageism
Ageism is referred to as, “one of the last socially acceptable prejudices” in our society as stereotypes are becoming more negative, more common, and less often challenged (Boduroglu et al., 2006; Ng et al., 2015; Palmore, 1999; Weir, 2023). Older adults are stereotyped as grumpy, frail, a burden on others, slow, and/or forgetful (Palmore, 1999). Adults who hold ageist views build negative aging stereotypes through their lifetime, and often view their own aging in a similarly negative light (Levy, 2003, 2009; Levy et al., 2022).
Stereotype embodiment theory explains that adherence to negative stereotypes of aging leads individuals to both view their aging in a negative way and dread the transition from middle to older adulthood (Levy, 2009). Thus, these ageist beliefs and negative stereotypes of aging can influence an individual’s attitudes toward aging to be more negative, and impact how they view their own outlook of how they are growing older. This negative perspective of aging is seen to negatively impact the individual in both mental and physical health aspects (Levy, 2003, 2009; Levy et al., 2009, 2022; Low et al., 2013). Researchers have found that those who hold negative stereotypes of aging in early life have negative physical health outcomes in late life, such as increased cardiovascular events (Levy et al., 2009; Low et al., 2013; Smith et al., 2019). Negative perceptions of aging mediate the relationship between health satisfaction and quality of life, with negative attitudes toward physical change being the strongest mediator on the relationship (Low et al., 2013).
Not all older adult groups experience the same negative aging stereotypes. Stereotype content model (SCM) explains how stereotypes are a social construct built by a two-dimensional spectrum of warmth and competence (Fiske, 2018). The warmth dimension evaluates a group's characteristics of trustworthiness and friendliness, while the dimension of competence examines the characteristics of assertiveness and independence (Fiske, 2018). Stereotypes of older adults tend to fall within the dimensions of high warmth and low competence, similar to stereotypes of young children, women, and individuals with disabilities (Fiske, 2018). However, intersectionality of identities creates complexity in the experiences and impact stereotypes have on individuals (Crenshaw, 1991).
When examining the intersectionality of different identities and older age, some identities will have experienced stereotypes within the dimensions of high warmth and low competence before older adulthood, but other identities have not (Fiske, 2018). This can influence how different demographics experience ageist treatment. For example, ethnic and racial minorities may experience ageism differently than their white counterparts. One qualitative study found that older adults of color often reported feeling unsure if the source of their experienced discrimination was age or race related (Steward et al., 2023). The research participants reported feeling confident over their lifetime about when they were being discriminated against for their race, but when approaching older age, it became less clear if their race or perceived age were causing them to be treated differently (Steward et al., 2023). One participant reported an instance of being followed around a grocery store, and being unsure if they were seen as a threat due to their race or if others were concerned about their perceived abilities due to being older (Steward et al., 2023). White older adult participants did not report the same thoughts about ageist treatment, but instead reported how this was often the first time they had to endure discrimination or maltreatment (Steward et al., 2023).
Similarly, older adult women may have experienced gender stereotypes in the same dimension as older adult stereotypes (high warmth, low competence), while men have not as male stereotypes fall in the opposite dimension (low warmth, high competence; Fiske, 2018). According to the SCM, older adult men simultaneously fall into two opposing dimensions: high competence/low warmth from stereotypes associated with men, and low competence/high warmth from being older (Fiske, 2018). In the high competence/ low warmth dimension, stereotypes associated with men often are related to competence, autonomy, work status, being less warm or caring, and being dominant (Ellemers, 2018; Fiske, 2018). These stereotypes and traits are often related to higher status, and these stereotypes of men are in direct opposition to aging stereotypes. Older adult men therefore may be feeling incongruencies with their identities, such as an older adult man who used to be praised for his assertiveness and intense work ethic may now be seen by others as grumpy or rigid (Palmore, 1999).
Older Adult Men
According to theories such as the double disadvantage hypothesis, which states that those who hold more than one minority status will have worse health than those who hold fewer disadvantaged statuses due to the overlapping and increased quantity of discrimination experiences, it would be expected that older adult men would have better outcomes in later life compared to women (Denise 2014; Dowd & Bengston, 1978). It would be expected that older adult men, especially older adult White men, would have the best health outcomes; however, older adult men have the highest rates of suicide compared to any other group, and older adult men have over twice the rates of suicide compared to women (World Health Organization, 2021).
The increased risk of suicide in men appears counterintuitive to rates of depression, which suggest that women are diagnosed twice as often with depression compared to men (Martin et al., 2013). The masculine depression framework suggests that men present differently with depression compared to women, and often exhibit externalizing symptoms such as substance misuse, aggression, or lower impulse control (Addis, 2008; Cavanagh et al., 2017). This would suggest that rates of depression for men are underrepresented in research. The masculine depression framework suggests that difficultly adhering to masculinity standards places men at increased risk for experiencing externalized symptoms of depression, which as stated are the more common symptoms for men to experience (Cavanagh et al., 2017). The inconsistencies between the double disadvantage hypothesis and the masculine depression framework warrant more research into the mental health of older adult men.
Older adult men experience both internal and external pressure to fulfill their roles according to stereotypes of men (Pattyn et al., 2015). Gender roles and hegemonic masculinity standards place pressure on men to maintain independence, assertiveness, and toughness, meaning they likely feel negatively about themselves and are viewed negatively by others if they do not meet these expectations (Smith et al., 2007). However, many negative stereotypes expect older adults to be the opposite of these masculine traits (i.e., dependent and frail). The contradiction in these expectations is likely to have an impact on older adult men, but research evaluating this impact remains scarce.
The Health, Illness, Men and Masculinities (HIMM) framework highlights the incongruencies and tradeoffs related to masculinity that older adult men encounter (Evans et al., 2011). The HIMM framework overall describes how health and wellness can be influenced by masculinity (Evans et al., 2011). During midlife, men are seen exploring and solidifying their identity within masculinity by building their career, beginning a family, and identifying ways they feel productive in society (Evans et al., 2011). However, men in late life encounter a gradual decrease to all that they have built in midlife. They experience changes with their body to where they are less able to complete physical tasks as easily as they could earlier in life, they begin to retire and thus their routine likely does not include as much productivity, and through all of these changes they may perceive their status in society falling. This often results in older men experiencing a growing sense of loss and crisis to their identity as a man (Evans et al., 2011). This sense of loss is thought to be attached to their growing difficulty to embody gender roles and fulfill hegemonic masculinity standards, which again are to maintain independence, assertiveness, and toughness (Doyle, 1989; Smith et al., 2007).
It was found that older men have more negative perceptions of aging when they are affected by chronic health conditions, such as heart disease, while women have more negative perceptions when experiencing a decrease in functional abilities, such as arthritis and back pain (Kim et al., 2021). Additionally, men are consistently less likely to seek help for subjective, chronic pain, which could be due to hegemonic masculinity standards expecting men to remain a tough exterior (Jones et al., 2016). It is possible that the objectiveness of a chronic condition diagnosis highlights a decline in a person's health. The formality of diagnosis for chronic conditions may be a more negative event for men because they are unable to hide it from others and, thus, unable to protect their masculinity. This is supported considering that men have higher rates of depression and suicide compared to women when they experience physical illness (Canetto, 2017). This adds to support for the HIMM framework as a challenge to a man's masculinity (such as not feeling physically fit) can have detrimental effects on a man's well-being. Given the aging process naturally involves a physical decline, it appears that this is especially true when men reach older adulthood.
Additionally, the concept of “successful aging” is often related to how well an older individual maintains autonomy and independence, and this description may be more salient for older adult men (Anton et al., 2015). One qualitative study found that older adult men related maintaining independence in older age both to their sense of masculinity and to their perception of successful aging (Smith et al., 2007). Even when they are not blatantly discriminated against, older adult men experience negative impacts when they feel they are perceived as incompetent or feel they are not viewed as masculine (Canetto et al., 1995). This suggests that an older man who does not feel he is maintaining high independence is likely concerned he is viewed as not aging successfully, as well as not masculine (Anton et al., 2015; Smith et al., 2007). This dual impact from losing independence may have a more negative impact on older adult men compared to their female counterparts who would not perceive their femininity being jeopardized.
As men age, they are still expected to maintain hegemonic masculinity standards, as well as being viewed with the negative perceptions that follow older adults (Kornadt et al., 2013; Pattyn et al., 2015; Smith et al., 2007). This means that if an older adult man perceives a decrease in independence or a loss in his physical functioning, he may interpret that as a loss of his masculinity and a confirmation of negative aging stereotypes. Older adult men would then be assumed to be simultaneously experiencing the negative effects of internalized ageism (as outlined by the stereotype embodiment theory) and the negative effects from losing their sense of masculinity when they reach older adulthood. Again referencing the HIMM, it would be assumed this loss to their sense of masculinity would lead to increased psychological issues, such as depression. Additionally as highlighted earlier, negative perspectives in aging lead to more negative mental health outcomes, including depression (Levy, 2003, 2009). This would suggest that an older adult man who values his masculinity and views aging in a negative light has two avenues that are likely to increase his risk for depressive symptoms.
Current Study
The current study aimed to explore the relationship between attitudes toward aging and well-being in older adult southern men and inform research about factors that put older adult men at risk for depression. Specifically, we examined masculinity as a potential moderator of the associations between attitudes toward aging and depression in older men. The Masculine Behavior Scale (MBS) was used to conceptualize our variable of masculinity as it evaluates how often a person is participating in hegemonic masculine behaviors, and could then be assumed that the more they value masculinity the more often they will participate in masculine behaviors. This scale was constructed using Doyle's (1989) themes of masculinity: antifemininity, success, aggression, sexuality, and self-reliance.
It is not expected that simply having a high belief in masculinity will lead to negative mental health outcomes, but rather it is expected that having high beliefs in masculinity will add to the burden of aging for participants who also have a negative perception of aging. Therefore, it is hypothesized that participation in masculinity beliefs will be a moderator on the relationship between perceptions of aging and mental well-being. Specifically, we hypothesized that men who reported participating in masculine behaviors more often and hold negative attitudes toward aging would have poorer mental well-being in older adulthood, compared to men who reported participating in fewer masculine behaviors or have positive views of aging.
Methods
Participants and Procedures
All study procedures were approved by the university's institutional review board. Recruitment was completed using Qualtrics recruitment services through their double-opt-in market research panels and social media sources. Due to evidence that individuals living in Southern States experience accelerated aging due to health disadvantages present in the region, participants were men aged 55 and older who lived in southern states (Reynolds et al., 2025). The southern states surveyed were Alabama, Georgia, Mississippi, Louisiana, Tennessee, and Arkansas. Participants completed a 100-item survey about their demographic information and the different self-report measurements listed below. The survey protocol required responses on all items before the survey could be completed. Participants who fully completed the survey were provided with compensation in the form of gift cards or other items of value (i.e., airplane miles, gas points) that equal a value of $5 to $10.
536 participants indicated informed consent. Participants were excluded from analyses if they were under the age of 55 years old (n = 1), completed less than 50% of the survey (n = 35), or did not respond to any items on the Masculine Behaviors Scale (n = 30).
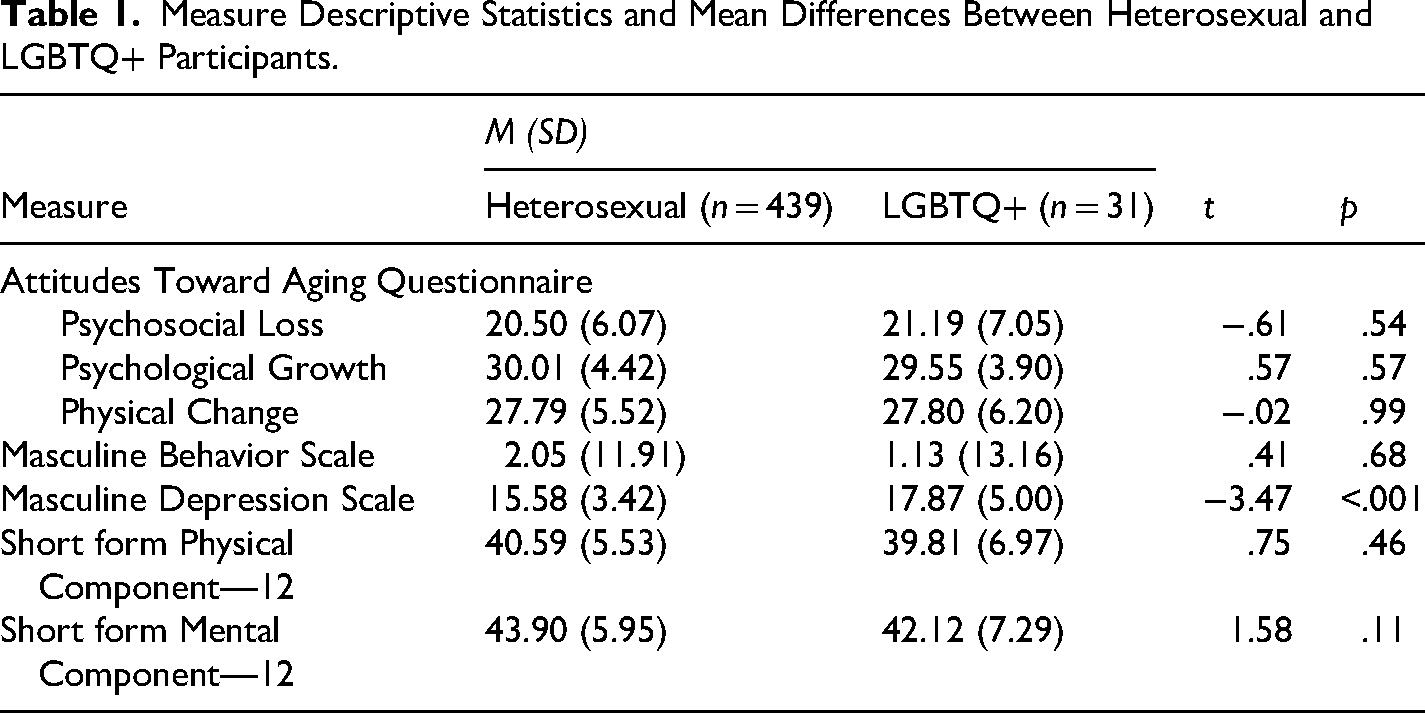
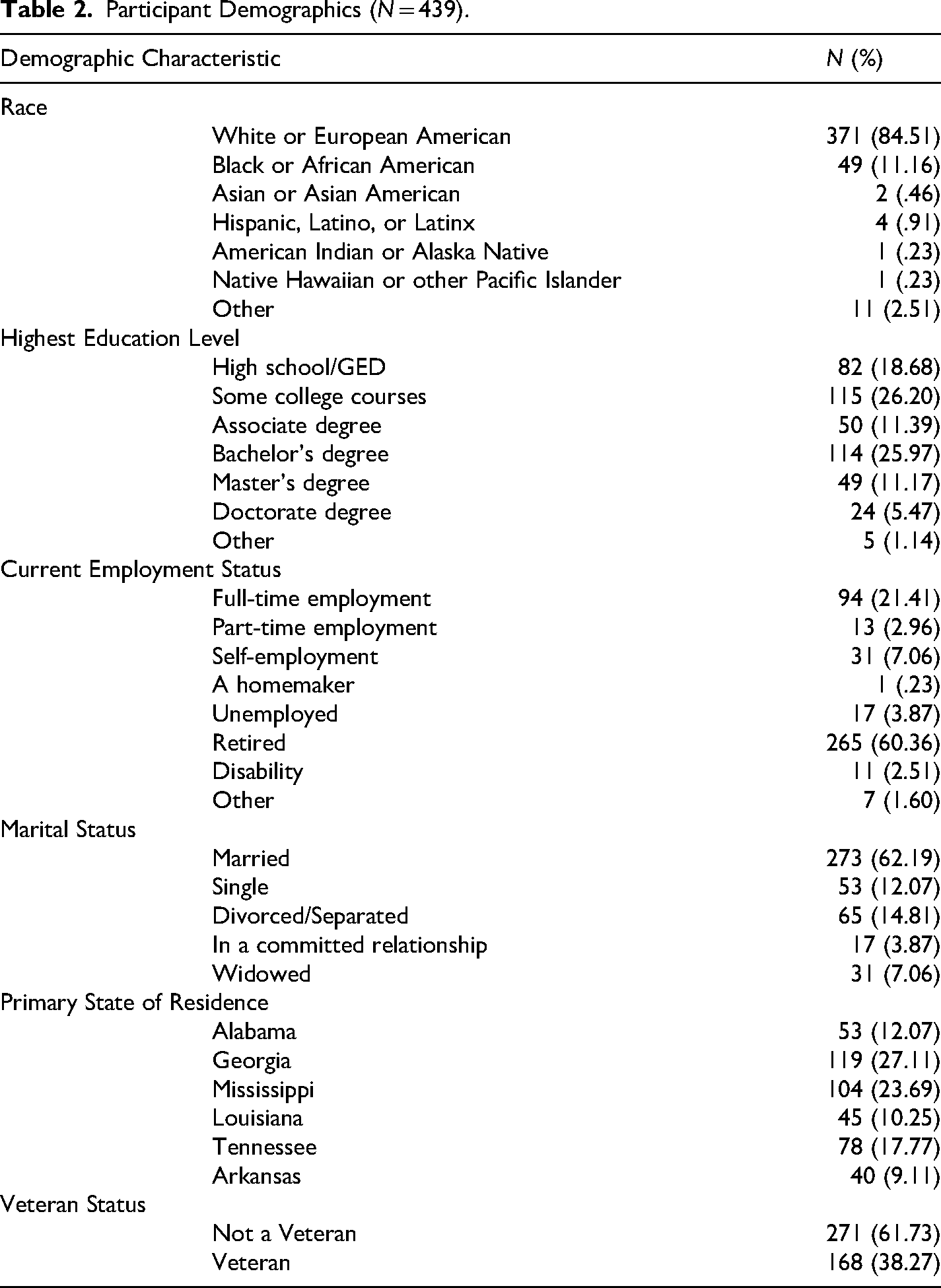
The study aimed to explore how masculine behaviors and attitudes toward aging affect older men's mental health. Although sexual orientation or gender identity may be a factor that influences one's masculinity or thoughts of aging, they are not likely the only factors. Respondents that identified as a part of the LGBTQ+ community were evaluated for similarity to other respondents using t-tests and chosen to be excluded based on these analyses. Participants who reported being part of the LGBTQ+ community (n = 31) reported higher levels of depression (M = 17.87, SD = 5.00) than the heterosexual participants, t(469) = -3.47, p = <.001. See Table 1 for measure descriptives and t-test statistics comparing groups. The final sample analyzed was 439 heterosexual men. The ages of participants ranged from 55 to 88 years old (M = 66.87; SD = 7.67). See Table 2 for participant demographics.
Measure Descriptive Statistics and Mean Differences Between Heterosexual and LGBTQ+ Participants.
Participant Demographics (N = 439).
Measures
Demographic Information
Participants were surveyed on demographic information. Questions included age, race, gender, sexual orientation, marital status, education, rurality, and veteran status.
Short Form Health Survey-12
Short Form Health Survey-12 (SF-12) was developed to assess the impact a person's health has on their life (Shah & Brown, 2020). The items ask a person's perception of both their overall health and their abilities within the last month (e.g., Does your health now limit you in the activities listed below?). The SF-12 has two factors: physical component summary (PCS-12) and mental component summary (MCS-12). A cutoff score of 50 or less on the PCS-12 factor indicates a physical health condition, and a score of 42 or less on the MCS-12 factor indicates clinical depression (Shah & Brown, 2020). The SF-12 is a condensed version of the Short Form Health Survey-36 and has been validated and shown to be reliable to be used with older adults (Shah & Brown, 2020; Ware & Sherbourne, 1992).
Masculine Depression Scale—Externalizing Factor
Masculine Depression Scale (MDS) was developed in response to research finding that individuals who subscribe to hegemonic masculinity standards do not endorse traditional depressive symptoms (Magovcevic & Addis, 2008). The MDS is a 44-item scale made up of two factors, externalizing factor (11 items) and internalizing factor (33 items). The MDS was found to have adequate reliability and construct validity in a sample of adults aged 18 to 65 (Magovcevic & Addis, 2008). The MDS was found to be highly reliable (α = .70) for the current sample.
The internalizing factor correlates best with typical depression scales that focus on internal symptoms of depression, has been seen to not correlate well with the Conformity to Masculine Norms Inventory, and is seen to not be a good representation of depressive symptoms experienced by highly masculine individuals (Price et al., 2015). The internalizing factor was not included in this study to decrease item burden on participants as the Short Form Health Survey includes a depression factor consistent with the internalizing factor. However, the externalizing factor moderately correlates with the Conformity to Masculine Norms Inventory and may be better at examining depression in men who adhere to masculine standards (Price et al., 2018).
Attitudes Toward Aging Questionnaire
The Attitudes Toward Aging Questionnaire is a 24-item scale that evaluates perceptions of successful aging in three factors: psychological growth, psychosocial loss, and physical change (Laidlaw et al., 2007). The psychosocial loss subscale (e.g., “Old age is a time of loneliness”) focuses on psychological and social losses in aging, and higher scores would assume an individual views aging as negatively. The Physical Change subscale (e.g., “It is important to exercise at any age”) relates to physical and functional changes that are currently occurring for a respondent and tends to not be associated with a negative or positive view of aging. The Psychological Growth subscale (e.g., “It is a privilege to grow old”) examines how much an individual associates aging with concepts of wisdom or growth, and higher scores tend to relate to individuals who view aging in a positive light. The items ask older adults to evaluate their own aging (e.g., I don’t feel old) and their thoughts about aging (e.g., It is a privilege to grow old; Laidlaw et al., 2007). Per Laidlaw et al., the Cronbach's alpha was calculated for each subscale as well as the full scale. The Cronbach's alpha for the full scale was found to be .56 for the current sample. The PG scale (α = .75), the PL scale (α = .86), and the PC scale (α = .83) were found to be highly reliable in the current sample.
Masculine Behavior Scale
The MBS is a 20-item scale to identify how many stereotypical masculine behaviors an individual regularly participates in. The scale has four subscales: restrictive emotionality, inhibited affection, success dedication, and exaggerated self-reliance (Snell, 1989). The MBS showed gender differences on only two subscales where men reported higher on restrictive emotionality and inhibited affection than women. This highlights how it is measuring masculinity as a spectrum compared to only gender stereotypes (Snell, 1989). The MBS was found to be highly reliable (α = .84) for the current sample.
Data Analysis
All analyses were conducted using SPSS 29.0. Data were found to be within normal limits regarding normality (i.e., skew < 3, kurtosis < 7) (Kline, 2016). Zero-order correlations were examined between all study variables. A series of multiple regression analyses were conducted to investigate whether masculinity as measured with the MBS moderated the associations between depression measured using the MDS and attitudes toward aging on the AAQ subscales (psychological growth, psychosocial loss, and physical change). An a priori power analysis using G*Power evaluating the sample size needed for a medium effect size of f2 with 3 tested predictors (two variables and the interaction term) would need a sample size of 107 individuals (Faul et al., 2007).
Results
On average, participants’ scores on the SF-PCS-12 suggested many participants have at least one physical health condition, which is consistent with the age range of the sample (≥55 year old). Participants’ average scores on the SF-MCS-12 were slightly above the cut-off for clinical depression (43.90 vs. ≤42), suggesting many participants within sample experience depression. To evaluate validity, scores on the SF-MCS-12 and the MDS were evaluated for correlation. Lower scores on the SF-MCS-12 indicate depression and higher scores on the MDS indicate depression, meaning a negative correlation suggests they are measuring depression similarly. This was found to be accurate within this sample, as SF-MCS-12 and the MDS were negatively correlated (r(486) = −.20, p < .001). See Table 3 for all correlations.
Correlations Among Variables.
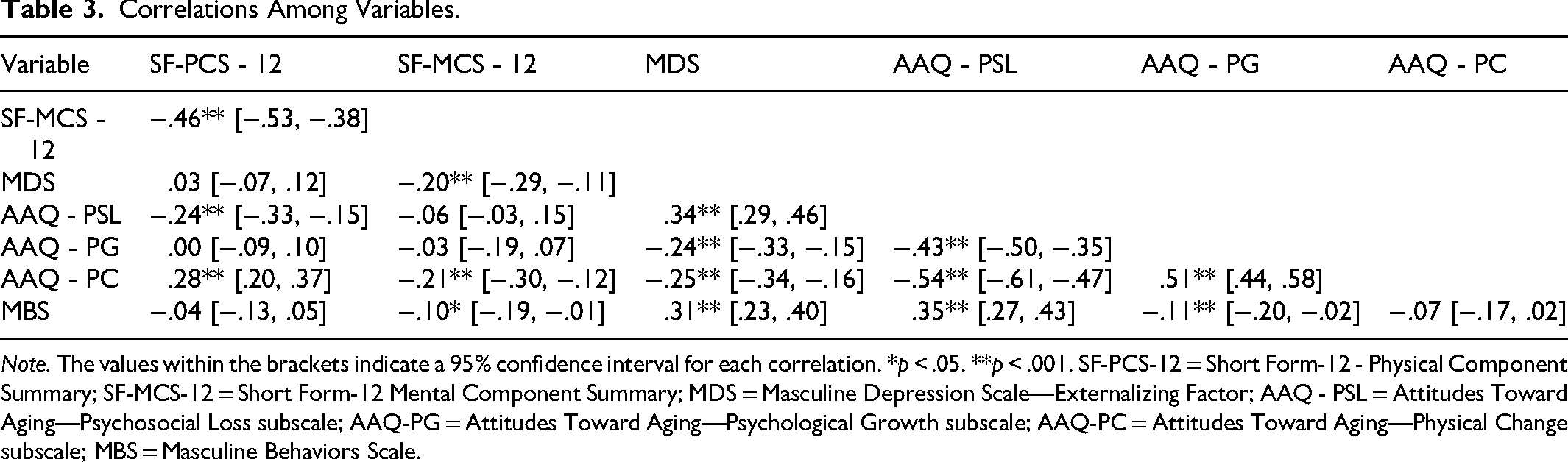
Note. The values within the brackets indicate a 95% confidence interval for each correlation. *p < .05. **p < .001. SF-PCS-12 = Short Form-12 - Physical Component Summary; SF-MCS-12 = Short Form-12 Mental Component Summary; MDS = Masculine Depression Scale—Externalizing Factor; AAQ - PSL = Attitudes Toward Aging—Psychosocial Loss subscale; AAQ-PG = Attitudes Toward Aging—Psychological Growth subscale; AAQ-PC = Attitudes Toward Aging—Physical Change subscale; MBS = Masculine Behaviors Scale.
Moderation Analyses
The interaction between AAQ-PSL and MBS was significant (β = .31, t = 2.05, p = .04), suggesting that the effect of AAQ-PSL on MDS depended on MBS scores, or the number of masculine behaviors one endorsed (see Table 4). Together, the variables accounted for approximately 19% of the variance in MDS, F(3, 435) = 33.61, p < .001. Simple slopes for the association between AAQ-PSL and MDS were tested for low (−1 SD below the mean), moderate (mean), and high (+1 SD above the mean) scores on the MBS. Each of the simple slope tests revealed a significant positive association between AAQ-PSL and MDS, but the AAQ-PSL was more strongly related to MDS for high levels of MBS (B = .21, SE = .03, β = .38, p < .001) than for moderate (B = .17, SE = .03, β = .29, p < .001) or lower scores (B = .12, SE = .04, β = .20, p = .003) on the MBS. See Figure 1 for a graph of moderation effect.
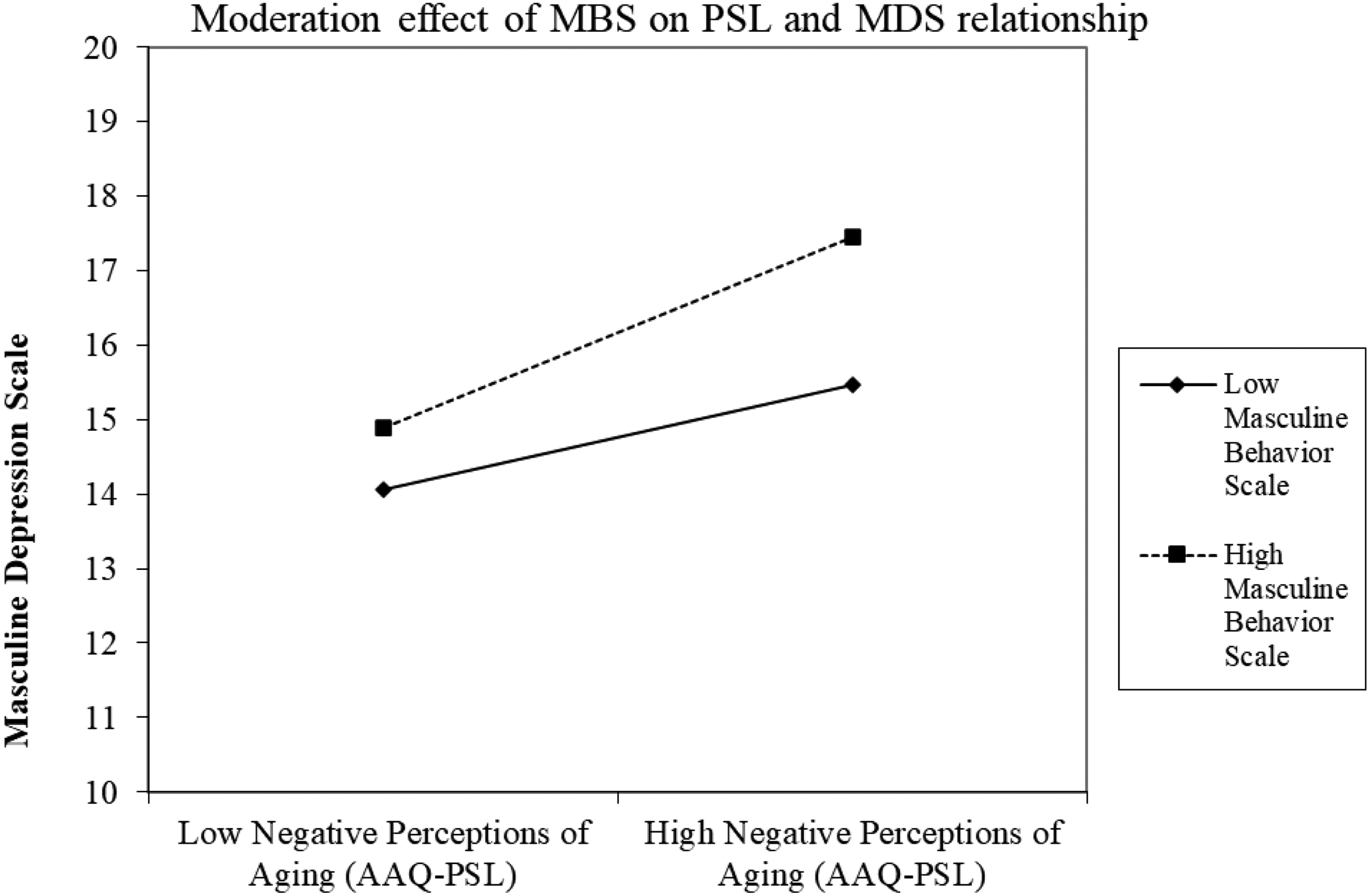
Graph of moderation effect of MBS on the relationship between AAQ-PSL and MDS. Note. Individuals with high scores on the MBS scale had higher scores of depression, whether they had low or high negative perceptions of aging. Individuals who had low scores on the MBS scale had higher scores of depression when they had more negative views of aging.
Regression Analyses Evaluating the Interaction of Attitudes Toward Aging and Masculine Behaviors Scale as a Predictor of Masculine Depression Scale.
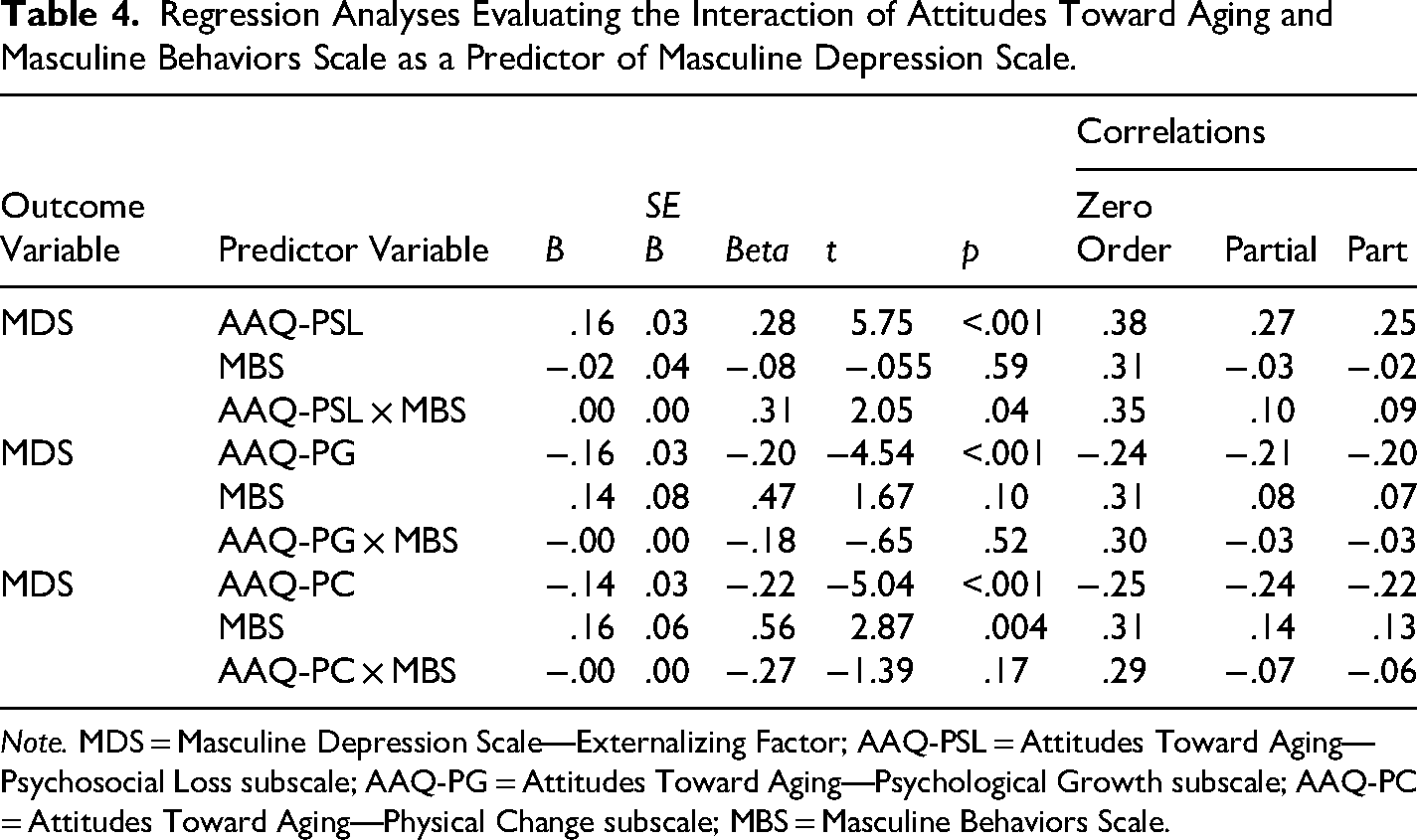
Note. MDS = Masculine Depression Scale—Externalizing Factor; AAQ-PSL = Attitudes Toward Aging—Psychosocial Loss subscale; AAQ-PG = Attitudes Toward Aging—Psychological Growth subscale; AAQ-PC = Attitudes Toward Aging—Physical Change subscale; MBS = Masculine Behaviors Scale.
The interaction between AAQ-PG and MBS was not significant (β = −.18, t = −.65, p = .52), suggesting that the effect of AAQ-PG on MDS was not dependent on MBS scores. Together, the variables accounted for approximately 14% of the variance in MDS, F(3, 435) = 24.17, p < .001. The interaction between AAQ-PC and MBS was also not significant (β = −.27, t = -1.39, p = .17), suggesting that the effect of AAQ-PC on MDS was not dependent on MBS scores. Together, the variables accounted for approximately 16% of the variance in MDS, F(3, 435) = 26.78, p < .001. When controlling for AAQ-PC and the interaction term for AAQ-PC and MBS, the partial correlation (r = .14, p = .004) suggests a small effect size for the relationship between MBS and MDS. Additionally, the part correlation (r = .13, p = .004) can be squared to evaluate the amount of specific variance MBS has in the regression to account for change in the MDS. In this case, the MBS accounts for 1.7% of the unique variance in MDS (see Table 4).
Discussion
This study aimed to evaluate the relationship between internalized aging, masculinity behaviors, and depression in older adult men to inform research about factors that put older adult men at risk for suicide. The HIMM framework suggests that perception of masculinity may play a major role in the health and wellness of older adult men (Evans et al., 2011). As older adult men age, they experience challenges to their ability to fit hegemonic masculine expectations, and these deficits in masculine identity are associated with poorer health outcomes (Evans et al., 2011). This highlights that for older men the specific relationship and intersectionality between identities may play a large role in the experience of aging stereotypes for men. For older adult men, their gender allowed them specific respect and status that their female counterparts were not granted. However, in older adulthood they may be experiencing a shift in how individuals treat them. For example, young and middle adult men are often seen as strong and independent, both of which are also traits of masculinity. However, older adults are seen as weak and in need of assistance, and inherently not masculine. This may mean that older adult men are going to experience a significant shift in how others view and treat them, and likely a shift in their sense of masculinity. As the HIMM framework explains, this would be expected to affect their health and well-being as they age.
Stereotype content theory explains that aging stereotypes tend to fall into the dimensions of high warmth and low competence, opposite to stereotypes of men (Fiske, 2018). Older adult men may not be as well equipped to cope with negative stereotypes than women or people of color, and may be experiencing a greater shift to their social identity. Men are often viewed as strong and with respect, while older adults are viewed as weak and as a burden. This shift in perception is likely going to challenge their sense of masculinity, which would be expected to lead to negative mental health outcomes.
The results supported our primary hypothesis, showing that participating in masculine behaviors moderated the relationship between holding negative attitudes toward aging and depression symptoms. The results suggest that those who participate in more masculine behaviors and have negative perceptions of aging have the highest reports of depression symptoms. This moderation was not present for measures of positive or neutral attitudes of aging, highlighting the impact that negative perceptions of aging in tandem with adherence to masculine beliefs can lead to negative outcomes.
It was expected that those who held negative attitudes toward aging and highly valued masculinity would have higher ratings of depression. This hypothesis was supported by the results, showing that scores on the MBS moderated the relationship between the AAQ- PSL and depression. These findings are congruent with the HIMM framework that masculinity plays a role in the well-being of older adult men (Evans et al., 2011). It appears that the relationship between negative perceptions of aging and depressive symptoms depended on how often men participated in masculine behaviors. It can be argued that those who participate more often in masculine behaviors value upholding masculinity standards more than those who choose to not adhere to masculine behaviors as often. Stereotype content theory would suggest that as men age, they will experience a shift from others perceiving them in the low warmth, high competence dimensions of stereotypes to the opposite dimensions of high warmth, low competence (Fiske, 2018). For an older adult man, this shift would look like others seeing him through a lens of jealousy and envy for the majority of his life, and then with pity and sympathy as he ages (Fiske, 2018).
The second hypothesis expected that masculine behaviors would not moderate the relationship between positive perceptions of aging and depression. The hypothesis was supported, showing that the MBS did not moderate the relationship between AAQ-PG and MDS for older adult men. Additionally, the third hypothesis expected that the MBS would moderate the relationship between AAQ-PC and the MDS for older adult men; however, it was not supported by the results. The AAQ-PC is not related to a positive or negative view of aging but rather the current experience of respondents, which may explain why masculinity did not moderate the relationship. Overall, the results suggest that masculinity is not likely an important predictor to the well-being of older adult men, except when paired with a negative view of the aging process.
These results suggest that for older adult men, their perceptions of aging and their beliefs in masculinity in tandem impact their mental health. Hegemonic masculinity standards place pressure on men to maintain their independence, assertiveness, and strength, even into older age (Smith et al., 2007). Older adult men who view themselves as an older person or is stereotyped as older may feel they are not fulfilling their masculine expectations. Individuals who have positive perceptions of aging are expected to have better outcomes in older age than those who have negative perceptions (Levy, 2009; Levy et al., 2022). This relationship is seen to be consistent with the result of this study, where older adult men who view older adulthood to be connected to psychological growth reported less depression, whether they had strong beliefs about masculinity or not. To be treated as an older adult would mean that an older adult man is not fulfilling his masculine role. He may experience a shift in how he is treated or being perceived by others, such as receiving more offers for help with tasks and thus feeling pitied rather than respected. This shift in treatment or perception would be seen as detrimental to a man's overall well-being according to the HIMM framework, but especially so if he places a high value on masculinity. However, the results of this study suggest that men who also hold a positive view of aging, such as viewing a need for assistance as an accepted part of aging, may not view these aging changes as a challenge to their masculinity. This would suggest positive view of aging could be a protective factor for older adult men experiencing a challenge to their masculinity.
The findings of this study further support theories about the influence of masculinity standards on the mental health of men. Robbins et al. (2016) discuss the theory of Gender Role Strain in older adults, and highlight how psychological distress often arises in men who feel they do not fulfill their male role. For older adult men, they may view aging in a negative way due to standard aging stereotypes, but additionally view the time as negative due to how aging is portrayed to be opposite of major tenets of masculinity (Doyle, 1989; Robbins et al., 2016). It was also highlighted how within the theory of Gender Role Strain, there is a level of gender role trauma related to how boys are socialized in extreme ways to uphold masculinity standards (Robbins et al., 2016). For years, men are criticized by their peers or shamed by society for not upholding masculinity standards. However, when they reach older adulthood, the expectation is now that they release these expectations of masculinity and accept being viewed as an older adult (i.e., weak, pitied, powerless; Palmore, 1999). It appears that the findings of this study may extend to support other theories of masculinity, and the impact adherence to these standards can have on older men.
Clinical Implications
The results suggest that older adult men who have negative attitudes toward aging and who adhere to traditional behaviors of masculinity experience more depressive symptoms in older adulthood. Researchers should continue to investigate this relationship to better understand the mechanisms and factors that contribute to these findings. Mental healthcare providers may benefit from recognizing the relationship between masculinity and negative perceptions of aging, and discussing thoughts or experiences related to aging with their clients who identify as men. Individuals who have a rigid adherence to hegemonic masculinity standards and who perceive aging negatively may benefit from discussing these views, and how to acknowledge the positive aspects of growing older.
As the results showed, there does not appear to be a consistent relationship between masculinity and depression. This indicates that adherence to masculinity standards does not lead to depressive symptoms, but that participating in masculine behaviors may be one of many factors that impact the well-being of older adult men. This suggests that mental healthcare providers may discuss masculinity in therapy as a component of what contributes to one's attitudes towards aging.
Constraints on Generality
This study evaluated how beliefs about masculinity moderate the relationship between negative perceptions of aging and depressive symptoms. This study was done using a sample of men 55 years old and older who reside in southern states of the United States. These findings may not generalize to all other geographic regions of the United States as masculinity standards may differ. These results also may not generalize to people of color as this sample was primarily White individuals. Additionally, this study only included heterosexual individuals, and thus these findings may not generalize to the LGBTQ+ community's experience of aging and beliefs related to masculinity. The study utilized a survey distribution service, and all participants completed the survey online. Individuals who do not have access to the internet therefore were not able to be recruited, which may limit the generalizability of the results to all older adults.
Future Directions
Future researchers should continue to evaluate the relationship between beliefs about masculinity and negative perceptions of aging, and how these factors impact well-being in older adults. Specifically, beliefs about masculinity should be investigated to establish what beliefs specifically are contributing the most to the relationship with negative perceptions of aging. Additionally, future research may evaluate how masculinity beliefs influence the well-being of older adults during specific timeframes of aging, such as retirement, changes in ADLs, or changes in ability to live independently. Future research also should evaluate this relationship for other aspects of mental health, such as suicide risk, for older adult men. In particular, longitudinal designs would be able to employ mediation models to examine potential causal relationships between beliefs about masculinity, mental health, and perceptions of aging.
Additionally, further research should be done to establish if this relationship is consistent in other regions of the United States, given this study was only done in southern states of the United States. Additionally, other demographic groups should be evaluated to establish if this pattern is consistent, especially regarding the LGBTQ+ community. The LGBTQ+ individuals in this study tended to score higher on the MDS and were therefore excluded from results. Older adult men in the LGBTQ+ community may have different experiences of aging or beliefs about masculinity or may be at a higher risk for depression due to other sociocultural factors.
Conclusion
This study helps fill the gap in research about older adult men's mental health, exploring participating in masculine behaviors and attitudes toward aging as factors. This study found that older adult men who often participate in masculine behaviors and had negative attitudes towards aging had higher rates of depression.
Footnotes
Ethical Considerations
The research study was approved by the Mississippi State University IRB (protocol number IRB-23-408).
Consent to Participate
Participants completed written informed consent prior to completing the survey. They were aware of the survey's intentions and of compensation they would receive for their participation.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The funding for the study was a miniature grant provided by the Mississippi State University Extension Service through one of the authors.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.