
Abstract
Purpose in life (PIL) is a core dimension of eudaimonic well-being, yet the developmental factors that shape purpose in later life remain understudied. Guided by Stereotype Embodiment Theory, this study examined whether two indicators of subjective aging were associated with PIL after accounting for covariates. Data came from 150 racially and ethnically diverse community-dwelling U.S. adults aged 65+. PIL was assessed with a Ryff-based scale; subjective aging with a single-item felt age measure and the Attitudes Toward Own Aging (ATOA) scale. Hierarchical ordinary least squares regressions adjusted for education, financial strain, religiosity, self-rated health, and depressive symptoms. Both felt age and ATOA were independently associated with PIL, and the final model explained 50% of the variance (R2 = .50, p < .001). Higher education, greater religiosity, and fewer depressive symptoms were also associated with greater PIL. Findings highlight subjective aging indicators as meaningful psychological correlates of purpose and well-being in later life.
Introduction
Purpose in life (PIL) is a core dimension of eudaimonic well-being, reflecting an individual's sense of direction, meaningful goals, and the belief that their existence holds significance (Ryff & Keyes, 1995). A stronger sense of purpose has been consistently linked to positive health behaviors, greater psychological resilience, more positive relationships, higher life satisfaction, and lower levels of depression, anxiety, loneliness, and stress, as well as reduced risks of chronic illness, cognitive decline, dementia, and all-cause mortality in later life (Alimujiang et al., 2019; Irving et al., 2017; Kim et al., 2019a, 2020; Pinquart, 2002; Sutin et al., 2022). Despite extensive evidence documenting the benefits of purpose, less is known about the developmental and psychological factors that help older adults maintain or strengthen PIL. One factor requiring further exploration is the role of subjective aging and aging-related stereotypes (Joshanloo, 2024; Rasset et al., 2024).
Subjective aging refers to how individuals perceive, interpret, and internalize their own age and aging process (Diehl et al., 2014). Research has shown that subjective aging predicts physical health, health behaviors, cognitive performance, mental well-being, and longevity (Alonso Debreczeni & Bailey, 2021; Diehl et al., 2021; Tully-Wilson et al., 2021; Westerhof et al., 2023). Emerging evidence also suggests that subjective aging may shape one's sense of purpose (Hedberg et al., 2010; Joshanloo, 2024; Pinquart, 2002).
The Stereotype Embodiment Theory (Levy, 2009) offers a developmental explanation for this link. According to the theory, age-related stereotypes—internalized across the life span—become self-relevant in midlife and influence behavior, motivation, and well-being in later adulthood (Kornadt & Rothermund, 2012). Individuals with more positive views of aging tend to maintain meaningful engagement and pursue valued goals, whereas negative perceptions reduce motivation, future orientation, and engagement in purposeful activity (Kim et al., 2019a, 2019b; Levy, 2009).
Negative perceptions of aging can erode one's sense of purpose through psychological, behavioral, and physiological pathways. Psychologically, they are associated with heightened stress, diminished self-worth, and reduced motivation (Kim et al., 2019b; Rasset et al., 2024), all of which can weaken purpose. Behaviorally, they are associated with fewer goal-directed activities, less proactive coping, and fewer self-regulation strategies (Boehmer, 2007; Levy, 2009; Wurm et al., 2013), thereby limiting opportunities to cultivate and sustain purpose. Physiologically, negative aging perceptions are linked to increased inflammation and cardiovascular stress, which can deplete energy, impair cognitive function, and reduce engagement in purposeful activities (Levy et al., 2000; Stephan et al., 2015). In contrast, positive perceptions of own aging foster self-acceptance, resilience, and active engagement in meaningful pursuits—factors conducive to sustaining PIL (Joshanloo, 2024; Ryff & Keyes, 1995). Individuals with a more positive view of aging report not only a stronger sense of purpose but also greater overall life satisfaction (Hedberg et al., 2010; Joshanloo, 2024). These findings underscore the critical role of subjective aging in shaping both PIL and broader indicators of well-being.
Given the substantial benefits of PIL and the growing evidence linking subjective aging to psychological and behavioral consequences, understanding how subjective aging contributes to purpose can inform interventions and policies to enhance well-being in later life. Promoting positive aging perceptions and challenging negative aging stereotypes may strengthen purpose and improve psychological functioning. Nevertheless, empirical work linking subjective aging to PIL remains limited (Joshanloo, 2024; Kim et al., 2019b).
Although few in number, existing studies consistently point to meaningful associations. Hedberg et al. (2010) found that attitude toward own aging were associated with PIL among adults aged 85+, even after adjusting for other correlates. Two longitudinal analyses using the Health and Retirement Study (HRS) extended this work: Kim et al. (2019a) showed that perceived ageism diminished self-perceptions of aging (SPA) and subsequently reduced PIL, ultimately leading to greater depressive symptoms. Joshanloo (2024) demonstrated that increases in positive aging perceptions predicted later growth in PIL, which, in turn, was associated with greater life satisfaction. Together, these findings highlight subjective aging as a potentially important correlate of purpose and broader well-being in older adulthood.
Two widely studied indicators of subjective aging are felt age (also called subjective age or age identity) and self-perceptions of aging (SPA) (Westerhof et al., 2014). Felt age reflects how old individuals feel relative to their chronological age, whereas SPA captures broader personal beliefs and attitudes toward the aging process (Diehl et al., 2014). Felt age serves as a robust global indicator but offers limited insight into specific beliefs or experiences. In contrast, SPA is a multi-item measure including both positive and negative aging beliefs, reflections, and behaviors, offering richer information about individual aging experiences (Diehl et al., 2021).
Responding to recent calls to incorporate multiple subjective aging measures within the same study to better understand their interplay and relative predictive value (Sabatini et al., 2025; Westerhof et al., 2023), the present study examines both felt age and SPA as correlates of PIL using a racially, ethnically, and geographically diverse sample. This dual-measure approach allows for a more nuanced assessment of subjective aging and its relationship to purpose. To isolate the unique contribution of subjective aging beyond established correlates, analyses adjust for sociodemographic, psychological, and health-related factors. By integrating two complementary indicators of subjective aging, this study addresses a key gap in the literature and clarifies the independent and combined contributions of subjective aging to PIL among older adults.
Methods
Study Design and Recruitment
Data were collected in Fall 2019 as part of a cross-institutional research project examining social relationships, health, and psychosocial well-being among community-dwelling older adults. Recruitment occurred through community outreach at two geographically diverse U.S. locations—one on the West Coast and one on the East Coast—to enhance demographic heterogeneity and minimize site-specific sampling bias. Institutional Review Board approval was obtained from both participating institutions prior to data collection.
Participants were recruited through community contacts, local organizations, religious groups, and interpersonal networks. Eligibility criteria required individuals to be at least 65 years old and reside in the community rather than in institutional care settings. Data were collected using structured questionnaires that included both closed- and open-ended items. Validated instruments were incorporated to assess constructs such as SPA and PIL. Participants either completed questionnaires independently and returned in person, via postage-paid envelopes, or completed them with assistance during interviewer-administered sessions. Informed consent was obtained through the return of a completed survey or verbally for participants who engaged in interviewer-assisted administration. To facilitate data verification, the final survey item asked whether any assistance had been provided and invited participants to provide contact information should clarification be required.
Data Management and Quality Control
A multi-stage protocol was used to ensure data integrity. All surveys underwent review to identify missing responses, internal inconsistencies, and unclear markings. When necessary, participants were contacted directly to clarify responses when feasible. Survey data were entered into Qualtrics under the supervision of the first author, who oversaw all data cleaning procedures. Validation of entered data against original paper forms was conducted, and entries were checked for implausible values, outliers, and transcription errors. Missing data were examined and, when possible, resolved. In rare instances where missing responses could not be clarified, scale items were imputed using person-mean substitution, and categorical variables were imputed using the modal response. This multi-step process ensured the accuracy and completeness of the dataset.
Sample Characteristics
A total of 168 responses were collected. Eleven respondents were excluded for being younger than 65, failing to report age, residing in assisted living, or missing an entire key instrument. One additional respondent was excluded as an extreme age outlier (age 96). The final analytic sample consisted of 150 community-dwelling older adults (mean age = 70.37, SD = 5.39; range = 65–87).
The sample was 64.00% female and 60.00% partnered. Racial and ethnic diversity was substantial: 39.30% identified as White, 32.00% as Hispanic, 20.70% as Black, and 8.00% as Asian. Educational attainment ranged from less than high school (18.00%) to a bachelor's degree or higher (32.00%). Participants were geographically distributed across U.S. regions, with 54.00% residing on the West Coast and 46.00% on the East Coast. Nearly one-third (30.7%) were born outside of the United States, reflecting considerable diversity in backgrounds and life experiences.
Measures
Purpose in Life
PIL, the outcome variable, was assessed using a seven-item scale adopted from the HRS. This scale includes five items from Ryff's Measures of Psychological Well-being and two additional items reflecting Personal Growth and Self-Acceptance (Kim et al., 2019a; 2019b). Each item was rated on a 6-point Likert scale ranging from 1 (strongly disagree) to 6 (strongly agree). Sample items included “I enjoy making plans for the future and working to make them a reality” and “I have a sense of direction and purpose in my life.” Four negatively worded items (e.g., “My daily activities often seem trivial and unimportant to me”) were reverse coded. Responses were averaged across all seven items to create an overall PIL index, with higher scores indicating a stronger sense of purpose (α = .80).
Subjective Aging
The key predictors were felt age and SPA. Felt age was assessed with the questions: “Many people feel older or younger than they actually are. What age do you feel?” Participants were categorized into one of three groups based on their response: younger felt age (felt age at least one year younger than chronological age), same felt age (felt age equal to chronological age), or older felt age (felt age at least one year older).
SPA were assessed using an eight-item scale also adopted from the HRS. This scale comprises five items from the Attitudes Toward Own Aging subscale of the Philadelphia Geriatric Center Morale Scale and three items from the Berlin Aging Study (Smith et al., 2017). Participants rated each item on a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree). Sample items included “Things keep getting worse as I get older” and “So far, I am satisfied with the way that I am aging.” Four negatively worded items were reverse coded. Responses were averaged across all eight items to create the final SPA scale, with higher scores reflecting more positive perceptions of aging (α = .80).
Covariates
Covariates included religiosity, self-rated health, and depressive symptoms. Religiosity was measured using a four-item scale adapted from the Brief Multidimensional Measure of Religiousness/Spirituality (Fetzer Institute, 2003). Items assessed individuals’ commitment to their religious beliefs (e.g., “I try hard to carry my religious beliefs over into all my other dealings in life”) on a 6-point Likert scale (1 = strongly disagree to 6 = strongly agree). Higher mean scores indicated greater religiosity (α = .92).
Self-rated health was assessed with the item: “Would you say your health is excellent, very good, good, fair, or poor?” Responses were dichotomized, with 0 indicating excellent, very good, or good health and 1 indicating fair or poor health.
Depressive symptoms were assessed using the five-item version of the Geriatric Depression Scale (GDS-5; Nguyen et al., 2006). Respondents answered “yes” or “no” to five questions regarding how they have felt over the past week (e.g, “Are you basically satisfied with your life?” and “Do you often get bored?”). Scores ranged from 0 to 5, with higher scores indicating more severe depressive symptoms (α = .60).
Sociodemographic Factors
Sociodemographic factors were self-reported and included age (years), sex (0 = male, 1 = female), race/ethnicity (1 = White, 2 = Black, 3 = Hispanic, 4 = Asian or American Indian), partnership status (0 = no partner, 1 = with a partner), educational attainment, and financial strain. Educational attainment was assessed with, “What is the highest degree or certification you have earned?” Financial strain was measured with, “How difficult is it for you to meet monthly payments on your bills?” Both variables were treated as categorical in regression analyses.
Data Analysis
Descriptive statistics were computed first, followed by an examination of inter-correlations among study variables. Bivariate analyses were conducted to explore relationships between key constructs. To assess the association between subjective aging and PIL, four hierarchical ordinary least squares (OLS) regression models were estimated. Model 1 examined the unadjusted relationship between felt age and PIL, while Model 2 assessed the unadjusted relationship between SPA and PIL. Model 3 included both felt age and SPA to assess their independent associations. Model 4 adjusted for sociodemographic, religiosity, and health-related covariates; all theoretically relevant covariates were retained in the final model.
All analyses were conducted using Stata/SE 18.0. Sensitivity analyses using generalized linear models (GLM) were also performed, and results were consistent across model specifications, yielding similar patterns of coefficients and statistical significance (available upon request). For clarity and interpretability, the primary results are presented based on the OLS regression analyses. A post-hoc power analysis conducted in GPower 3.1 (Faul et al., 2007) indicated that the study achieved a power of 0.994 to detect the observed R2 increment from Model 3 to Model 4 (f2 = 0.20, α = .05, N = 150).
Results
Descriptive statistics are reported in Table 1. The mean PIL score was 4.81 (SD = 1.05), suggesting generally high purpose. Most participants (75.33%) reported feeling younger than their chronological age, while 15.33% felt the same age and 9.33% felt older. The mean score on the SPA scale was 4.23 (SD = 1.10), reflecting moderately positive aging self-perceptions. Educational attainment ranged widely, with 48.67% having a high school diploma or less and 14.67% holding a master's degree or higher. Financial strain also varied: 46.00% reported no difficulty paying bills, whereas 23.33% reported frequent hardship. The mean religiosity score was 4.63 (SD = 1.84). One quarter (24.00%) reported fair or poor health. Depressive symptoms averaged 1.03 (SD = 1.16) on a 0–5 scale, indicating low overall symptom severity.
Descriptive statistics of study variables (N = 150).
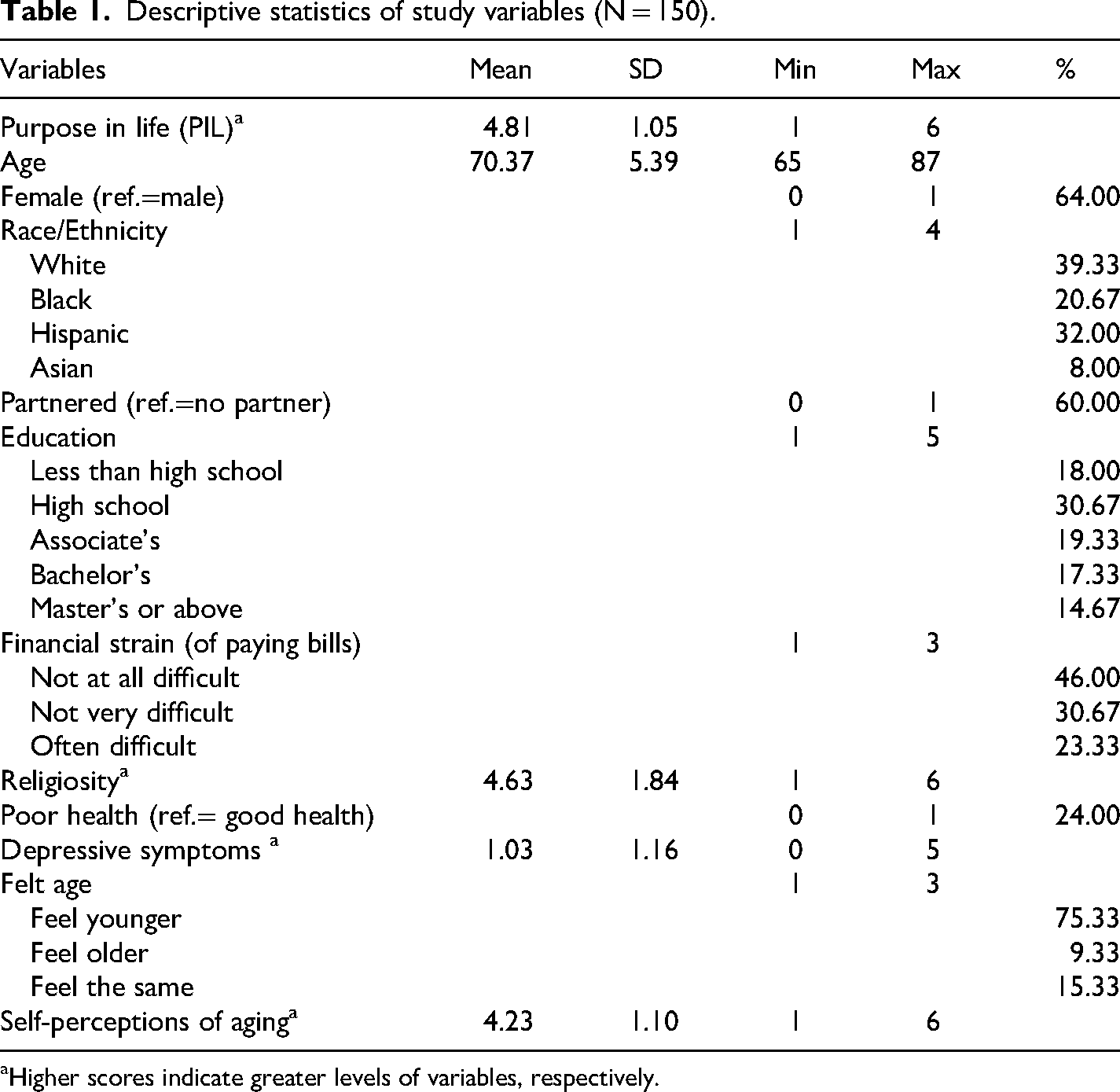
Higher scores indicate greater levels of variables, respectively.
Bivariate correlations among study variables are presented in Table 2. PIL was positively associated with educational attainment (r = .27, p < .001), religiosity (r = .20, p < .05), and SPA (r = .57, p < .001), and negatively correlated with financial strain (r = −.16, p < .05), poor health (r = −.27, p < .01), depressive symptoms (r = −.41, p < .001), and feeling older relative to one's chronological age (r = −.29, p < .001). Felt age and SPA were weakly correlated (r = −.19, p < .05), suggesting related but distinct components of subjective aging. Demographic variables (age, gender, race/ethnicity, and partner status) were not significantly correlated with PIL and were therefore excluded from Model 4.
Bivariate correlations between study variables (N = 150).
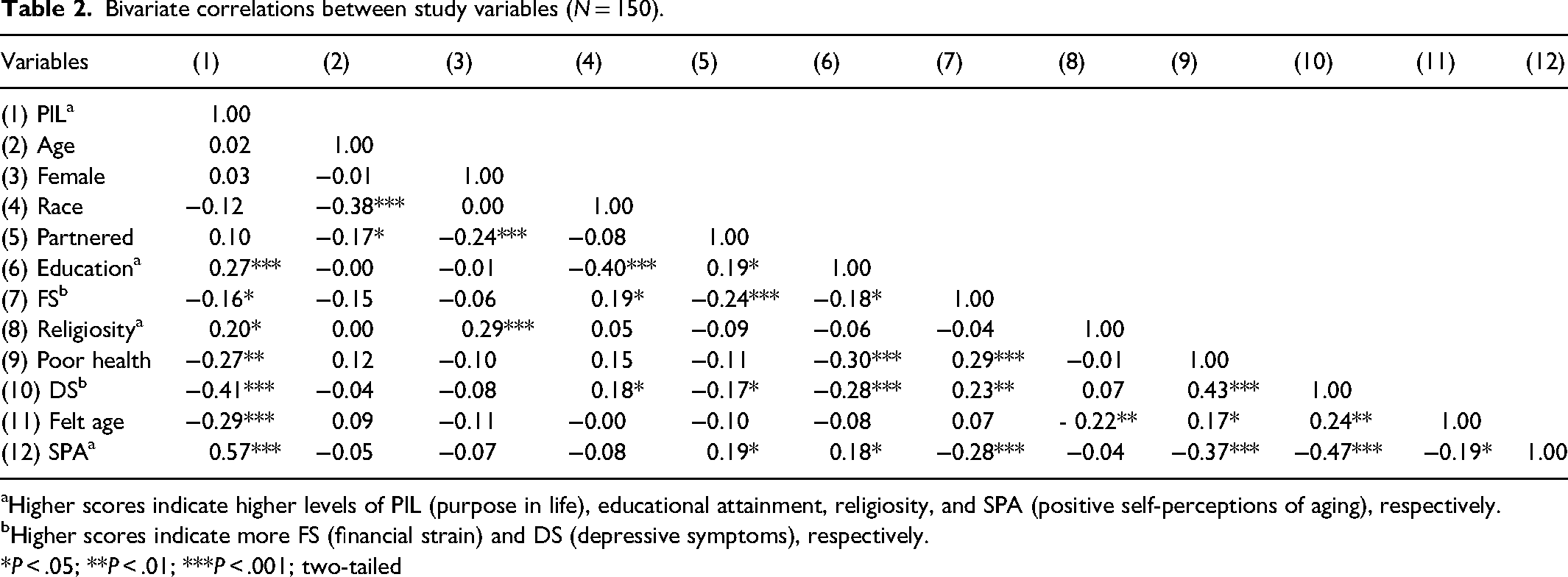
Higher scores indicate higher levels of PIL (purpose in life), educational attainment, religiosity, and SPA (positive self-perceptions of aging), respectively.
Higher scores indicate more FS (financial strain) and DS (depressive symptoms), respectively.
*P < .05; **P < .01; ***P < .001; two-tailed
Variance inflation factor (VIF) diagnostics indicated no concerns of multicollinearity (all VIF < 2). Results from hierarchical OLS regression on PIL are displayed in Table 3.
Regression analysis of predictors associated with PIL (N = 150).
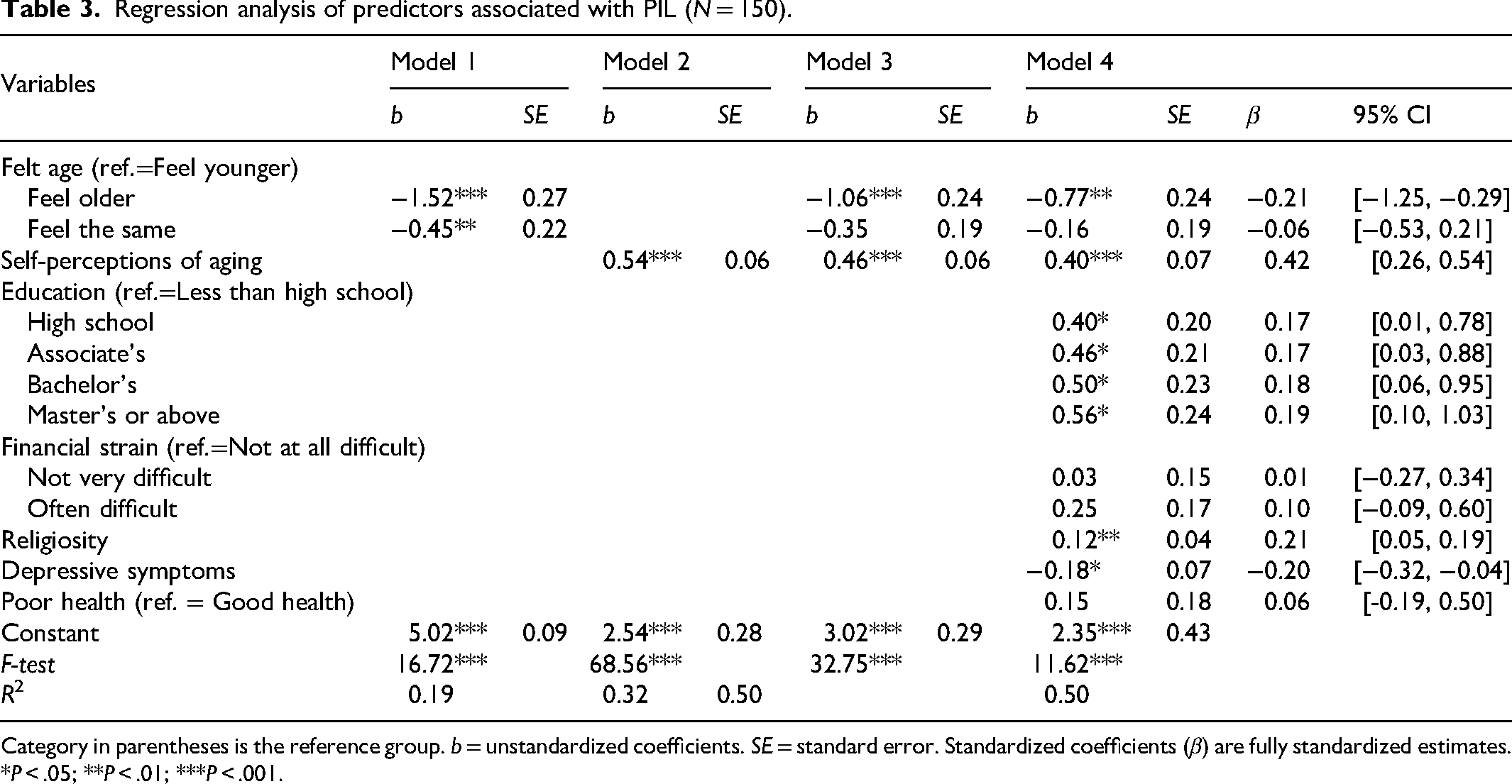
Category in parentheses is the reference group. b = unstandardized coefficients. SE = standard error. Standardized coefficients (β) are fully standardized estimates.
*P < .05; **P < .01; ***P < .001.
Model 1 examined the unadjusted association between felt age and PIL. Feeling older than one's chronological age was associated with significantly lower PIL, while feeling the same age was associated with moderately lower PIL relative to feeling younger. Felt age accounted for 19% of the variance in PIL (R2 = .19, F(2, 147) = 16.72, p < .001). Model 2 tested the unadjusted association between SPA and PIL. SPA was strongly and positively associated with PIL, accounting for 32% of the variance (R2 = 0.32, F(1, 148) = 68.56, p < .001). Model 3 included both felt age and SPA. The negative association between feeling older and PIL was attenuated but remained significant, whereas the association for feeling the same age was no longer significant. This model explained 40% of the variance in PIL (R2 = .40, F(3, 146) = 32.75, p < .001).
Model 4 added educational attainment, financial strain, religiosity, depressive symptoms, and poor self-rated health to Model 3. Religiosity was positively associated with PIL and depressive symptoms were negatively associated with PIL. Financial strain and poor health were no longer significant. Both subjective aging measures remained significant but with reduced effect sizes. Model 4 explained 50% of the variance in PIL (R2 = .50, F(12, 137) = 11.62, p < .001), indicating that subjective aging and psychosocial resources contribute uniquely to purpose in later life.
Discussion
This study examined the correlates of PIL, with a focus on the understudied relationship between subjective aging and purpose in later life. Extending prior research that has identified positive associations between SPA and PIL (Hedberg et al., 2010; Joshanloo, 2024; Kim et al., 2019a; 2019b), this study incorporated both SPA and felt age to capture multiple dimensions of subjective aging. Findings showed that each was strongly associated with PIL, and key dimensions of subjective aging remained associated with PIL after adjusting for sociodemographic, psychological, and health-related factors. Feeling older than one's chronological age remained significantly associated with lower purpose, whereas more positive SPA was associated with higher purpose, underscoring the central role of subjective aging perceptions in eudaimonic well-being.
Consistent with—and extending—previous work reporting that SPA more strongly predicts health-related outcomes than felt age (Westerhof et al., 2023), SPA showed a stronger association with PIL than felt age. This difference may reflect measurement distinctions: SPA is a multi-item construct that captures a broader range of age-related beliefs, whereas felt age relies on a single-item subjective comparison to chronological age. The present findings highlight the conceptual and empirical value of considering multiple indicators of subjective aging and demonstrate their unique contributions to older adults’ sense of purpose (Sabatini et al., 2025).
Beyond subjective aging, educational attainment, religiosity, and depressive symptoms emerged as significant correlates of PIL. These results align with prior research linking greater purpose to higher educational attainment and intrinsic religiosity (Irving et al., 2017), potentially reflecting increased opportunities for meaningful engagement and established goals and value systems that support a sense of direction (Emmons, 2005). Depressive symptoms were inversely related to purpose, consistent with earlier research showing that mood and motivation are closely tied to meaning-making processes (Fischer et al., 2023; Mei et al., 2021), reinforcing the notion that mental health plays a critical role in sustaining purpose in old age (Pinquart, 2002). These findings reaffirm that psychological well-being and purpose are intertwined in later life.
Financial strain and self-rated health were negatively correlated with PIL at the bivariate level but nonsignificant in the fully adjusted model. Although prior literature links financial strain to psychological distress and diminished well-being (Ettman et al., 2023) and poor health to reduced purpose (Irving et al., 2017), the present results suggest that the associations between financial strain, poor health, and PIL may reflect shared variance with subjective aging, depressive symptoms, or other psychosocial factors. Whether these represent indirect pathways cannot be determined from cross-sectional data alone, and formal mediation testing in future longitudinal work would be needed to confirm this possibility. These findings nonetheless highlight subjective aging as a salient correlate of purpose, beyond material or health-related stressors.
No significant associations between PIL and chronological age, gender, race, or partner status were observed. Although Irving et al. (2017) reported demographic differences in purpose, the lack of such variation in this study may reflect the demographic diversity of the sample, which included substantial representation across racial/ethnic groups, immigrant status, gender, and partnership. These findings may suggest that purpose is broadly accessible across demographic groups within this sample. Future work should explore how protective social, cultural, or psychological factors sustain purpose across diverse populations.
The substantial proportion of foreign-born participants in this sample raises important questions about cultural variation in subjective aging processes. Stereotype Embodiment Theory (Levy, 2009) posits that aging stereotypes internalized across the life course shape health and well-being outcomes in later life. However, the degree to which this process operates uniformly across cultural contexts remains unclear. Immigrant older adults may draw on culturally distinct frameworks for understanding aging that differ from those prevalent in U.S. society, potentially serving as a protective factor against the internalization of negative aging stereotypes. Future research should examine whether nativity moderates the relationship between subjective aging and PIL, and whether culturally tailored interventions are needed to promote positive aging perceptions among immigrant older adult populations.
Several limitations warrant consideration. The cross-sectional design precludes causal inference and cannot disentangle the directionality of associations. Longitudinal and experimental studies are needed to determine whether subjective aging shapes purpose, purpose shapes subjective aging, or both. The internal consistency of the GDS-5 was at the lower bound of acceptable reliability (α = .60). Although the GDS-5 is a commonly used brief screening tool, its relatively modest alpha in the present sample may introduce some measurement imprecision in the assessment of depressive symptoms as a covariate. Future studies should consider using longer depression measures with stronger internal consistency to replicate and extend these findings. Additionally, the sample was limited to community-dwelling older adults, and future work should examine whether findings extend to institutionalized populations or those with greater functional limitations. Subjective aging is also multidimensional; constructs such as the Age-related Cognitions (AgeCog) and Awareness of Age-related Change (AARC) may capture additional aspects of aging perceptions not reflected in SPA or felt age (Sabatini et al., 2024). Incorporating these measures would offer a more comprehensive view of how individuals perceive their aging and how these perceptions relate to purpose.
Despite these limitations, the present study is among the first to examine subjective aging using both SPA and felt age in relation to PIL. By demonstrating their independent and combined predictive value, the findings identify subjective aging as an important correlate of older adults’ sense of purpose—a core domain of eudaimonic well-being (Ryff & Keyes, 1995). SPA is malleable and responsive to interventions (Kotter-Grühn, 2015), suggesting that strengthening positive attitudes toward aging may represent a promising target for enhancing purpose and well-being in later life. Another strength of this study is its demographic diversity. Participants represented varied racial, ethnic, and geographic backgrounds, with nearly one-third born outside the United States. This diversity addresses a persistent gap in gerontological research, which has often drawn from homogeneous samples, and supports the feasibility and importance of capturing more inclusive perspectives on aging.
The broader implications for research, practice, and policy are notable. Interventions targeting negative aging stereotypes may bolster purpose in later life. Educational and spiritual resources may sustain meaning-making across the life course, while mental health support remains essential for supporting purpose-enhancing processes. Together, these findings emphasize that subjective aging is a key correlate of well-being and a promising target for psychosocial and community-based interventions. In sum, this study contributes new evidence that both felt age and SPA uniquely shape older adults’ sense of purpose. By identifying subjective aging as a key pathway to meaningful living, the findings highlight opportunities for intervention and underscore the importance of fostering positive SPA to promote healthier, more purposeful aging trajectories.
Footnotes
Ethical Approval and Informed Consent Statements
The data analyzed in this study were collected as part of a larger project approved by the Institutional Review Boards of Western Carolina University and California State University, Dominguez Hills. All participants provided informed consent.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Data collection was partially supported by a 2019 Intentional Learning Plan Grant from Western Carolina University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.