
Abstract
Introduction
Loneliness is a significant and growing public health concern experienced by older adults as, according to a national study, more than one-third of people aged 50 to 80 have reported experiencing loneliness or social isolation (Gerlach et al., 2024). Researchers have identified a variety of factors that contribute to loneliness in this population that include a reduction in social networks following retirement, the loss of a spouse, and chronic health challenges (Cohen-Mansfield et al., 2016; Niino et al., 2025; Vozikaki et al., 2018; Warner et al., 2019). Retirement is also a key life transition that often contributes to older adults experiencing a loss of work-based relationships that results in increased loneliness (Kauppi et al., 2021; Segel-Karpas et al., 2018).
Older adults often pursue effective coping strategies such as initiating new routines and activities and engaging in organized recreational programs to actively manage the increasing psychological distress related to negative emotions such as loneliness (Chen et al., 2025; Hadida-Naus et al., 2025; Kharel et al., 2024). Despite the importance of adaptive coping strategies, research has provided evidence that many older adults also use maladaptive coping behaviors such as alcohol consumption to alleviate the emotional distress they experience that is related to increasing levels of loneliness (Boumans et al., 2022; Chang et al., 2024; Fenollal-Maldonado et al., 2022). For example, Wakabayashi et al. (2022) found that individuals with high levels of loneliness reported a 45% greater risk of transitioning to hazardous levels of alcohol consumption when compared to their less lonely counterparts. Additionally, individuals who reported moderate or severe loneliness in the prior two weeks were more likely to report a higher frequency of alcohol use compared to those who had not experienced loneliness (Gutkind et al., 2022). Unhealthy lifestyle patterns such as alcohol use that have been found in previous research are concerning as they may ultimately contribute to the development of lifestyle-related diseases including obesity, mental health disorders, and cardiovascular disease (Arora et al., 2022; Garg, 2025). Therefore, it is of critical importance to educate older adults experiencing loneliness about healthy coping strategies and to encourage their adoption.
Participation in leisure time physical activity (LTPA) is considered an effective coping strategy that improves the health and wellbeing of older adults (Kim et al., 2025; Park et al., 2025) and people with disabilities who are vulnerable to stress (Han et al., 2019; Kim et al., 2021a, 2021b). In particular, for older adult populations, a growing body of research has provided evidence of the positive contributions of LTPA participation in reducing their loneliness. For example, Surkalim et al. (2024) found that middle-aged and older adults who engaged in LTPA such as walking and dancing were more likely to report lower levels of loneliness 2 years later. Similarly, participation in sport programs (e.g., shuffleboard, basketball, golf, and baseball) also played a significant role in reducing the loneliness levels of older adults (Bedini et al., 2019). These findings suggest that engagement in LTPA may serve as an effective strategy for managing loneliness in older adults.
LTPA is often categorized based on activity intensity, with moderate leisure-time physical activity (MLTPA) referring to activities that moderately raise heart rate, such as walking and slow jogging, and vigorous leisure-time physical activity (VLTPA) referring to higher-intensity activities that significantly increase heart rate and breathing, such as running and fast cycling. Han et al. (2021) found that older adults who participated in higher levels of MLTPA, such as leisure walking, tended to report perceiving higher levels of mental and general health. Some studies have found that VLTPA participation has been associated with enhanced social connectedness and a sense of community that may contribute to the alleviation of loneliness and a reduction in social isolation (Gravelle et al., 2025; Leirós-Rodríguez et al., 2018). Overall, previous findings suggest that both MLTPA and VLTPA are associated with improved mental health in older adults.
In addition to the general health benefits of LTPA participation, earlier research has also provided evidence that different intensities of LTPA have distinct effects on health outcomes. For example, Kim et al. (2020) found that, when compared to light-to-moderate forms of LTPA, participation in VLTPA was a stronger predictor of the mental health of older adults in the United States. Similarly, the findings of Joshi et al. (2016) showed that older adults who engaged in more active forms of LTPA such as sports and walking were more likely to report better mental health than those who engaged in less active activities such as gardening, or those who were inactive. Additionally, Kim et al. (2025) examined the associations between LTPA intensity and life satisfaction and found that both VLTPA and leisure walking positively influenced the life satisfaction of older adults. More importantly, however, VLTPA participation has been found to produce a stronger positive effect on life satisfaction among older adults with dementia than among those without dementia. These findings suggest that different LTPA intensities may have different levels of effect on the mental health outcomes of older adults. Examining these differences is important because different LTPA intensities may influence the mental health of older adults through distinct psychosocial and physiological mechanisms (Bedini et al., 2019; Kim et al., 2020).
Earlier research has provided valuable insights into loneliness as a primary driver of late-life alcohol abuse (i.e., loneliness → alcohol consumption; Rhew et al., 2025; Wakabayashi et al., 2022). However, relatively little research has examined the inverse relationship (i.e., alcohol consumption → loneliness) or the extent to which alcohol consumption influences loneliness in older adults. In fact, it has been suggested that the relationship between loneliness and alcohol consumption may be cyclical, such that individuals who experience loneliness may increase alcohol use, and, in turn, those who consume alcohol may experience more intense loneliness (Abdellaoui et al., 2019). However, a study evaluating the reciprocal relationship in a European context found no significant association between loneliness and alcohol use or dependence in either direction (Wootton et al., 2021). As such, further research is needed to identify possible intervening factors that influence the negative interactions between loneliness and alcohol consumption and potentially disrupt this cycle.
Based on our review of the previous literature, we hypothesized that either or both MLTPA and VLTPA participation would serve as a potential moderator that could weaken the negative impact of alcohol consumption on loneliness in older adults. To date, few studies have examined the moderating effect of LTPA participation on this relationship, especially among older adults at a national level, and there has been limited research conducted to explore how the intensity of LTPA participation (i.e., MLPTA and VLTPA) may differentially provide health benefits within this context. Examining the relationships between alcohol consumption, LTPA participation and loneliness may provide insight into the moderating role of LTPA in buffering the negative effects of alcohol consumption on the loneliness of older adults.
Therefore, in this study we investigated whether MLTPA and VLTPA participation moderates the relationship between alcohol consumption and loneliness in older adults. Specifically, we tested these potential moderating effects using data from the Health Information National Trends Survey (HINTS), a cross-sectional, nationally representative survey of the non-institutionalized adult population in the United States. Our findings have significant potential to inform the design of the health education and promotion programs with the goal of encouraging the use of healthier coping strategies and reducing feelings of loneliness in later life. Specifically, we tested the following hypotheses:
Hypothesis 1 (H1): Alcohol consumption is associated with loneliness in older adults.
Hypothesis 2 (H2): Moderate levels of leisure time physical activity participation moderate the relationship between alcohol consumption and loneliness in older adults in a negative direction.
Hypothesis 3 (H3): Vigorous levels of leisure time physical activity participation moderate the relationship between alcohol consumption and loneliness in older adults in a negative direction.
Methods
Data and Samples
We utilized data from the HINTS 7 (2024), administered by the National Cancer Institute (NCI). HINTS data collection used both paper and internet questionnaire protocols and a two-stage sampling design based on residential addresses. In the first stage, a random sample of household addresses was selected. In the second stage, one adult aged 18 years or older from each selected household was invited to complete the questionnaire. A total of 7,278 respondents were included in the dataset, of whom 7,208 completed at least 80% of sections A and B. For our analysis using section B, the inclusion criteria were: (a) participants must be 60 years of age or older, (b) data must be available on alcohol consumption, MLTPA and VLTPA participation levels, and loneliness, and (c) complete observations must be available on covariates (age, sex, educational attainment, household income). Thus, based on these inclusion criteria, a total of 3,213 participants were included in this study. Ethical review of this study was conducted by the National Cancer Institute (NCI) as part of the HINTS program. As the publicly available dataset contains no personally identifiable information, this secondary analysis did not require additional institutional review.
Instruments
Independent Variables
Alcohol Consumption
Alcohol consumption was assessed using the item “During the past 30 days, how many times did you have alcoholic drinks on one occasion?,” which measured the frequency of alcohol consumption episodes over the previous 30 days. Responses ranged from “Never” to “11 or more times.” This variable was treated as a continuous measure, with higher values indicating more frequent alcohol consumption.
Moderating Variables
Moderate Leisure Time Physical Activity (MLTPA)
MLTPA participation was measured using the item “How long do you usually engage in moderate intensity exercise each day?,” recorded as the total number of minutes of moderate activity per day. Responses ranged widely, from 7 to over 600 minutes per day that reflected time spent in activities such as brisk walking, cycling at a casual pace, or other exercises requiring moderate effort. This variable was treated as a continuous measure with higher values indicating higher levels of MLTPA engagement.
Vigorous Leisure Time Physical Activity (VLTPA)
VLTPA was assessed using the item “In a typical week, outside of your job or work around the house, how many days do you participate in leisure-time physical activities specifically designed to strengthen your muscles, such as lifting weights or circuit training?” Respondents indicated the number of days per week they engaged in muscle-strengthening or high-intensity exercises including activities such as weightlifting, resistance training, or circuit workouts. Responses ranged from 0 to 7 days per week, with higher scores indicating more frequent participation in VLTPA. This variable was treated as a continuous measure representing the weekly frequency of vigorous activity in the analysis.
Dependent Variable
The loneliness variable in HINTS 7 was assessed using the PROMIS Social Isolation Scale T score. This measure was derived from four items, “FeelLeftOut,” “FeelPeopleBarelyKnowMe,” “FeelIsolated,” and “FeelPeopleNotWithMe,” each capturing distinct aspects of perceived social isolation. Responses to these items were combined and converted to a standardized T score following the Patient Reported Outcomes Measurement Information System (PROMIS) scoring procedures. These T scores are normed to the US general population with a mean of 50 and a standard deviation of 10 in which higher T scores indicate higher levels of feelings of loneliness or social isolation and lower scores reflect lower levels of perceived isolation and higher levels of social connectedness. In this study, isolation was treated as a continuous variable with higher continuous values representing higher levels of loneliness.
Controlled Variables
Age was measured as a continuous variable based on self-reported age in years. Sex was assessed using a self-reported item asking participants to indicate their biological sex at birth (male = 0, female = 1). Educational attainment was measured by asking, “What is the highest grade or level of schooling you completed?” with responses categorized as less than high school (1), high school graduate (2), some college (3), bachelor's degree (4), or graduate degree (5). Household income was measured as total annual household income before taxes, reported in categories ranging from “$0–$9,999” to “$200,000 or more.”
Analysis
The goal of this analysis was to determine the effect of alcohol consumption on loneliness and to identify whether MLTPA and VLTPA participation moderated this relationship in older adults. Prior to the main analysis, descriptive statistics were computed to summarize participant demographic characteristics. Hierarchical regression models were then conducted to examine the association between alcohol consumption and loneliness (Model 1), the moderating effect of MLTPA participation on the relationship between alcohol consumption and loneliness (Model 2), and the moderating effect of MLTPA and VLTPA participation on the relationship between alcohol consumption and loneliness (Model 3) while controlling for age, sex, educational attainment, and household income. Changes in explanatory power were evaluated using R2 differences across models. All analyses were performed using SPSS version 30.0.
The regression equation we used to test research hypotheses are below:

H1: Alcohol consumption is associated with loneliness.
H2: Moderate levels of leisure time physical activity participation moderate the relationship between alcohol consumption and loneliness in a negative direction.
H3: Vigorous levels of leisure time physical activity participation moderate the relationship between alcohol consumption and loneliness in a negative direction.
Results
Table 1 summarizes the descriptive characteristics of the study participant sample that consisted of 3,213 adults 60 to 88 years of age with a mean age of 71.39 years (SD = 7.81). Of the total sample, 43.6% (n = 1,400) were men and 56.4% (n = 1,813) were women. Nearly half of study participants were married (45.8%, n = 1,472), while 2.5% (n = 81) were living with a romantic partner, 18.8% (n = 605) were divorced, 19.4% (n = 622) were widowed, 2.8% (n = 88) were separated, and 10.7% (n = 345) were single. Regarding educational attainment, 7.6% (n = 245) reported having less than a high school education, 18.6% (n = 598) were high school graduates, 32.9% (n = 1,059) had some college education, 21.9% (n = 703) held a bachelor's degree, and 19.0% (n = 608) held a graduate degree. Household income varied widely: 7.0% (n = 225) reported annual income below $10,000, whereas 6.1% (n = 196) reported an income of $200,000 or more. The mean number of alcoholic drinks consumed per week was 2.01 (SD = 7.00). The average loneliness score was 42.09 (SD = 12.33), suggesting a slightly lower level of perceived social isolation compared with the population norm (T = 50). Participants engaged in an average of 185.86 minutes of moderate physical activity per week (SD = 322.15) and reported 1.43 (SD = 1.96) sessions of vigorous activity per week.
Descriptive Statistics.
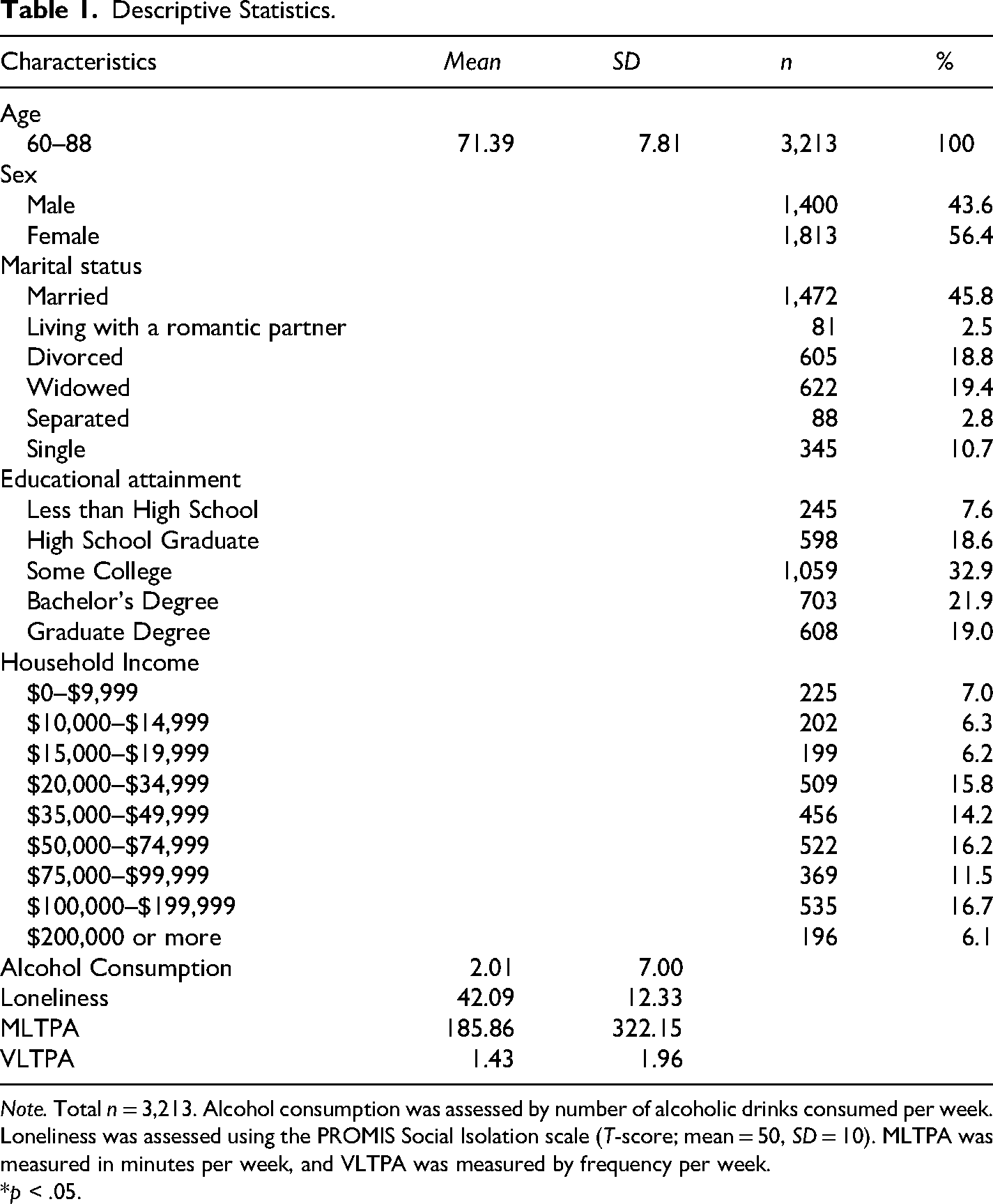
Note. Total n = 3,213. Alcohol consumption was assessed by number of alcoholic drinks consumed per week. Loneliness was assessed using the PROMIS Social Isolation scale (T-score; mean = 50, SD = 10). MLTPA was measured in minutes per week, and VLTPA was measured by frequency per week.
*p < .05.
As shown in Table 2, alcohol consumption was positively associated with education (r = 0.11, p < .05), income (r = 0.14, p < .05), and MLTPA participation (r = 0.05, p < .05), but negatively related to age (r = –0.09, p < .05) and sex (r = –0.18, p < .05). Loneliness was inversely associated with both MLTPA (r = –0.04, p < .05) and VLTPA participation (r = –0.10, p < .05). Education and income were found to have a strong positive association (r = 0.47, p < .05), and MLTPA and VLTPA participation were moderately correlated (r = 0.24, p < .05).
Correlations Between Study Variables.
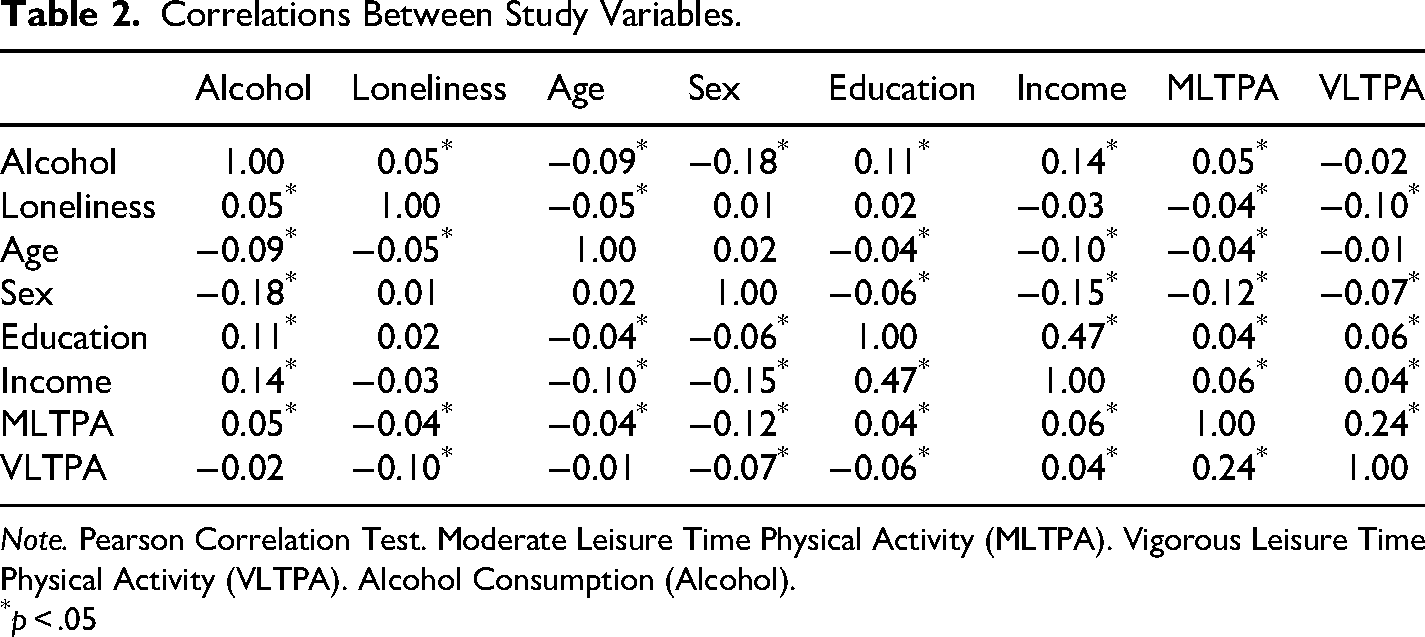
Note. Pearson Correlation Test. Moderate Leisure Time Physical Activity (MLTPA). Vigorous Leisure Time Physical Activity (VLTPA). Alcohol Consumption (Alcohol).
p < .05
Table 3 presents the hierarchical regression models used to assess loneliness. In Model 1, demographic and alcohol consumption variables explained 1.9% of the variance in loneliness (R2 = 0.019, F (5, 1377) = 5.21, p < .01). In Model 2, the interaction between MLTPA participation and alcohol consumption was added, but the explained variance did not improve meaningfully (ΔR2 = 0.001, F (1, 1376) = 0.27, p = .60). When the second interaction term, VLTPA participation × alcohol consumption, was included in Model 3, the model accounted for a slightly greater portion of variance (R2 = 0.024, ΔR2 = 0.010, F (1, 1375) = 4.64, p = .03), indicating a small but statistically significant improvement. The Durbin Watson statistic (1.93) suggested that residuals showed no indication of autocorrelation.
Model Summary.
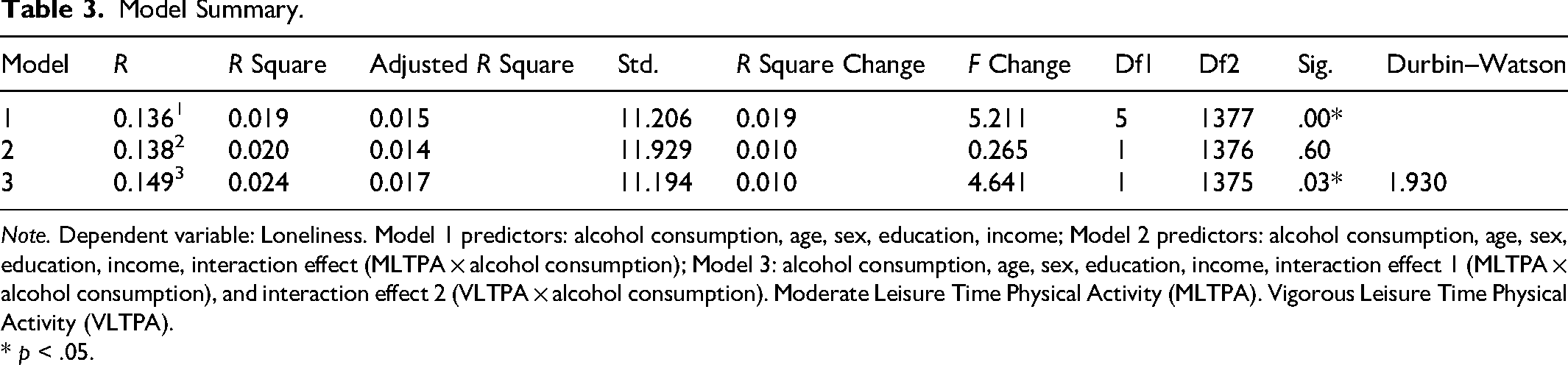
Note. Dependent variable: Loneliness. Model 1 predictors: alcohol consumption, age, sex, education, income; Model 2 predictors: alcohol consumption, age, sex, education, income, interaction effect (MLTPA × alcohol consumption); Model 3: alcohol consumption, age, sex, education, income, interaction effect 1 (MLTPA × alcohol consumption), and interaction effect 2 (VLTPA × alcohol consumption). Moderate Leisure Time Physical Activity (MLTPA). Vigorous Leisure Time Physical Activity (VLTPA).
* p < .05.
Hierarchical regression analyses (Table 4) were then conducted to examine how alcohol consumption was associated with loneliness, with physical activity variables entered in steps to test their interaction effects. In Model 1 (Figure 1), alcohol consumption was entered as the independent variable with age, sex, education, and income included as control variables. The model revealed that alcohol consumption had a significant positive association with loneliness (B = 0.11, SE = 0.04, t = 2.48, p = .01), indicating that higher levels of alcohol consumption were linked to higher levels of perceived loneliness. Among the controls, age (B = −0.08, p = .02) and income (B = −0.57, p < .01) were negatively associated, and education (B = 0.84, p = .01) was positively associated with loneliness. Multicollinearity statistics indicated no issues of concern (Tolerance > 0.70, VIF < 1.4).
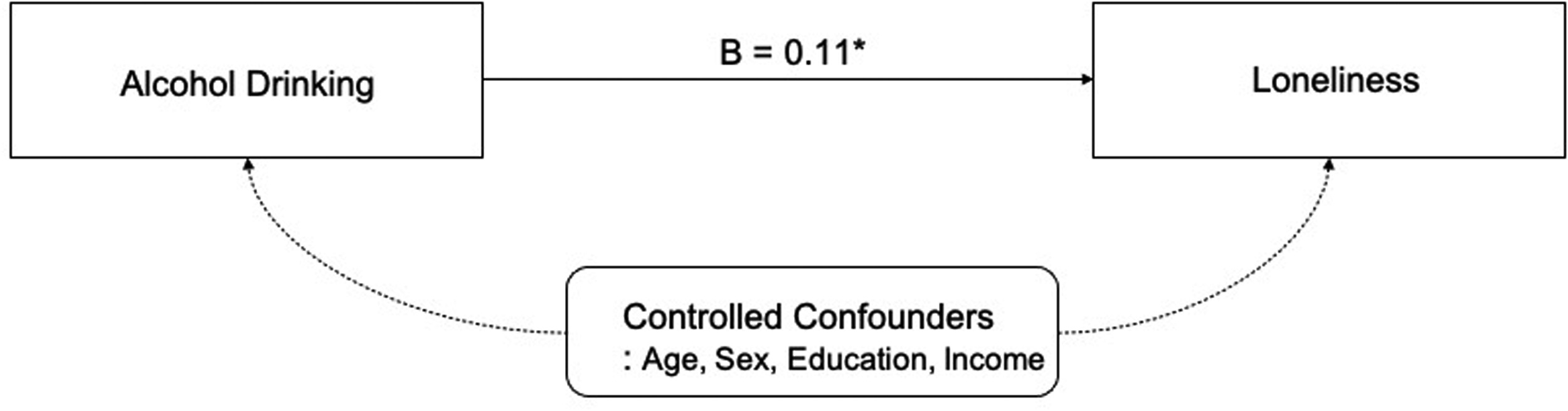
Relationship between alcohol drinking and loneliness. *p < .05.
Regression Analysis Results for Loneliness.
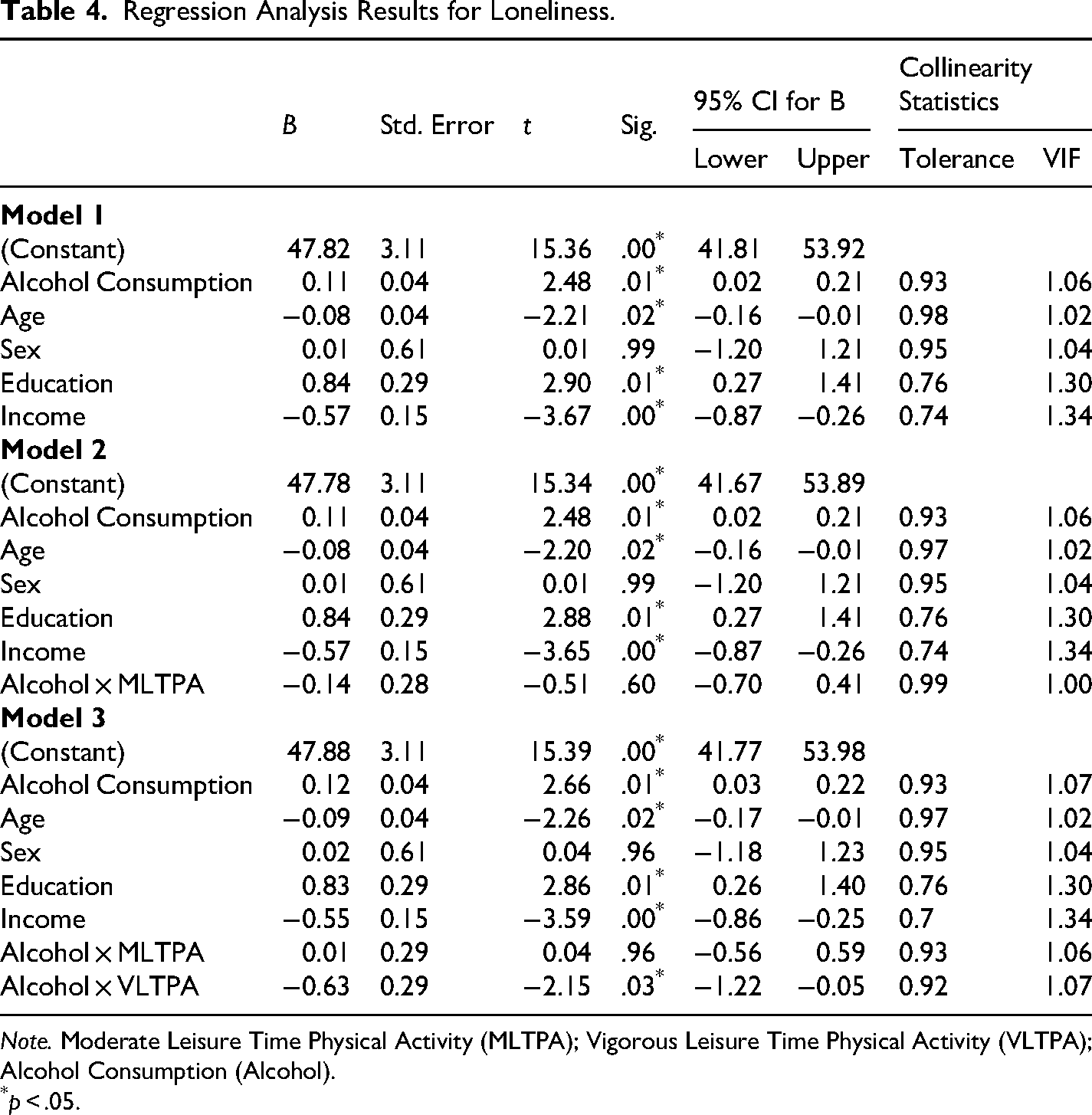
Note. Moderate Leisure Time Physical Activity (MLTPA); Vigorous Leisure Time Physical Activity (VLTPA); Alcohol Consumption (Alcohol).
p < .05.
In Model 2 (Figure 2), an interaction term between alcohol consumption and MLTPA participation was added to test whether moderate levels of leisure time physical activity participation moderated the effect of alcohol consumption on loneliness. The main effect of alcohol consumption remained significant (B = 0.11, SE = 0.04, t = 2.48, p = .01), while the interaction term was not significant (B = −0.14, p = .60), which indicates that MLTPA participation did not meaningfully influence the relationship between alcohol consumption and loneliness. The effects of age, education, and income remained similar in direction and magnitude to Model 1, and no multicollinearity concerns were found (VIF < 1.4).
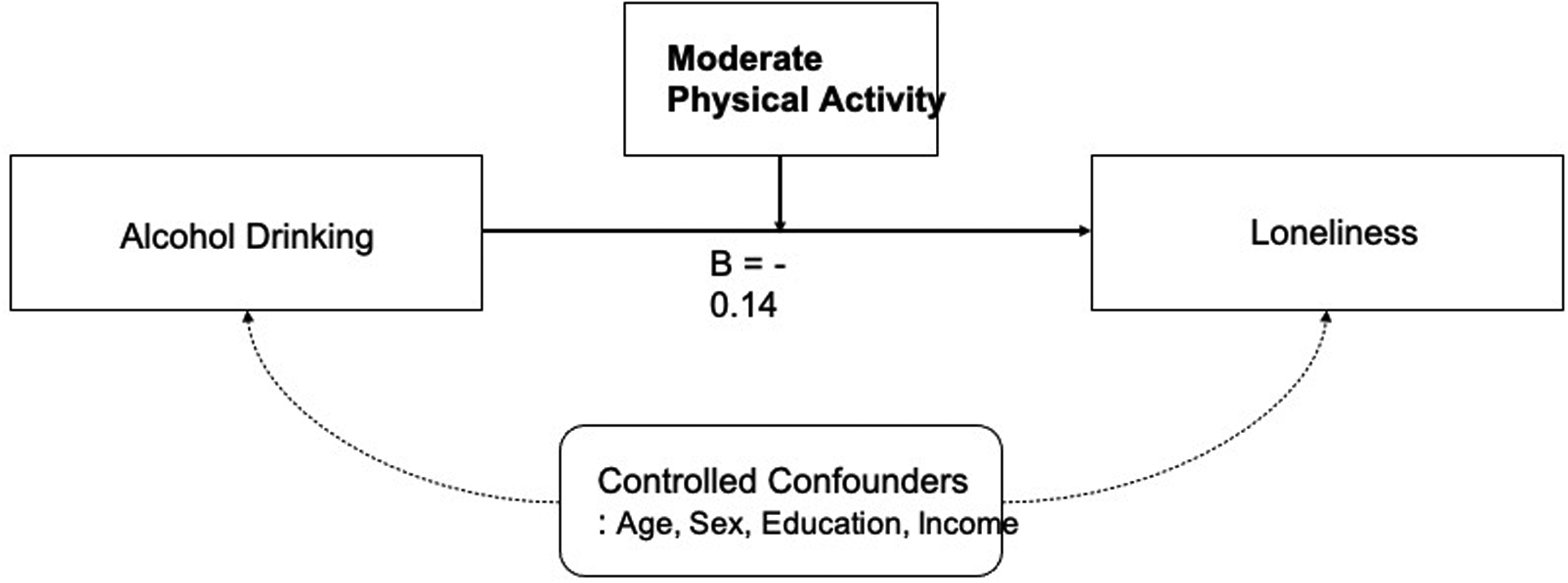
Interaction effect between alcohol drinking and moderate physical activity on loneliness. *p < .05.
In Model 3 (Figure 3), a second interaction term between alcohol consumption and VLTPA participation was added. The main effect of alcohol consumption remained significant (B = 0.12, SE = 0.04, t = 2.66, p = .01) and the interaction between alcohol consumption and VLTPA participation was also significant (B = −0.63, SE = 0.29, t = −2.15, p = .03), suggesting that VLTPA participation moderated the positive relationship between alcohol consumption and loneliness. In other words, individuals who engaged in vigorous exercise experienced a weaker association between alcohol use and loneliness. The interaction between alcohol consumption and MLTPA participation remained non-significant (p = .96). Multicollinearity diagnostics again indicated that the independent variables in the regression model were not highly correlated (VIF < 1.5). Overall, these results suggest that while a higher level of alcohol consumption is generally associated with higher levels of perceived loneliness, engaging in VLTPA can moderate this relationship, highlighting the potentially protective role of intense exercise against alcohol-related loneliness.
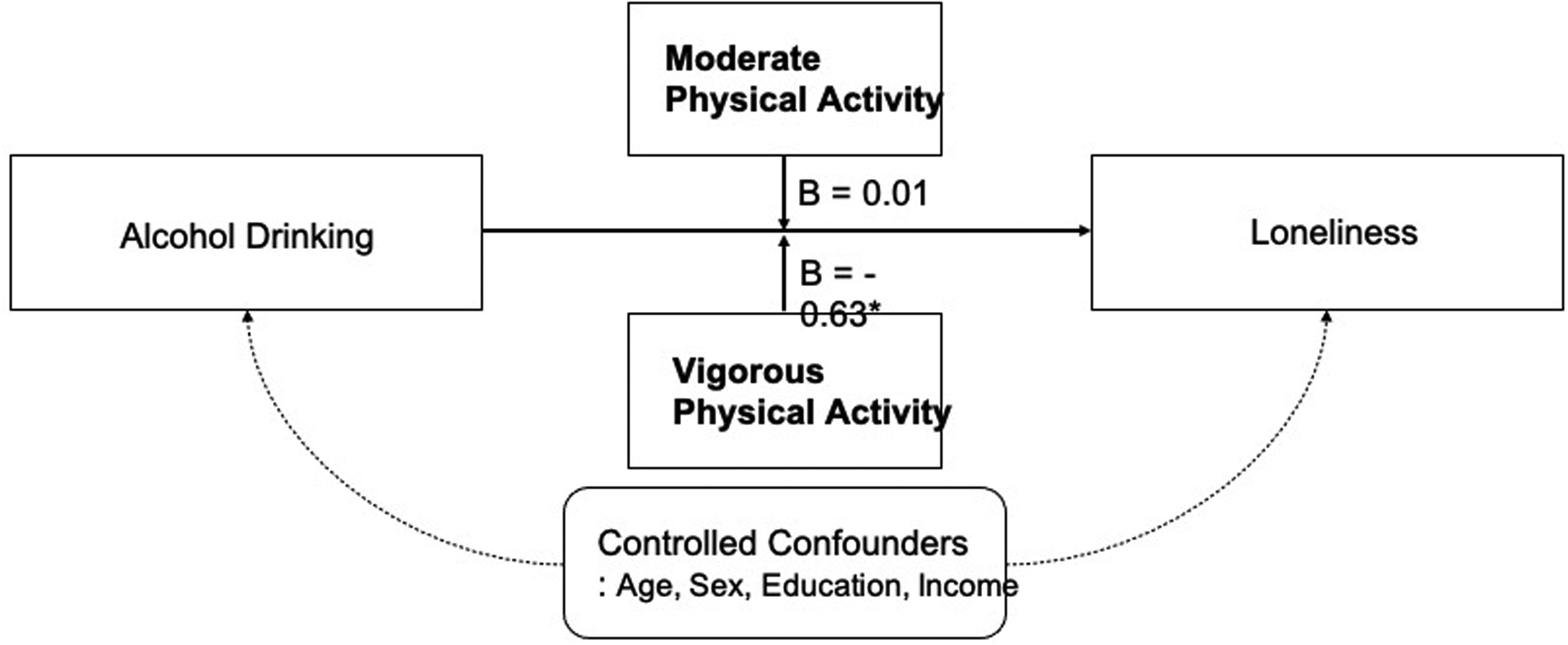
Interaction effect between alcohol drinking, moderate, and vigorous physical activity on loneliness. * p < .05.
Discussion
In this study, we examined the relationship between alcohol consumption and loneliness in older adults and the moderating role of different levels of LTPA participation. Our results provide evidence that higher levels of alcohol use are associated with higher levels of perceived loneliness in older adults. That is, older adults who consume alcohol more frequently may be more vulnerable to loneliness. More importantly, however, we found that the moderating effect of LTPA participation on the relationship between alcohol consumption and loneliness differed depending on the intensity of the LTPA in which older adults had participated. Specifically, older adults who frequently engage in VLTPA experienced lower levels of loneliness even when alcohol use was higher, whereas MLTPA participation did not provide a significant moderating effect. Our findings further highlight the importance of VLTPA participation as a moderator of the loneliness that older adults experience.
Earlier studies that have assessed the impact of loneliness on alcohol use by older adults have provided evidence that older adults who experience higher levels of loneliness tend to consume alcohol more frequently than those experiencing lower levels of loneliness (Adebisi et al., 2024; Gutkind et al., 2022; Johar et al., 2025). Older adults who experience challenges in later life such as limited social networks, the loss of a spouse, and chronic health-related challenges often experience higher levels of loneliness that may increase the likelihood and amount of alcohol consumption (Cohen-Mansfield et al., 2016; Niino et al., 2025; Vozikaki et al., 2018; Warner et al., 2019). When we examined the inverse relationship (i.e., alcohol consumption → loneliness), we found that alcohol use can contribute to higher levels of loneliness in older adults. There are several possible explanations for this finding. Neurologically, alcohol releases dopamine in the reward system of the brain that creates a short-term increase in pleasure and emotional relief. However, repeated alcohol use can dysregulate dopamine functioning and raise the threshold for experiencing positive emotions naturally that may lead to anhedonia, depression, and loneliness (Koob & Volkow, 2016). Socially, alcohol use often has a negative impact on social relationships that can lead to emotional withdrawal, reduced social involvement, and adverse mental and physical health outcomes, such as depressive symptoms and cognitive decline (Abdellaoui et al., 2019). This suggests that older adults who use alcohol as a coping mechanism may become increasingly socially isolated and experience greater feelings of loneliness over time. Overall, the findings of our study expand the existing literature by highlighting the bidirectional nature of the relationship between alcohol consumption and loneliness in later life. Our findings also provide valuable insight into the moderating role of VLTPA participation by providing evidence that engagement in adaptive leisure activities may help replace maladaptive coping behaviors such as alcohol use.
Earlier research findings provided evidence that participation in both light-to-moderate and vigorous LTPA contributes to improving the mental health of older adults (Joshi et al., 2016; Kim et al., 2020). Our findings further suggest that, beyond older adults in general, older adults who consume alcohol more frequently and experience loneliness may only benefit from participation in strenuous forms of LTPA. Our findings suggests that VLTPA participation may play a moderating role in the relationship between alcohol use and loneliness, which is contrary to the findings of previous studies (Kim et al., 2020), and that moderate levels of LTPA participation did not appear to provide the same reduction in loneliness for older adults with higher levels of alcohol consumption as did VLTPA participation. Kim and colleagues (2019, p. 297) noted that, “although the majority of older adults may predominately engage in light-to-moderate LTPA (e.g., walking), greater benefits for mental health could be derived by more strenuous types of LTPA (e.g., jogging, recreational sports).” Accordingly, our findings underscore the importance of engagement in VLTPA to reduce the loneliness that older adults experience.
Several mechanisms have been found to support a stronger moderating effect of VLTPA than light-to-moderate activity (López-Bueno et al., 2023). VLTPA may produce greater physiological and psychological benefits including better stress management, increased feelings of mastery and self-efficacy, and improved mood through neurobiological reactions (Yang et al., 2025). These authors stated that VLTPA, especially in the form of sport activities, improves regulatory emotional self-efficacy and reduces self-perceived burden, both of which improve mental health in older adults. Further, VLTPA is often delivered in organized or group settings that may promote higher levels of social interaction and further enhance the life satisfaction and psychological wellbeing of older adults who experience loneliness (Kim et al., 2025; Park et al., 2025). Overall, these mechanisms highlight VLTPA as a more effective, health-promoting behavioral option that may be particularly beneficial for older adults who use alcohol to cope with loneliness.
Our findings suggest important implications for promoting mental wellbeing, particularly among older adults who drink more frequently to cope with loneliness. Our findings indicate that VLTPA may serve as a healthy leisure choice that buffers the negative psychological consequences of alcohol use. Accordingly, health professionals and recreation program providers may consider offering community-based programs that integrate VLTPA as an effective coping strategy to address loneliness. Earlier related research findings suggest that programs incorporating more vigorous forms of recreational activity such as cycling, brisk walking, swimming, and dance-based activities can positively contribute to multiple aspects of health and lifestyle that include physical health, social relationships, and reductions in unhealthy coping behaviors such as alcohol use (Halaweh et al., 2015; Tao et al., 2025). In addition, the findings of earlier studies further suggest that physical activity programs incorporating social interaction components may have additional positive effects on reducing the loneliness experience by older adults (Ahn et al., 2024; Sebastião & Mirda, 2021). These findings underscore the importance of public health policies that promote active aging through improved access to affordable and socially engaging health-promoting opportunities for older adults. In this regard, local senior centers, aging-service organizations, and substance use treatment centers can play a key role in reducing the loneliness associated with older adult alcohol use by expanding age-friendly physical activity infrastructure and programs that encourage consistent social engagement and healthy coping behaviors.
From a practical standpoint, we emphasize the importance of designing and providing accessible physical activity programs for older adults. Due to physical limitations or medical conditions, some older adults may not be able to safely participate in traditional forms of VLTPA. Therefore, health professionals and service providers should consider adaptive approaches to VLTPA that balance intensity and safety while accounting for the range of functional abilities present in older participants. For example, modified or supervised forms of vigorous activity such as chair-assisted aerobic activities or low-impact dance programs, may still yield psychosocial benefits while ensuring the safety of older participants (Klempel et al., 2021). In addition to practitioner efforts, we suggest that future studies employ experimental and longitudinal designs to clarify the causal relationships between VLTPA participation, alcohol consumption, and loneliness. Intervention studies would also be useful in examining whether increasing VLTPA leads to subsequent reductions in alcohol consumption and loneliness. Lastly, it is necessary to examine a wide variety of LTPA intensity levels in research to better understand the distinct psychosocial effects associated with each intensity level, and to provide the critically needed data that is necessary to guide the development of intensity-specific interventions whose goal is to support healthy aging.
Limitations
Several limitations inherent to this study must be acknowledged. First, the cross-sectional design of this study did not allow for a longitudinal analysis of how alcohol consumption influences psychological wellbeing over time. A deeper understanding of alcohol consumption behaviors in a time-dependent context will provide stronger evidence for causal inferences, rather than capturing a single alcohol use episode potentially driven by impermanent life events. Future research should employ mixed effects models with longitudinal data to assess both the fixed and random effects of alcohol consumption behaviors on psychological wellbeing.
Second, our study included limited information on the amount and type of alcohol consumed and the presence or absence of companions during alcohol consumption, factors that may be associated with loneliness. Further, the incorporation of covariates related to alcohol metabolism such as height, weight, and body mass index would also help clarify the health implications of alcohol consumption behaviors.
Third, potential confounders related to LTPA participation were not adequately considered in this study. Given that the mean age of the participants was 71 years, many were likely to experience functional limitations that affected their ability to engage in LTPA. In particular, MLTPA or VLTPA participation may be less accessible for older adults who tend to prefer light intensity LTPAs such as yoga, walking, and tai chi that require lower levels of muscle strength and aerobic capacity. Future studies should incorporate measures of functional status, such as activities of daily living, to better account for these limitations. This approach would help clarify the benefits of MLTPA and VLTPA participation while considering the age-related constraints on physical activity participation that must be considered when developing tailored LTPA based wellness programs for older adults.
Conclusions
For older adults experiencing loneliness, alcohol consumption may serve as an easily accessible coping strategy to manage feelings of loneliness related to disconnection from family or community. However, our findings indicate that alcohol consumption is not an effective strategy for alleviating feelings of isolation. Instead, we found that alcohol consumption behaviors were negatively associated with the loneliness that can be experienced by older adults. We did find that VLTPA participation moderates this relationship and helps reduce the loneliness experienced by older adults who consume alcohol, whereas MLTPA participation was not associated with a significant reduction in perceived loneliness. Encouraging participation in physical activity that accounts for age-related functional limitations, alongside fostering intergenerational engagement with family and community members, underscores the importance of promoting healthy behaviors rather than merely prohibiting unhealthy ones. Our findings further suggest that carefully tailored community programs may offer a sustainable approach to reducing the loneliness that can be experienced by older adults.
Footnotes
Ethical Consideration
This study utilized publicly available anonymized databases, and as such, was exempt from ethical compliance review.
Authors’ Contributions
Jaehyun Kim did conceptualization, project administration, writing the original draft, writing—review and editing.
Jungjoo Lee did conceptualization, data curation, formal analysis, investigation, methodology, writing the original draft.
Junhyoung Kim performed supervision, validation, writing the original draft, writing—review and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interest
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Generative AI and AI-Assisted Technologies in the Writing Process
Not applicable.
Data Availability
The data are publicly available on the Health Information National Trends Survey website.