
Abstract
This study investigates the relationship between life expectancy among older adults and key fiscal variables such as state development expenditure, central development expenditure, and pension expenditure, using an auto-regressive distributed lag model. The analysis explores both short- and long-run dynamics over an extended period. Results show that state and central development expenditures have a significant positive impact on the life expectancy of men aged 60 and above. However, lagged central development expenditure exerts a negative and statistically significant effect on the life expectancy of older adult women, suggesting potential gender disparities in the benefits of public spending. Bounds testing confirms a stable long-run association between the fiscal variables and life expectancy among older adults. The findings underscore the importance of inclusive and gender-sensitive development policies to enhance the quality of life for older adults in India, offering valuable insights for fiscal planning.
Introduction
Ageing is an inevitable outcome of demographic shifts, with its extent and progression differing across countries based on the timing and speed of population growth (Bongaarts, 2004). India stands on the cusp of a significant demographic transition, which has far-reaching implications for its economic and social fabric. With an ageing population projected to reach 20% of the total population by 2050 (United Nations, 2019), India faces a looming challenge in ensuring economic security for its elderly citizens. This demographic shift, driven by rising life expectancy and declining fertility rates, highlights the urgent need to understand and address the vulnerabilities faced by older adults (Visaria, 2022). Access to adequate economic support, healthcare services, and social security remains limited for a large section of the older adult population. These challenges are particularly severe in rural areas, where poverty levels and dependency ratios are comparatively higher (Bloom et al., 2010; Mutchler et al., 2015; Sahoo et al., 2023).
Ageing and economic security are closely interconnected, particularly in India, where traditional family-based support systems for older adults are gradually weakening (Das & Dhillon, 2024). In a country where more than 90% of the workforce is employed in the informal sector, only a small proportion of individuals are covered by formal pension systems (ILO, 2018; Roy & Barua, 2023). As a result, ageing is often associated with declining income levels and increasing economic vulnerability. Limited access to universal healthcare further intensifies these challenges.
Older adults frequently experience rising healthcare expenditures without adequate savings or insurance coverage to manage these costs (Agarwal et al., 2020). Such financial pressures affect not only the well-being of elderly individuals but also place a significant burden on families, who continue to serve as the primary caregivers in many households (Lena et al., 2009). In addition, the gradual decline of the joint family system has increased the risk of social isolation and financial dependence among older adults. Although welfare programmes such as the National Social Assistance Programme (NSAP) provide some support, their coverage and adequacy often remain insufficient to address the growing needs of India's ageing population.
The projected increase in the elderly population in both absolute and relative terms is a subject of growing concern for policymakers and pension economists in many countries (Bloom et al., 2010; Rajan, 2008). Globally, research on ageing has highlighted the importance of economic security as a determinant of quality of life for the elderly (Foster & Walker, 2015; Kalache & Keller, 2000; Walker, 2005). Social security aims to safeguard the well-being of individuals within a state, industry, institution, or family. It aims to ensure access to basic necessities such as food, shelter, clothing, education, clean water, and healthcare, while also protecting individuals from unforeseen risks (Goli et al., 2019). Evidence from developed countries with strong social security systems shows that income security and accessible healthcare play important roles in reducing the adverse effects associated with ageing (Börsch-Supan, 2013; Dave & Kaestner, 2009; Holzmann, 2005).
As India experiences a profound demographic shift, with a rapidly growing ageing population, questions about how public policies shape the well-being and longevity of older adults have never been more important. Hence, the research question guiding this study is: What is the impact of state and central development expenditures, including pension expenditures (PEs), on the life expectancy of older adults in India, and do these effects differ by gender in both the short and long run? This question focuses on how different components of public development spending influence the longevity of older adults, explicitly considering potential gender disparities. The analysis emphasises understanding both short-term and long-term dynamics, using an auto-regressive distributed lag (ARDL) modelling approach. Through this framework, the study aims to provide a comprehensive assessment of the relationship between fiscal policy and life expectancy outcomes among older adults in India.
Despite the growing literature on ageing and economic security in India, limited research has examined the direct impact of state and central pensions on life expectancy among the elderly population. Existing studies have primarily explored the adequacy of pensions and their role in reducing poverty among older adults (Pal & Palacios, 2011). However, the extent to which these financial provisions influence life expectancy remains understudied. This gap is particularly critical given India's demographic transition, where life expectancy is increasing, but disparities persist across gender and socioeconomic groups. Previous research suggests that financial security in old age improves access to healthcare and nutrition, thereby potentially enhancing longevity (Bloom et al., 2015a). However, empirical evidence on whether state and central pension schemes contribute to differential life expectancy outcomes between elderly men and women in India is scarce.
The longitudinal ageing study in India (LASI) provides some insights into elderly well-being. However, it does not explicitly analyse the causal relationship between pension benefits and life expectancy (Arokiasamy et al., 2012). Addressing this gap is essential for policymakers to assess the effectiveness of pension schemes in improving not just economic stability but also health and longevity outcomes among India's ageing population. Ultimately, this research aims to contribute to a framework that not only supports the financial and health needs of the elderly but also fosters a more inclusive and economically secure ageing population in India.
Literature Review
India's rapidly ageing population is reshaping its socioeconomic landscape, posing significant implications for economic security and social policy. As the elderly population increases, understanding the vulnerabilities that older adults face becomes crucial for developing effective policy interventions (Agarwal et al., 2020). Economic security, encompassing income stability, healthcare access, and social support, is a key factor determining the quality of life among the elderly (Sahoo et al., 2023). The following literature review explores key findings from existing research on the economic security and vulnerabilities of ageing populations globally.
In high-income countries, extensive research has documented the challenges and needs associated with ageing, emphasising the role of robust social security systems in safeguarding the economic well-being of older adults (Foster & Walker, 2015). Studies suggest that countries with comprehensive pension systems, universal healthcare, and well-developed welfare policies are better positioned to provide economic security for the elderly. For example, Bloom et al. (2015b) found that countries with strong social security frameworks report higher life satisfaction and lower levels of poverty among the elderly. These findings highlight the critical role of government support systems in mitigating the financial and social vulnerabilities associated with ageing.
On the other hand, in developing countries, the elderly often rely on family support and limited social welfare, as formal pension coverage is minimal. Bongaarts and Zimmer (2002) highlight the reliance on family and community networks in developing nations, where the elderly typically depend on younger family members for financial and physical support. However, as urbanisation, migration, and changing family structures weaken traditional support systems, elderly individuals increasingly face economic insecurity. This trend has been observed across regions in Asia, Latin America, and sub-Saharan Africa, where the formal safety nets for ageing populations are inadequate to meet growing needs (Bastia et al., 2022; Gangopadhyay, 2024; Higo & Khan, 2015; Kakwani & Subbarao, 2007).
When we look at India's case, the demographic transition is creating an unprecedented demand for economic and social support systems tailored to an ageing population. The percentage of elderly individuals in India's population has grown significantly, leading to increased concerns about their economic security (Agarwal et al., 2020). While family support remains the primary source of security for many, the decline of the joint family system due to urban migration and employment shifts has disrupted this traditional safety net (Lena et al., 2009). Moreover, income insecurity, inadequate healthcare access, and limited social security exacerbate vulnerabilities among the elderly.
Sahoo et al. (2023) argue that a healthcare financing model centred on progressive taxation and extensive prepayment coverage constitutes an effective approach to ensuring the long-term sustainability of the health system. A study by Alam and Karan (2010) found that only 10% of India's elderly receive pensions from formal employment, while the vast majority are left without regular income support. This lack of formal pension coverage is primarily due to India's extensive informal labour sector, which accounts for over 90% of employment and offers limited benefits (ILO, 2018). Consequently, many elderly individuals rely on informal sources of income, savings, or family support, leaving them vulnerable to poverty, especially in the event of illness or financial crises. Irshad and Dash (2022) found that elderly individuals in the lowest wealth quintiles were more vulnerable to health deterioration due to short-term morbidity, whereas those in the highest wealth quintiles were more likely to experience long-term and multi-morbidity, providing evidence for the ‘disease of affluence’. Moreover, social capital, particularly co-residence in a joint family, played a crucial role in mitigating health risks and enhancing overall well-being.
Health insecurity is another component of economic vulnerability among India's elderly. Ageing populations experience higher healthcare needs, yet access to affordable healthcare remains limited, particularly for low-income individuals. Research by Rajan et al. (2020) emphasises the challenges that the elderly face in accessing healthcare, noting that out-of-pocket expenses account for a significant proportion of their income. For instance, a large segment of India's elderly population lacks health insurance, and state-provided healthcare facilities are often inadequate, particularly in rural areas (Chatterjee & Srinivasan, 2013). These healthcare challenges are further compounded by gender disparities. Studies indicate that elderly women are more vulnerable to economic and health insecurities than men, primarily due to lower lifetime earnings, limited asset ownership, and a greater likelihood of living alone (Kalavar & Jamuna, 2011). As a result, elderly women are at a higher risk of falling into poverty, particularly those without family support or financial resources.
The social context also plays a significant role in shaping economic security for India's elderly population. Socioeconomic factors such as education, income, and employment history influence the financial resilience of older adults (Bloom et al., 2010). Studies show that individuals with lower educational attainment and those who have worked in informal or low-wage occupations are more likely to experience poverty in old age (Bloom et al., 2015a). Educational disparities are particularly pronounced among India's rural elderly population, where the lack of formal employment and pensions increases reliance on children for support. Additionally, the social stigma associated with ageing and dependence can hinder elderly individuals from seeking support. A study by Das and Dhillon (2024) notes that older adults in India often hesitate to seek assistance from family members or community programs due to concerns about being perceived as a burden. This reluctance is more evident among women, who may face additional social expectations regarding financial dependence.
India's policy framework has recognised the need for elderly support through programs such as the NSAP, which provides limited financial assistance to individuals below the poverty line. However, studies argue that the reach and adequacy of such programs are insufficient to meet the needs of India's rapidly growing elderly population. For instance, Alam and Karan (2010) found that only a fraction of eligible beneficiaries receive social assistance benefits due to administrative challenges, limited resources, and poor implementation. Comparative studies show that countries such as Brazil, China, and South Africa have implemented broader social security programs that cover the majority of their elderly population, suggesting that India could benefit from adopting similar models (ILO, 2018). In particular, the expansion of healthcare coverage and the development of comprehensive pension schemes could significantly improve economic security among India's elderly.
While existing literature provides valuable insights, several research gaps remain in understanding the specific needs and vulnerabilities of India's ageing population (Bhan et al., 2017). Further research could explore the differential impact of ageing on urban versus rural populations, considering that elderly individuals in rural areas often have less access to healthcare and social support. Moreover, research should examine the potential for public–private partnerships to enhance elderly support services, as limited government resources may constrain the scalability of state-led programs.
In summary, the literature reveals that India's ageing population faces significant economic vulnerabilities due to inadequate social security, limited healthcare access, and weakening family support systems. The shift from traditional family structures and the inadequacy of formal income support mechanisms pose significant challenges for policymakers. To address these challenges, India must consider expanding social security coverage, enhancing healthcare access, and creating targeted support programs for vulnerable groups, particularly elderly women and rural populations. By implementing these policy changes, India can better address the needs of its ageing citizens, promoting economic security and well-being for this growing demographic.
Methodology
The study employs a time-series dataset spanning 38 years, from 1986 to 2023, which allows for a comprehensive analysis of both short- and long-run relationships. This period is chosen to capture significant economic and policy developments in India, including structural reforms initiated in the early 1990s, the expansion of pension schemes, and increasing public investment in social sectors. The extended timeframe ensures sufficient data variability and structural shifts necessary for the robust application of the ARDL approach, thereby enhancing the validity of the empirical analysis. The data is sourced from government databases such as the Reserve Bank of India, the Ministry of Statistics and Programme Implementation, and relevant international organisations.
The Dependent Variable is the Life expectancy of the ageing population (aged 60 and above). The dependent variable, Life Expectancy of the Ageing Population, is operationalised as the average number of years a person aged 60 and above is expected to live, as reported by official demographic sources such as the Government of India statistical reports. The independent variables are state development expenditure (SDE) – Investments made by state governments in development sectors; central development expenditure (CDE) – Development spending at the national level; and PE – Financial allocations to old-age pensions. All variables are converted to log values for the analysis.
Among the independent variables, SDE is measured as the total annual expenditure incurred by state governments on development activities, including health care, education, infrastructure, and social welfare programs, sourced from government budget reports and state financial statements. The CDE is defined as the total annual development spending by the central government, allocated toward health schemes, education programs, and other economic development initiatives, based on the Union Budget and government financial statistics. Another independent variable, PE, is measured as the total annual government expenditure allocated to old-age pension schemes at both the state and central levels, including direct transfers and social security payments for elderly individuals, as reported in government finance records and policy documents. These operational definitions ensure that the variables accurately reflect government fiscal actions targeted toward development and elderly welfare, enabling empirical analysis of their impact on the life expectancy of older adults in India.
The study investigates the impact of SDE, CDE, and PE on the life expectancy of the ageing population in India using the ARDL model. The ARDL approach is chosen due to its flexibility in accommodating variables with mixed integration orders I (0) and I (1) and its ability to estimate both short-term and long-term relationships within a single framework (Pesaran et al., 2001). However, the critical bounds values provided by Pesaran et al. (2001) for the ARDL bounds testing procedure are no longer valid in the presence of variables integrated of order two, i.e., I(2). Therefore, it becomes essential to conduct unit root tests prior to the application of the ARDL approach in order to ensure that none of the variables are integrated beyond the first difference (Narayan, 2005). Accordingly, the present study employed the augmented Dickey–Fuller (ADF) test and the Phillips–Perron (PP) test to examine the order of integration of the variables. The relationship is expressed as follows:

The ARDL model is estimated to capture the relationship between life expectancy and its determinants. The model is specified as follows:

The ARDL model is used here for several other reasons as well. The ARDL model is a versatile and widely used econometric tool for analysing the relationship between variables, particularly in time series data. One of the ARDL model's most significant advantages is its ability to handle variables of mixed integration orders, i.e., I(0) (stationary at levels) and I(1) (stationary at first difference). Unlike traditional cointegration methods such as the Johansen or Engle-Granger approaches, the ARDL model does not require all variables to be of the same order of integration (Nkoro & Uko, 2016). The ARDL model simultaneously estimates short-term dynamics and long-term equilibrium relationships. Moreover, the ARDL model is particularly effective when working with small sample sizes, offering robust and reliable estimates compared to alternative techniques (Ghatak & Siddiki, 2001). Furthermore, the ARDL model incorporates lagged values of dependent and independent variables, providing a framework to explore dynamic interaction among variables (Sari et al., 2008). In the current study, variables exhibit mixed integration properties due to differing statistical behaviours and trends. The ARDL model addresses this issue by accommodating I(0) and I(1) variables, making it indispensable for studies involving economic, financial, or social data (Menegaki, 2019; Nkoro & Uko, 2016; Pesaran et al., 2001; Yorucu & Mehmet, 2015). Table 1 shows the descriptive statistics of the variables considered for the study.
Descriptive Statistics of the Variables.
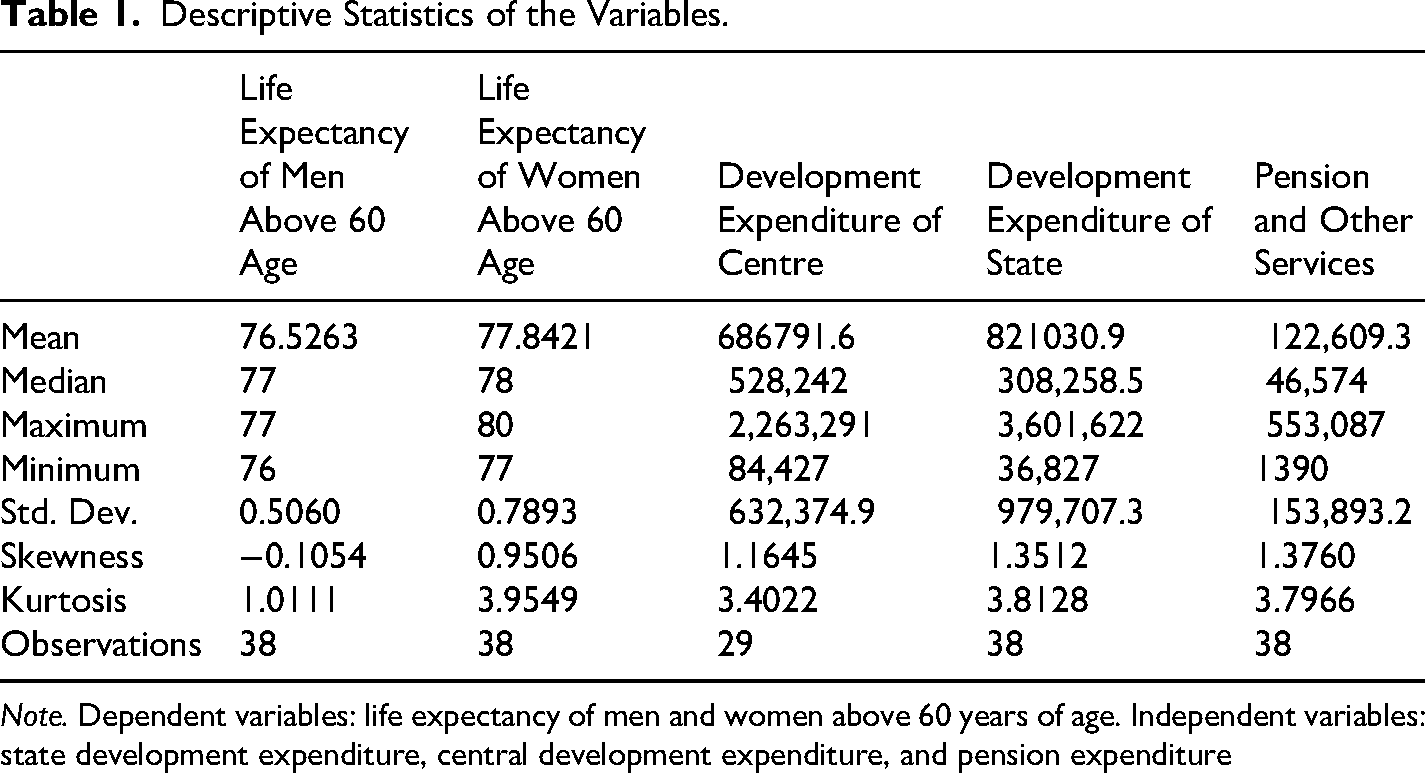
Note. Dependent variables: life expectancy of men and women above 60 years of age. Independent variables: state development expenditure, central development expenditure, and pension expenditure
Results and Findings
As a preliminary step for applying the ARDL model, the stationarity properties of the variables were examined using the ADF test and the PP test. The results are presented in Table 2. Overall, the results indicate that the variables are integrated of mixed order, I(0) for some variables and I(1) for others. Since none of the variables is integrated of order two, i.e., I(2), the ARDL approach is appropriate to investigate the existence of a relationship among the variables (Pesaran et al., 2001).
Unit Root Test Results Using ADF and Phillips–Perron.
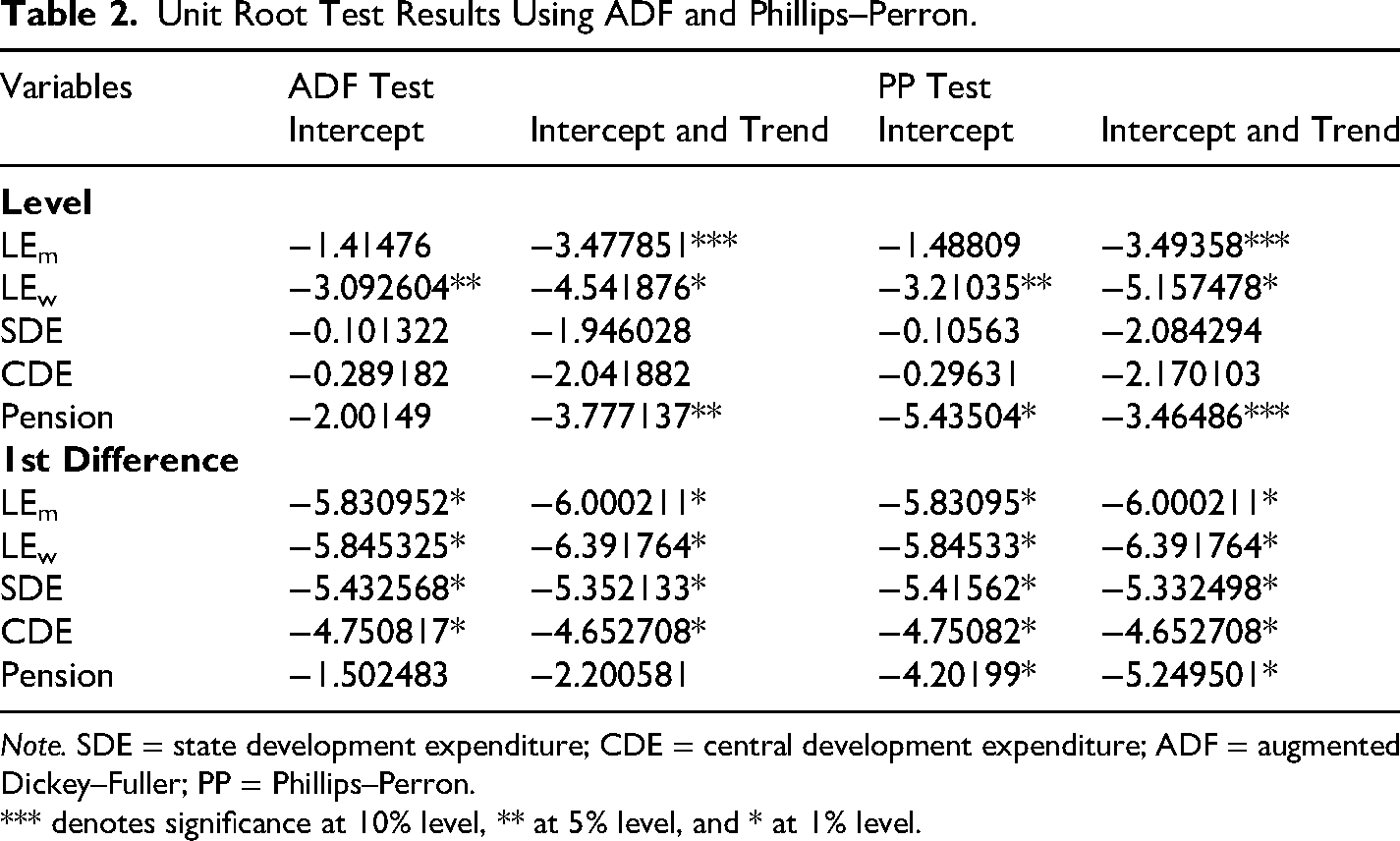
Note. SDE = state development expenditure; CDE = central development expenditure; ADF = augmented Dickey–Fuller; PP = Phillips–Perron.
*** denotes significance at 10% level, ** at 5% level, and * at 1% level.
The ARDL estimation results in Table 3 provide insights into the relationship between the life expectancy of men and the independent variables: SDE, central development expenditure, and PE. The model is specified with lagged terms of the dependent and independent variables, allowing us to capture both short-term and long-term dynamics. From Table 3, the coefficients of the lagged dependent variable terms indicate the dynamic nature of life expectancy of men above 60 years of age. The coefficient of life expectancy of men at first lag is positive (0.690) and significant, suggesting that previous life expectancy levels positively influence current levels. The coefficient of life expectancy of men at the second lag is negative (−0.580) and significant, indicating a correction mechanism in the dynamic process, where deviations from prior periods adjust over time. These results highlight a mixed but significant dynamic adjustment process of life expectancy.
Results of ARDL (2,4,3,2) with Life Expectancy of Men Above 60 Years of Age as the Dependent Variable.
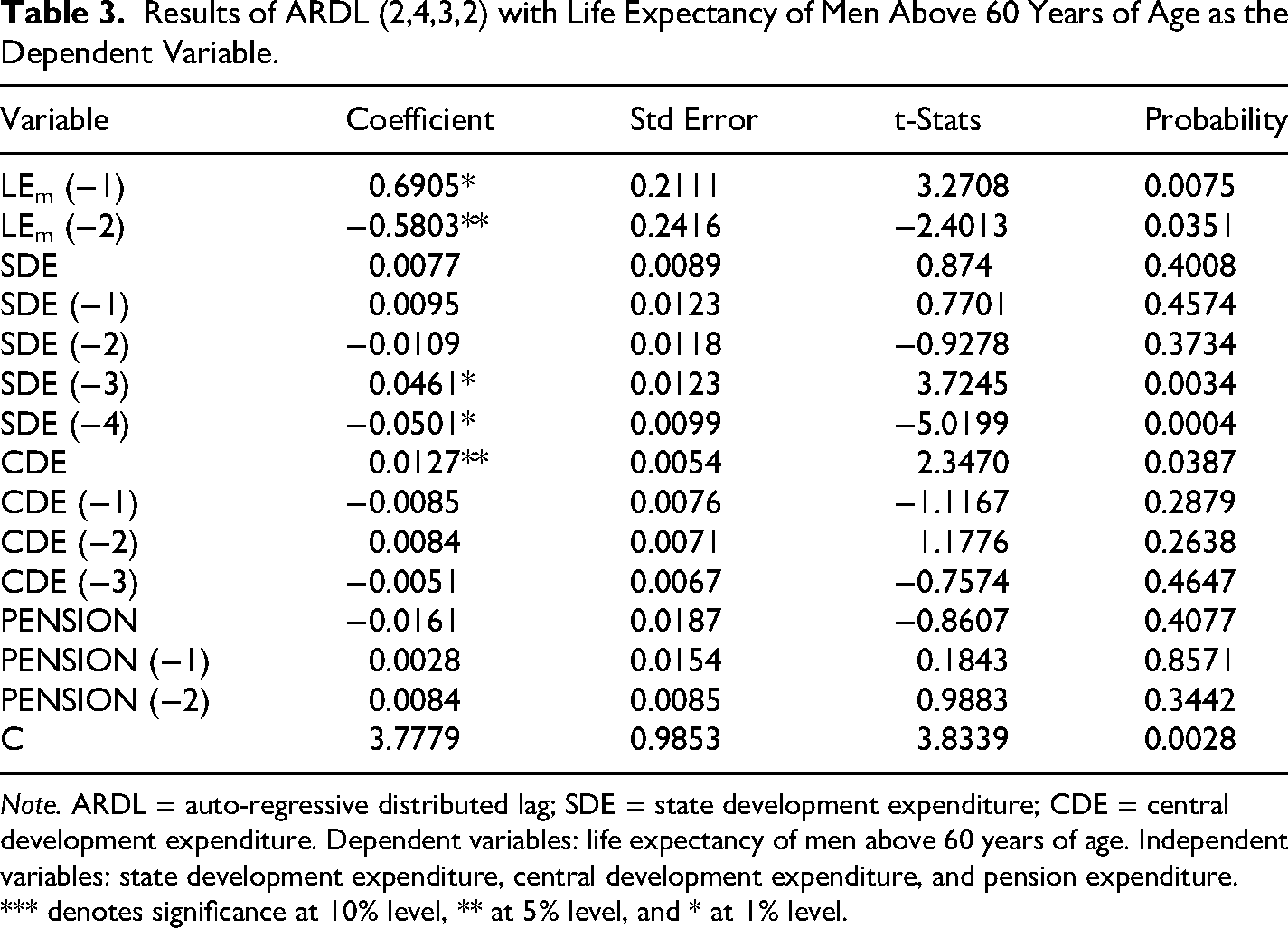
Note. ARDL = auto-regressive distributed lag; SDE = state development expenditure; CDE = central development expenditure. Dependent variables: life expectancy of men above 60 years of age. Independent variables: state development expenditure, central development expenditure, and pension expenditure.
*** denotes significance at 10% level, ** at 5% level, and * at 1% level.
The independent variables reported in Table 3 reveal important relationships between public expenditure and life expectancy among men. The coefficient for current SDE is positive (0.007) but statistically insignificant. In contrast, the third lag of SDE shows a large positive and significant effect, indicating that investments in state-level development improve life expectancy after approximately 3 years. However, the fourth lag has a significant negative coefficient, suggesting diminishing returns or possible inefficiencies over time. These findings highlight the lagged and non-linear nature of SDE, where benefits emerge in the medium term but may weaken or reverse over longer periods.
In the case of central development expenditure, it has a positive and significant effect, showing an immediate positive impact of central development expenditure on life expectancy. However, the lagged coefficients are statistically insignificant, suggesting that the positive effects of central expenditure are largely short term and do not persist across subsequent years. Overall, the findings indicate that central development expenditure contributes to improvements in life expectancy primarily in the immediate period.
When it comes to PE, the coefficients for pension and its lags are statistically insignificant, with p-values well above .05. This suggests that PE does not have a measurable direct impact on the life expectancy of men within the studied time frame. This could be due to inefficiencies in pension systems or the fact that other factors, such as healthcare spending, may play a more direct role in influencing life expectancy.
The ARDL analysis demonstrates that both state and central development expenditures influence male life expectancy, although their effects vary across time. These findings are consistent with earlier studies that reported a positive association between public expenditure and health outcomes (Bloom et al., 2004; Sahoo et al., 2023; Subramanian & Kawachi, 2004; Vogt & Kluge, 2015). While central development expenditure generates an immediate effect, SDE produces more substantial medium-term effects. PE, however, appears to have limited influence within the scope of the model. This result aligns with previous studies that questioned the effectiveness of social pension policies in significantly improving the lives of older adults (Pal & Palacios, 2011). The findings therefore suggest that policymakers should maintain a balanced approach to development expenditure at both the state and central levels, while also addressing inefficiencies within pension systems.
For women above 60 years of age, the coefficients of the lagged dependent variable terms reveal the dynamic adjustments in life expectancy. Table 4 presents the ARDL results with female life expectancy as the dependent variable. The third lag of life expectancy has a negative and statistically significant coefficient (−0.462). In contrast, the remaining lagged coefficients are statistically insignificant. Although most lagged terms are not strongly significant, their negative signs suggest that past deviations in life expectancy may adversely influence current outcomes, even if the effect is small.
Results of ARDL (3,4,4,3) with Life Expectancy of Women Above 60 Years of Age as the Dependent variable.
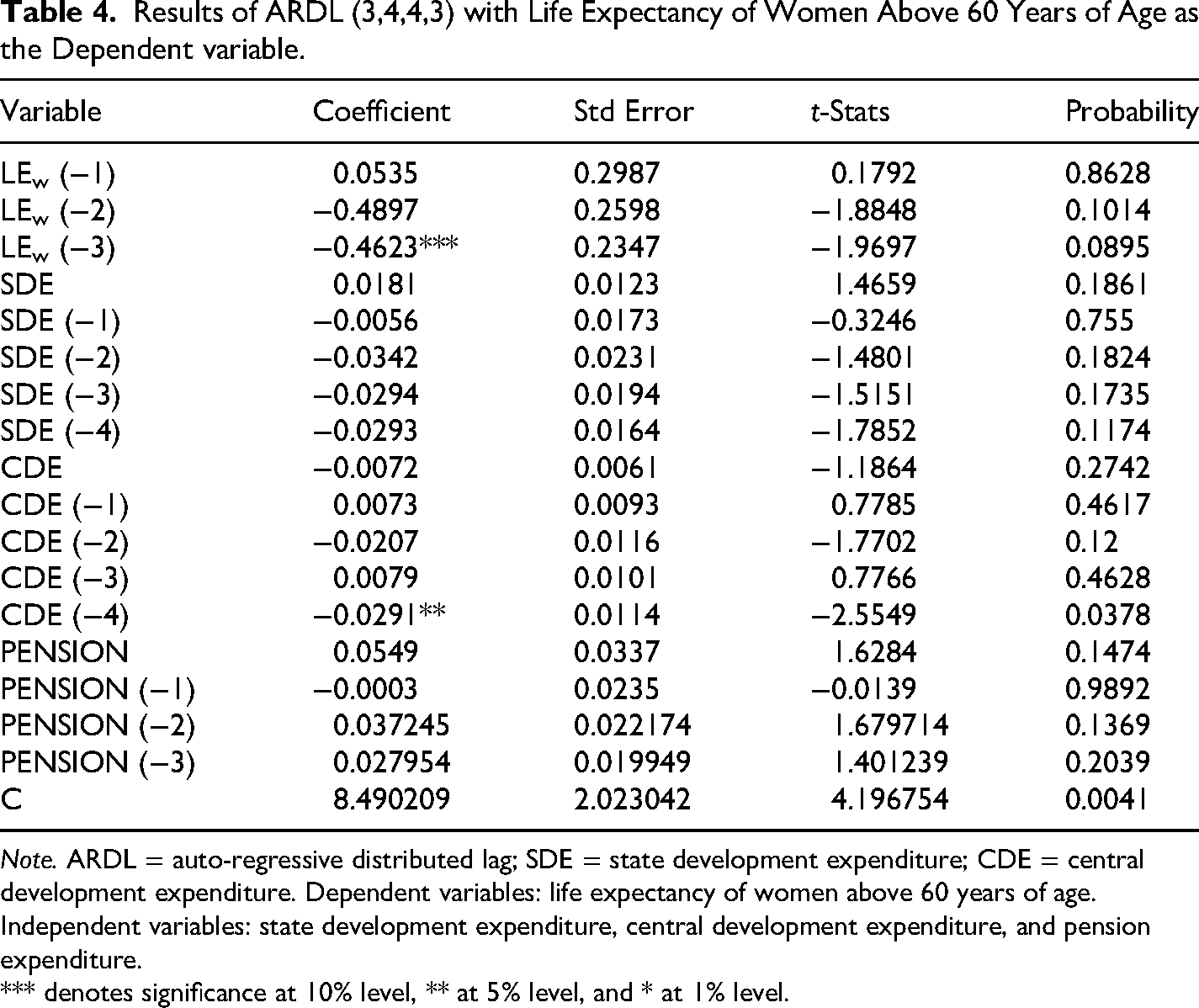
Note. ARDL = auto-regressive distributed lag; SDE = state development expenditure; CDE = central development expenditure. Dependent variables: life expectancy of women above 60 years of age. Independent variables: state development expenditure, central development expenditure, and pension expenditure.
*** denotes significance at 10% level, ** at 5% level, and * at 1% level.
The coefficients of SDE and its lags suggest nuanced impacts on the life expectancy of women. The current period coefficient (0.018) is positive but insignificant, with no effect on the dependent variable. All lagged terms (up to four periods) are negative, but none are statistically significant. These results imply that SDE does not contribute, reflecting inefficiencies or delays in the realisation of benefits.
The relationship between central development expenditure and women's life expectancy presents mixed outcomes. The current period coefficient is negative but statistically insignificant, indicating no immediate impact. Among the lagged terms, the fourth lag of central development expenditure has a negative and statistically significant coefficient (−0.029). This finding suggests that central expenditure may exert a delayed adverse effect on life expectancy, potentially due to inefficiencies in allocation, implementation delays, or ineffective targeting of resources. The significance of the fourth lag further indicates that the effects of central policies and investments emerge only after a considerable time period and may not always generate favourable outcomes.
The coefficients of PE reported in Table 4 indicate limited direct effects on life expectancy of women. Lagged terms are also insignificant, though pension (−2) shows a near-significant positive impact, suggesting delayed benefits from pensions. The lack of strong significance for PE may indicate inefficiencies in pension delivery or its indirect role in life expectancy.
The findings of the ARDL model for the determinants of life expectancy in women reveal several nuanced relationships, each with potential underlying causes. The weak dependence of life expectancy on its own lagged values suggests that short-term variations are not strongly driven by recent trends. Instead, life expectancy appears to depend more on long-term structural and demographic factors (Bloom, Canning & Sevilla, 2004). The near-significant negative coefficients of the second and third lags may indicate an adjustment process in which earlier deviations in life expectancy are gradually corrected over time. This stabilising mechanism may be influenced by long-term healthcare policies and demographic transitions (Vogt & Kluge, 2015).
SDE demonstrates inconsistent effects, with a positive but insignificant current coefficient and negative lagged coefficients. These results may reflect delays or inefficiencies in converting state-level expenditure into measurable health improvements for women. Although development expenditure has the potential to improve healthcare access and socioeconomic conditions (Subramanian & Kawachi, 2004), the negative lagged effects may arise from inefficient allocation, misaligned policy priorities, or diminishing returns from sustained expenditure. Gender disparities within pension systems and social welfare policies may also reduce the effectiveness of such investments for women. Women often receive lower pension benefits and face structural barriers that limit their ability to convert financial support into improved health outcomes (Alvarez et al., 2021; Ginn & Foster, 2023). Furthermore, long-term investments may fail to adequately address gender-specific healthcare requirements, such as women-centred health infrastructure and support services, which remain underprioritised in broader development programmes. These structural limitations may explain the negative lagged effects of SDE on women's life expectancy.
The mixed results for central development expenditure further underscore the complexities of resource allocation. The immediate effect is insignificant, and the fourth lag shows a significant negative coefficient, possibly indicating delayed inefficiencies. This may indicate delayed inefficiencies arising from bureaucratic constraints, implementation delays, or mismanagement of funds. It is also possible that the benefits of central expenditure are unevenly distributed across regions, thereby failing to address localised health and social challenges affecting women's life expectancy.
PE shows weak but mostly positive coefficients, hinting at delayed benefits. Pensions may indirectly improve life expectancy by enhancing financial security among older women, thereby improving access to healthcare and reducing financial stress. However, the lack of statistically significant results may reflect structural weaknesses within the pension system, including inadequate coverage, insufficient benefit levels, and delays in disbursement, all of which reduce the effectiveness of pension support on health outcomes (Bloom & McKinnon, 2014; Holzmann, 2013). Overall, the findings emphasise the importance of targeted and efficient policy interventions that address gender-specific health challenges while improving the implementation and monitoring of development and PEs.
The stability of the estimated ARDL models was assessed using the CUSUM and CUSUM of Squares tests, and the results are presented in Figure 1a and b. In Model 1, the plots of both the CUSUM and CUSUM of squares statistics remain well within the 5% significance boundaries throughout the sample period. This indicates that the estimated coefficients of the ARDL model are structurally stable over time. The absence of any significant deviation from the critical bounds confirms that there are no structural breaks or instability in the long-run and short-run dynamics of the model during the study period.
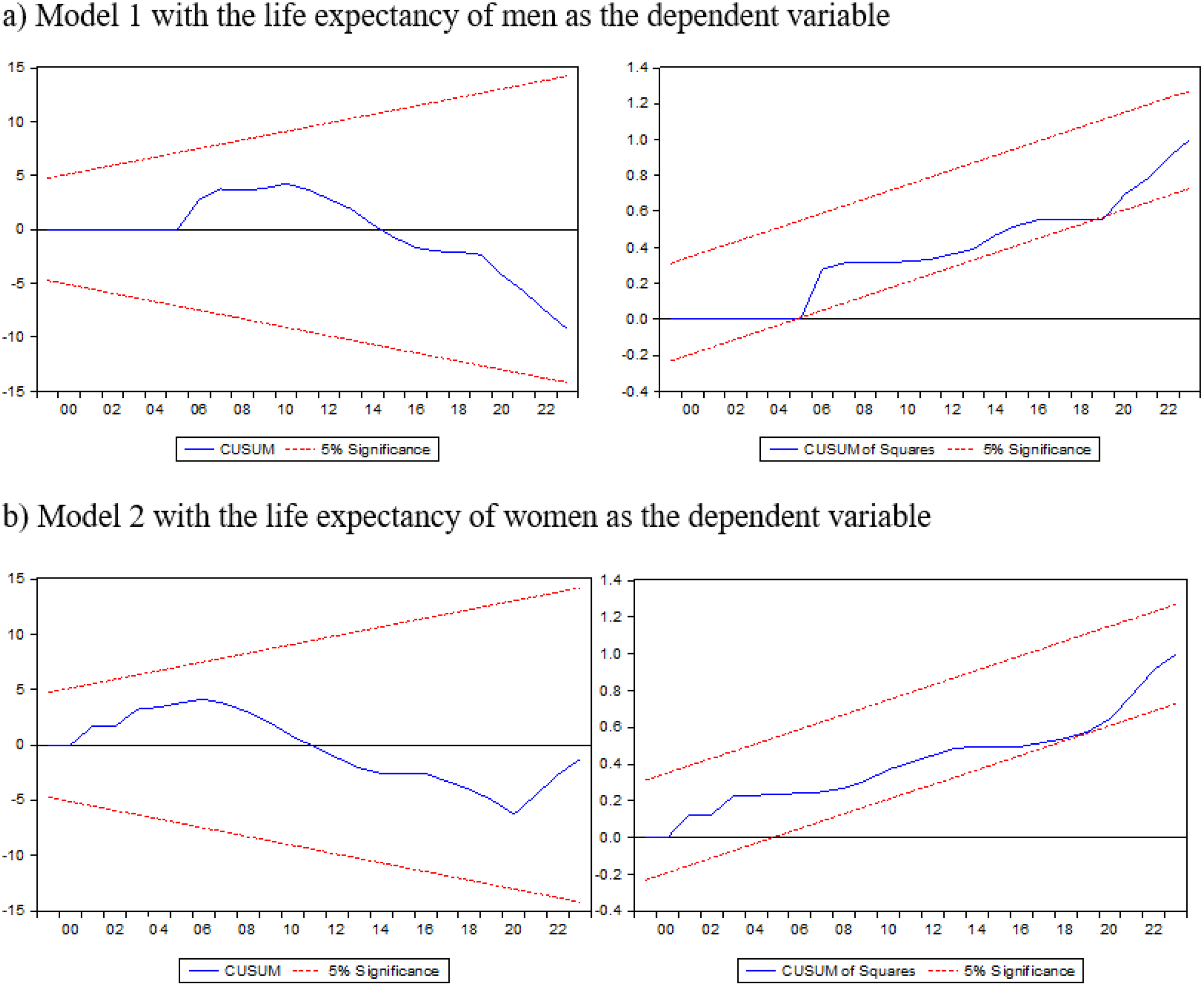
The results of CUSUM and CUSUM of squares.
Similarly, in Model 2, the CUSUM and CUSUM of squares plots also lie within the 5% confidence bands, suggesting that the estimated parameters of the ARDL model are stable across the sample period. These findings support the validity and robustness of the ARDL specification. Overall, the stability tests indicate that the relationships identified in both the male and female models remain consistent throughout the study period. This suggests that the effects of the explanatory variables on life expectancy do not change unexpectedly over time, thereby strengthening the reliability of the results across different years.
To check the possible long-run effect of independent variables on the dependent variables, an ARDL bounds test has been conducted. The results of the ARDL Bounds Test presented in Table 5 provide evidence of a long-run relationship between pension benefits and life expectancy among elderly men and women in India.
Results of Long-Run Bounds Test.
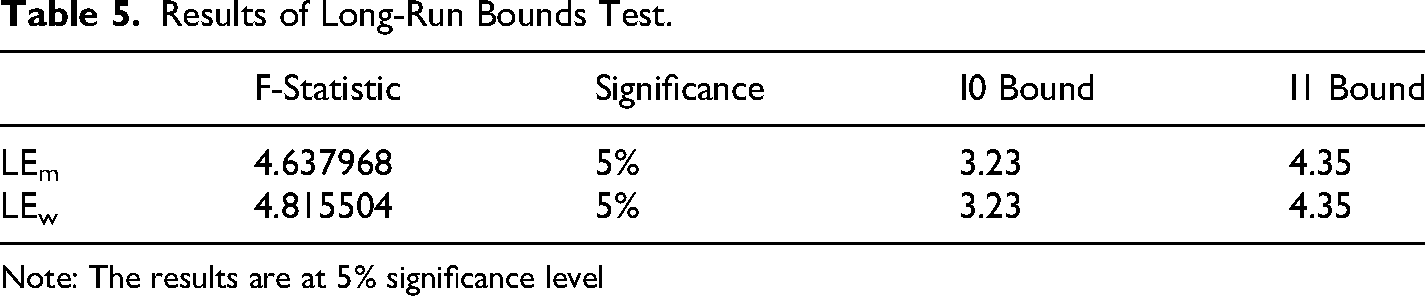
Note: The results are at 5% significance level
For the life expectancy of men, the computed F-statistic is 4.63 in Table 5, which exceeds the upper bound critical value (I1 Bound) of 4.35 at the 5% significance level. Similarly, for the life expectancy of women, the F-statistic is 4.8, which also surpasses the I1 Bound of 4.35 at the 5% significance level. Since the calculated F-statistics for both life expectancy of men and women fall above the upper bound critical values at the 5% significance level, the null hypothesis of no long-run relationship is rejected. This implies a statistically significant long-run equilibrium relationship between independent variables and life expectancy for both male and female elderly populations. The test results indicate a significant long-run relationship between public spending and the life expectancy of both elderly men and women. This means that development expenditure and pension spending have a significant influence on long-term changes in life expectancy in India.
The long-run estimates derived from the ARDL model, presented in Tables 6 and 7, provide important insights into the relationship between developmental expenditure and elderly life expectancy in India. The findings indicate that public expenditure at both the state and central levels plays a significant role in shaping long-term health outcomes among older adults, although the effects vary across gender.
The Long Form-Life Expectancy of Men as the Dependent variable.
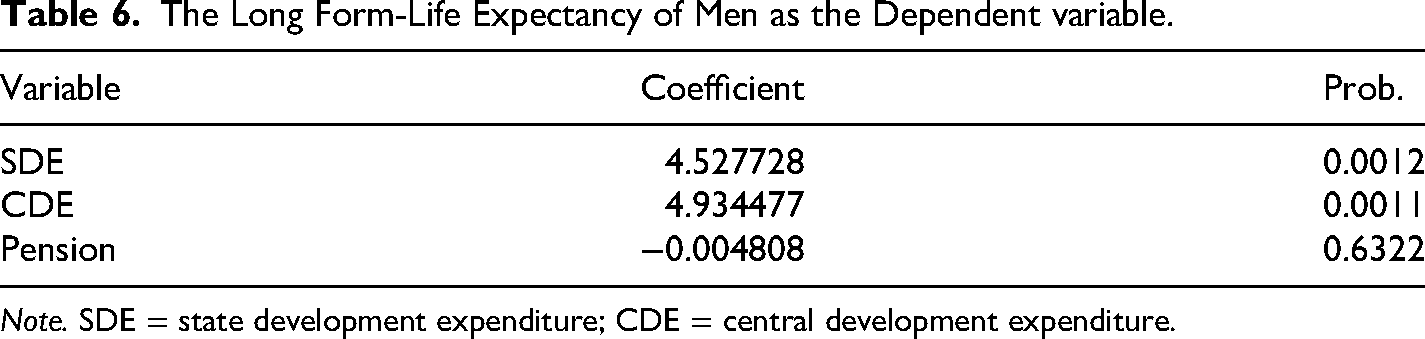
Note. SDE = state development expenditure; CDE = central development expenditure.
The Long Form-Life Expectancy of Women as Dependent variable.
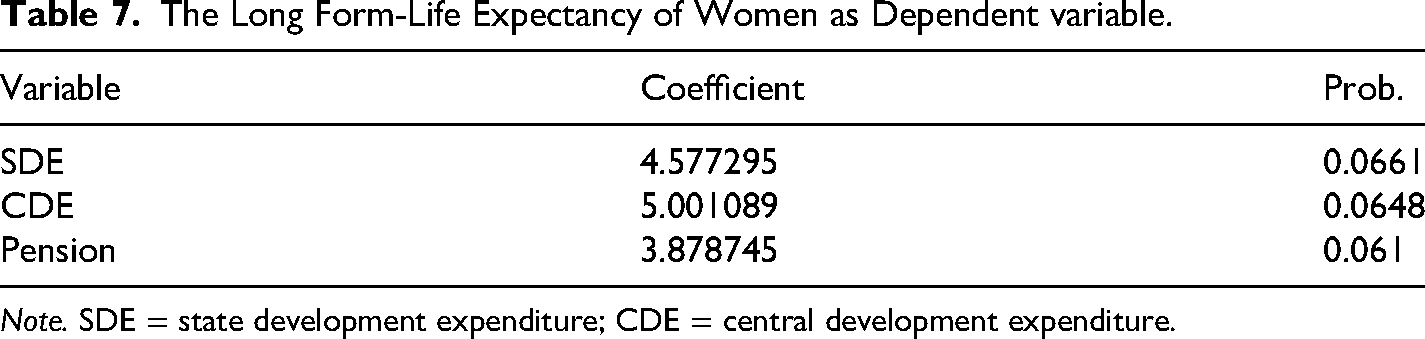
Note. SDE = state development expenditure; CDE = central development expenditure.
Table 6 shows that, for men above 60 years of age, both state and central development expenditures have strong positive and statistically significant effects at the 1% level. These findings highlight the importance of sustained public investment in developmental sectors for improving male longevity. In contrast, PE is statistically insignificant, suggesting that pension-related spending alone does not significantly influence the life expectancy of older men within the scope of the model.
The long-run estimates reported in Table 7 reveal somewhat different patterns for women above 60 years of age. Public development expenditure continues to exert a positive influence on life expectancy, although the coefficients are only marginally significant at the 10% level. This suggests that development expenditure contributes to improvements in female longevity, but the strength of the relationship is comparatively weaker than that observed for men.
Unlike the results for men, PE demonstrates a positive and marginally significant effect on women's life expectancy. This finding may reflect the greater dependence of older women on social protection mechanisms due to lower lifetime earnings, interrupted labour force participation, and longer life expectancy. The results, therefore, highlight the gendered dimensions of public policy effectiveness. While development expenditure appears beneficial for both men and women, pension support may be particularly important in improving the well-being and longevity of older women. Overall, the findings confirm the existence of a long-run relationship between public expenditure and elderly health outcomes in India. The results emphasise the importance of inclusive and sustained fiscal policies aimed at promoting healthy ageing within India's evolving demographic context.
The gender disparities observed in the effects of public development and PEs on women's life expectancy can be better understood through broader theoretical perspectives related to welfare regimes, social protection, and feminist economics. From a welfare perspective, India's social provisioning system is characterised by uneven coverage, decentralised implementation, and a continued reliance on household-based caregiving. These structural features often limit the equitable distribution of welfare benefits and disproportionately disadvantage women (Bloom et al., 2010; Jha, 2014).
In addition, programme design limitations, rigid eligibility criteria, and administrative bottlenecks frequently reduce women's effective access to old-age security measures. As a result, the potential health-enhancing benefits of these policies may not be fully realised among older women (Holzmann & Jørgensen, 2001; Vera-Sanso, 2010). Feminist economics explains that gender inequalities accumulate throughout the life course. Women often face unpaid care responsibilities, weaker labour market attachment, and lower lifetime earnings. These factors reduce women's economic entitlements and bargaining power in old age (Folbre, 2006). These structural disadvantages may limit women's ability to convert public transfers and development support into improved longevity outcomes. Taken together, these theoretical perspectives suggest that the weaker or negative effects of fiscal variables on women's life expectancy are not merely statistical outcomes. Instead, they reflect deeper structural inequalities embedded in social policies and the allocation of resources.
Conclusion
In conclusion, the ARDL analysis reveals that both state and central development expenditures influence life expectancy among men, though their effects manifest differently across time lags. While central development expenditure has an immediate impact, state expenditure demonstrates significant medium-term effects. PE appears less impactful within the model's scope. These findings provide valuable insights for policymakers, suggesting the need to balance development spending at both the state and central levels while addressing inefficiencies in pension systems.
The model further highlights the complexity of factors influencing the life expectancy of women. While state and central development expenditures show delayed and sometimes adverse effects, the immediate impacts are weak or insignificant. PE exhibits a potential positive effect, though the evidence is not statistically robust. These findings emphasise the importance of improving the efficiency and implementation of development and PEs to maximise their benefits for women's health outcomes. Furthermore, the findings emphasise the need for inclusive and gender-sensitive fiscal policies that address the specific health and social needs of ageing populations.
Policies should emphasise the equitable distribution of central and state funds, prioritising underserved regions and addressing local health challenges that disproportionately affect women. While showing potential delayed benefits, pension schemes require reforms to enhance their coverage and efficiency. Expanding pension accessibility for marginalised women and ensuring timely disbursements can improve financial security, indirectly influencing health outcomes. Moreover, pension reforms should prioritise increasing the adequacy of benefits, especially for women who have lower lifetime earnings and weaker labour market attachment.
Expanding pension coverage to informal-sector workers, simplifying enrolment procedures, and reducing documentation barriers would further enhance access for older women who are often excluded from contributory schemes. Priority should be given to expanding geriatric services, improving screening and management of chronic conditions, and integrating gender-responsive interventions into public health programmes. Finally, policies aimed at improving coordination between central and state-level development spending could help ensure that resources are allocated more equitably and aligned with the specific health and social needs of ageing women. These concrete measures can help translate public expenditure into more meaningful and sustained improvements in life expectancy outcomes.
For future research, it is recommended to explore additional factors that may mediate the relationship between public expenditure and life expectancy. In particular, examining the role of healthcare quality and accessibility could provide deeper insights into how public spending translates into health outcomes for older adults. Further, investigating regional variations in policy implementation and expenditure efficiency across Indian states could help identify best practices and structural challenges that affect the effectiveness of development spending. Longitudinal micro-level studies, using individual-level data such as the LASI, would also help establish causal mechanisms between fiscal interventions and individual health outcomes. Such research will be essential to design targeted and evidence-based policies that promote healthy and economically secure ageing in India.
Footnotes
Ethical Approval
The authors declare that the research conducted in this study adheres to ethical standards.
Informed Consent
Not applicable.
Research Involving Human Participants and/or Animals
Not applicable.
Author's Contribution
This is the sole contribution of the author.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Availability of Data and Materials
Not applicable