
Abstract
This 6-month randomized controlled trial compared TEAM, a group intervention to reduce stroke risk versus a 6-month wait-list control in Black men with stroke or transient ischemic attack. The primary outcome was the change from baseline to 6 months in systolic blood pressure (SBP). There were 160 randomized, N = 78 to TEAM, N = 82 to Waitlist, mean age 61.2 (SD 9.5). Attrition was 53.1% and similar across arms. Biomarker values were extracted from health records for individuals with missed visits. Baseline SBP was 135.3 (SD 17.9). Among the entire sample, SBP was numerically but not statistically significantly reduced with no significant difference between TEAM versus Waitlist. Post-hoc analyses suggested those with elevated baseline blood pressure (BP) had significant BP reduction in the group as a whole and in TEAM. Future research might target Black men with poorly controlled BP and address barriers to engaging in risk reduction programs.
Stroke is a leading cause of death and disability worldwide, accounting for 11.6% of total global deaths and 5.7% of total disability-adjusted life years worldwide (Global Burden of Disease [GBD] 2019 Stroke Collaborators, 2021). In some communities, the burden of stroke is especially pronounced. According to the U.S. Centers for Disease Control and Prevention, African Americans are 50% more likely to have a stroke as compared to their White adult counterparts (Murphy et al., 2022). Additionally, Black men are 70% more likely to die from a stroke as compared to non-Hispanic whites (Murphy et al., 2022). Risk factors for stroke such as poorly controlled hypertension, obesity, high cholesterol and higher rates of smoking contribute to the disproportionate burden of stroke in Black men (Centers for Disease Control and Prevention [CDC], 2022). In spite of the sobering data, stroke is a condition that may be preventable, even among high-risk groups. The 2021 American Heart Association/American Stroke Association Guideline for the Prevention of Stroke in Patients with Stroke and Transient Ischemic Attack (TIA) (Kleindorfer et al., 2021) notes that risk of stroke recurrence in stroke survivors can be reduced by up to 80% through the management of stroke risk factors, including lifestyle change such as healthy diet, exercise and appropriate use of evidence-based medications such as glucose-, lipid-, and blood pressure (BP)-lowering medications.
Self-management has been defined as the strategies that individuals use to manage their health and well-being (Zhu et al., 2025). These strategies include activities accomplished by individuals to: (1) live a healthy life, (2) meet their socio-emotional and behavioral needs, (3) care for them, and (4) avoid future disease (McLean et al., 2016). Self-management has been applied to stroke recovery as outlined in a recent review of the research literature by Zhu et al. (2025). A randomized controlled trial (RCT) by Lo and colleagues (2018) showed that a nurse-led stroke self-management program based on Bandura's self-efficacy theory was associated with improved survivors’ self-efficacy, anticipated outcomes, and satisfaction with self-management behaviors (Lo et al. 2018). A self-management program by Nott and colleagues (2021) was demonstrated to enhance patients’ perceptions of occupational performance and satisfaction, with self-efficacy acting as a mediating variable for improved occupational performance. In spite of the disproportionate burden, there are relatively few post-stroke recovery approaches that have specifically focused on Black men (Cao et al., 2023). Sajatovic et al. (2018) pilot -tested a self-management program based called Targeted Management (TEAM) Intervention that was intended to enhance self-management skills among Black men who had experienced recent stroke or TIA. In pilot testing, TEAM, compared to treatment as usual (TAU) found significantly better control of BP and HDL cholesterol (Sajatovic et al., 2018).
The 2024 literature review of stroke health management interventions by Zhu et al. (2025) identified some notable gaps in the available stroke self-management evidence including limited use of telemedicine and a greater need to leverage the collaborative potential of multidisciplinary teams (including in community-based efforts) for optimal stroke recovery. A qualitative study on barriers and facilitators of stroke recovery among Black individuals (Magwood et al., 2019) identified social support, resources, and knowledge as the most salient factors associated with stroke recovery. To help address existing gaps and barriers, as well as focusing directly on the critical need for effective approaches to reduce stroke burden in Black men, a prospective RCT was conducted to compare TEAM, a nurse and patient-led remotely delivered group intervention intended to reduce stroke risk versus a 6-month wait-list control (Waitlist). We hypothesized that the RCT would replicate and extend pilot findings and that TEAM would be associated with significantly lower systolic blood pressure (SBP) and higher high-density lipoprotein (HDL) when compared to Black men in the Waitlist control group at 6-month follow-up.
Methods
Study Overview
This 6-month prospective RCT compared a novel behavioral intervention to reduce stroke risk factors in Black men versus a 6-month wait-list control (Waitlist). TEAM consisted of a five-session group format, remotely delivered self-management curriculum co-delivered by a nurse and a Black man who has had stroke or TIA and his care partner (someone who is involved in their stroke recovery care or support network). Research assessments were done at study screening, 3- month follow-up and 6-month follow-up. The primary outcome was change from baseline to 6-month follow-up in SBP, while secondary outcomes included change in diastolic BP (DBP), low-density lipoprotein (LDL), HDL, triglycerides, and glycemic control (HbA1c) for individuals with diabetes. Process factors targeted by the TEAM intervention (stroke knowledge, self-efficacy, social support), and proximal health behavior outcomes (diet, exercise, smoking, and tobacco/substance use) were also examined using standardized scales, as was participant acceptability and satisfaction using Likert scales. The project was supported by the National Institute of Nursing Research (NINR) R01NR018023. The study was approved by the local Institutional Review Board (IRB) and registered on ClinicalTrials.gov identifier: NCT04402125. Study methods have been described in greater detail elsewhere (Still et al., 2021).
Sample and Recruitment
The study enrolled 160 Black men with stroke or TIA within the past 10 years. TIA categorization was based upon the ABCD TIA score (Rothwell et al., 2005). Additional inclusion criteria included being an adult ≥18 years of age, having a Barthel Index (BI) functional status score of >40 (indicating at least some degree of functional independence) (Kasner, 2006; Mahoney & Barthel, 1965), and 3) able to participate in study procedures. To maximize generalizability of findings only those who were unable to provide informed consent and those with stroke related to sickle-cell disease were excluded. Involvement of care partners was encouraged but not required. All study participants provided informed consent. Participants were recruited using a variety of methods including outreach to clinicians at two large health systems, free or paid advertising such as Research Match, (Harris et al., 2012) querying the electronic health records (EHRs) of two health systems, use of IRB-approved advertising and in-person outreach.
Table 1 illustrates demographic and clinical characteristics of the baseline sample. Not all individuals provided data on every variable. Mean sample age was 61.2 (SD 9.5) years, and mean level of education was 14.0 (SD 2.2) years. The majority of individuals (N = 97, 63.4%) had at least some college education. Less than half (N = 69, 43.9%) were married, while the remainder were single/never married or divorced, separated, or widowed. Over one-third (N = 55, 35.3%) lived alone. All except four (2.5%) had health insurance coverage of some type. The mean REALM-SF score 6.3 (SD 1.2) suggested relatively high levels of health literacy with 62% (N = 82) of the overall sample scoring a 7 on the REALM-SF, the maximum possible score. With respect to clinical variables, the majority had stroke (N = 114, 71.3%) while a smaller proportion (N = 46, 28.7%) had TIA. Baseline SBP was 135.3 (SD 17.9) and mean DBP was 83.0 (SD 12.0). Mean BMI was 30.1 (SD 6.2) and nearly half of the sample (49.4%, N = 79) had diabetes. Of the 160 men enrolled in the study, 53 (33.1%) had care partners.
Baseline Descriptive Data on a Sample of Black Men (N = 160) With Stroke or TIA.
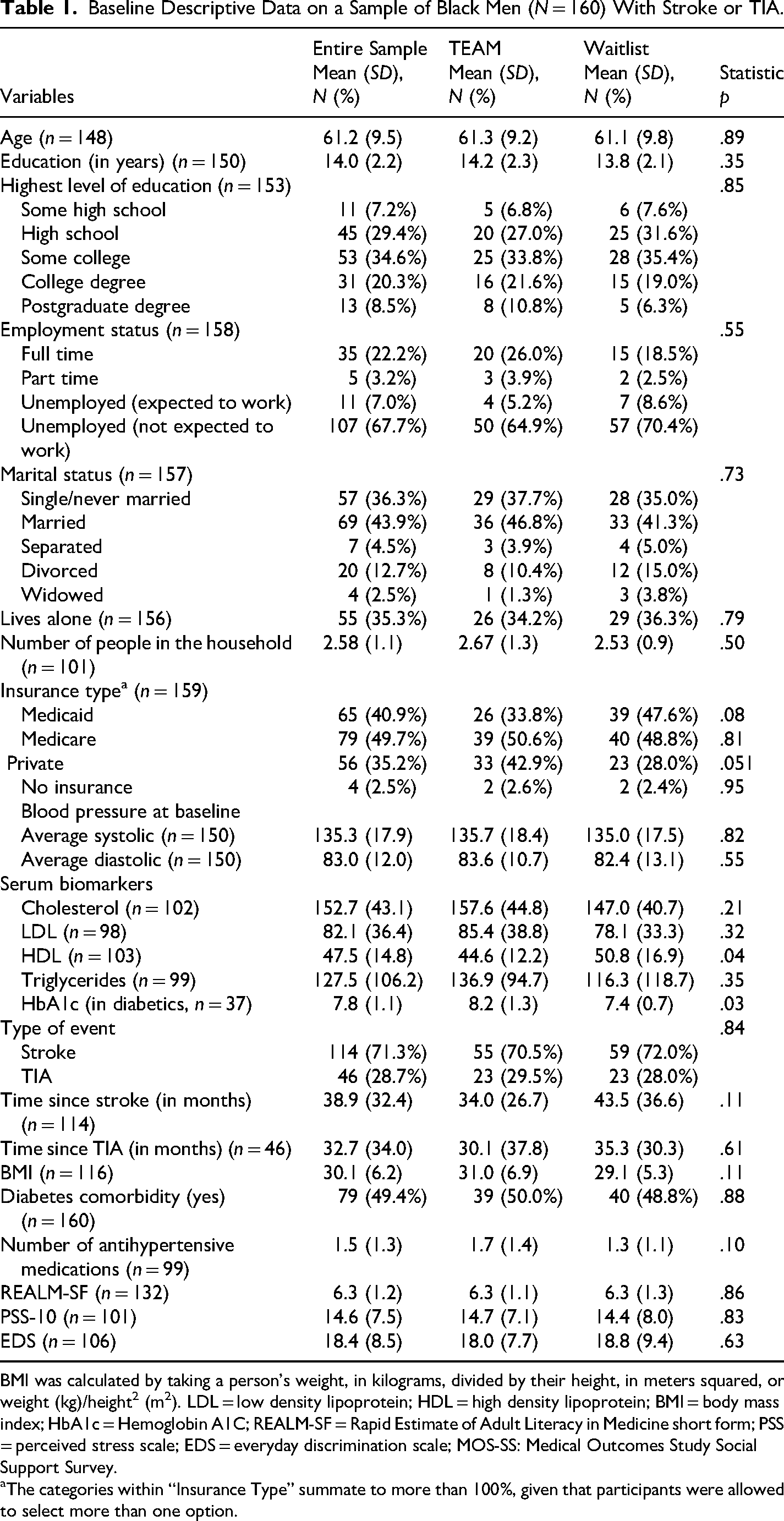
BMI was calculated by taking a person's weight, in kilograms, divided by their height, in meters squared, or weight (kg)/height2 (m2). LDL = low density lipoprotein; HDL = high density lipoprotein; BMI = body mass index; HbA1c = Hemoglobin A1C; REALM-SF = Rapid Estimate of Adult Literacy in Medicine short form; PSS = perceived stress scale; EDS = everyday discrimination scale; MOS-SS: Medical Outcomes Study Social Support Survey.
The categories within “Insurance Type” summate to more than 100%, given that participants were allowed to select more than one option.
Randomization
RCT participants were allocated on a 1:1 basis to receive either TEAM or Waitlist. Block randomization with block sizes ranging randomly between four and eight consecutive patients helped to ensure that equal numbers of TEAM and ETAU patients occurred within strata and were balanced with respect to diabetes and previous stroke.
Interventions
TEAM: TEAM is a curriculum-guided self-management approach (Sajatovic et al., 2018) which consists of an initial individual session, followed by five group sessions and six telephone follow-up sessions. TEAM sessions were delivered remotely via videoconference by a Nurse Educator and a Peer Educator Dyad (PED). The PED consisted of a Black man with experience in managing his own stroke risk and his care partner. The initial individual session was a 1:1 meeting with the PED, the participant and his care partner (if applicable). This initial session covered introductions, orientation, and logistic planning. Participants then completed five interactive group sessions involving 6–10 Black men (and their care partner if applicable) which occurred every 2 weeks. Group sessions lasted approximately 60 min. Individuals who missed a group session were encouraged to complete a make-up session conducted immediately before or after regularly scheduled groups. Individuals who were unable to participate in video calls were able to participate via standard telephone line. All participants received paper copies of the program curriculum in a format that featured graphics, handouts and a format /language that would be understandable to individuals who have experienced stroke. Following the group session series, participants had six telephone maintenance sessions, spaced approximately 2 weeks apart, with the nurse or a member of the PED. Phone sessions reinforced group session content and provided social support.
Waitlist: Individuals randomized to Waitlist participated in their regular medical care for 6 months. After 6 months, those randomized to Waitlist received the TEAM intervention as a supplement to their regular medical care. Individuals in Waitlist participated in research assessments at the same timepoints as TEAM participants.
Measures
For this primary outcome analysis, participants were evaluated at four timepoints: screening, baseline (completed immediately prior to randomization allocation), 3-month follow-up and 6-month follow-up. All data was collected and managed using an electronic data platform, REDCap (Research Electronic Data Capture) (Harris et al., 2009, 2019). Safety data was collected on spontaneously reported adverse events (AEs) and serious adverse events (SAEs) as they may have occurred during the conduct of the RCT.
Demographic variables: Age, educational level, marital status, living alone status, and insurance status were all assessed via participant self-report at study screening. We also assessed several selected contextuality variables, including health literacy, perceived stress, and discrimination.
BP: BP was assessed using an Omron 3 Model BP7100 (Omron Healthcare, 2018). As RCT enrollment began shortly before the onset of the COVID-19 pandemic, BP assessments were primarily done remotely, using home-based BP evaluation methods. All enrolled participants received a BP monitoring device and were training on its use as part of study screening procedures. Following recommendations for home-based BP evaluation (CDC, 2014). BP was assessed by having a research team member assess each participant remotely (via video conference call or phone) twice daily (morning and late afternoon/evening) for a time period of up to 7 days. Participants were asked to take two BP measurements each morning and each evening (approximately 1 min apart). The baseline BP value was calculated as an average of the series of BP readings. In situations where individuals were unable to capture BP readings using multiple home-based measurements, the baseline BP data could be obtained using either home-based reading, an in-person BP reading conducted by the study team or clinical research unit nursing staff or extracted from the electronic health record up to 8 weeks prior to or 6 weeks after the baseline time-point and up to 6 weeks before or after follow-up time points. The team prioritized home-based or in-person BP measurement capture and only used electronic health record extraction if other methods of BP evaluation were not available.
Other Stroke Risk Biomarkers
Laboratory testing for serum total cholesterol, HDL, LDL, triglycerides, and HbA1c was conducted at baseline and at 6-month follow-up timepoints. Laboratory testing was conducted using an academic medical center clinical services or national laboratory services for participants who resided outside of the regional reach of the medical center. If individuals were unable to travel to laboratory testing locations due to the COVID-19 pandemic restrictions, results were extracted from the electronic health record using similar timeframes as the BP health record data extraction. We also evaluated body mass index (BMI) as an additional stroke risk biomarker.
Self-Management Processes Outcomes
We examined selected variables and behaviors that are relevant to behavior change and that are targeted by the TEAM intervention. Stroke knowledge was measured with the Stroke Knowledge Test (SKT) (Ellis, 2014; Sullivan & Dutton, 2004) to examine knowledge of key stroke risk factors and stroke prevention practices. The SKT is scored on a continuum of 0 to 5, where higher scores indicate more stroke knowledge. Self-efficacy was measured with the General Self-Efficacy Scale (GSE) (Schwarzer & Jerusalem, 1995; Vauth et al., 2007). The SES is scored on a continuum of 10 to 40, where higher scores indicate higher self-efficacy. Social support was measured with the Medical Outcomes Study Social Support Survey (MOS-SS) (Hays et al., 1995). The MOS-SS is scored on a continuum of 0 to 100, where higher scores indicate more social support.
Proximal Behavioral Outcomes
Healthy behaviors targeted by the TEAM intervention and known to be important to stroke risk were assessed and included adherence with medication, diet, exercise, and avoidance of alcohol and recreational drugs. Medication-taking was assessed in two ways: (1) whether individuals were taking indicated stroke risk-reduction drugs (anticoagulants, antiplatelet agents, antihypertensive drugs, lipid-lowering drugs and drugs for diabetes); and (2) self-reported medication adherence using the Tablets Routine Questionnaire (TRQ) (Scott & Pope, 2002). The TRQ is scored on a continuum of 0 to 100 where higher scores indicate a greater percentage of missed medications (worse adherence). Exercise was assessed with the Morgenstern Physical Activity Questionnaire (MPAQ) (Rubenstein et al., 2011). The MPAQ is scored where higher scores indicate greater physical activity in kcal/kg/week. Smoking was assessed with the Fagerström Test for Nicotine Dependence (FND) (Fagerstrom, 1978). The FND is scored on a continuum of 0 to 10 where higher scores indicate greater dependence on nicotine. Usage of alcohol and other recreational drugs was assessed with the Modified Alcohol, Smoking, and Substance Involvement Screening Test (ASSIST) (NIDA, 2017). The ASSIST (Tobacco) is scored on a continuum of 0 to 31 where higher scores indicate greater involvement with a given drug and the need for more intensive treatment. The ASSIST (Alcohol and Cannabis) is scored on a continuum of 0 to 39 where higher scores indicate greater involvement with a given drug and the need for more intensive treatment. Diet in the past 3 days was assessed using the Nutrition Data System for Research (NDSR) (Conway et al., 2004), a Windows-based nutritional analysis software program specifically designed for collecting and analyzing 24-h dietary recalls. The NDSR is scored on a continuum of 0 to 100 where higher scores indicate a diet that better aligns with key dietary guidelines and recommendations. NDSR assessments were done at baseline and at 6-month follow-up.
Participant Acceptability and Satisfaction
Participants randomized to receive the TEAM group completed a brief participant satisfaction evaluation after the conclusion of the TEAM group sessions that covered seven domains: whether they perceived TEAM to be useful, whether the TEAM intervention covered important areas generally, whether the TEAM intervention covered important areas to them personally, whether the benefit of TEAM exceeded the burden, whether they would recommend TEAM to someone else who had a stroke/TIA and two questions regarding the appropriate number of sessions in TEAM and the appropriate duration of TEAM sessions.
Data Analysis
Descriptive statistics included examining means, standard deviation, and testing for normality using skewness and kurtosis. Statistical analyses were performed using SPSS 30.0 and SAS 9.4. Analyses were performed for the intention-to-treat population (all RCT participants enrolled; N = 160). Independent samples t-tests and chi-square statistics were used to compare group (TEAM vs Waitlist) differences for demographic and patient characteristics. The primary outcome analysis compared TEAM versus Waitlist control groups at 6 months (2 group × 3 timepoints repeated measures linear mixed models) on the primary outcome of SBP. Repeated measures mixed models were used to assess the main effect of changes over time, the interaction of the trend in the means over time by group differences, and the main effect of between-group differences. Mixed models used Full Information Maximum Likelihood (FIML) to handle incomplete data. Because the repeated measures mixed model approach was used, at least two time points of data were needed to conduct analyses. Any combination of ≥2 time points was acceptable. Data were not included in the analyses if ≥2 timepoints were missing.
We similarly evaluated TEAM versus Waitlist on change from baseline to 6 months follow-up on secondary outcomes and process measures. In addition, given missing data challenges in conducting this RCT during the COVID pandemic, we conducted a sensitivity analysis to identify demographic and clinical variables that were significantly different between RCT participants who had ≤ 1 time points of SBP data research assessments versus those who had BP data with ≥2 or more time points. Specifically, independent samples t-tests and chi-square statistics were used in sensitivity analyses to compare data that were included versus not included in the primary SBP mixed model analyses across demographic and patient characteristics. A two-sided Type I error rate of 5% was used for all tests. Post-hoc tests used Tukey-Kramer p value adjustment for type 1 error.
Results
Study Enrollment and Flow
Figure 1 illustrates overall study flow. There were 190 individuals screened and 160 randomized, N = 78 randomized to TEAM and N = 82 randomized to Waitlist. Six-month study attrition was 53.1% overall and similar across arms (N = 85 individuals were lost to follow-up, withdrew consent, or did not complete the 6-month follow-up visit). In the TEAM arm, four participants withdrew, 30 were LTFU, and six missed their 6-month visit (N = 40). In the Waitlist arm, one participant withdrew, one was withdrawn by staff, 31 were LTFU, and 13 missed their 6-month visit (N = 46). If available, health record data was extracted on BP and blood biomarker values for individuals who did not provide this data at the 3- and 6-month follow-up timepoints. Including extracted health record data there were a total of 121 individuals in the total analyzable BP analysis sample (see Table 2) comprising 57 men in the TEAM group (73.1% of original randomized allocation) and 64 individuals in the Waitlist sample (78.0% of original randomized allocation).

CONSORT diagram.
Distribution of TEAM group attendance.
Longitudinal Outcomes of Baseline to 6-Month Follow-Up BP and Other Biomarkers in TEAM Versus Waitlist Among Black Men With Stroke or TIA.
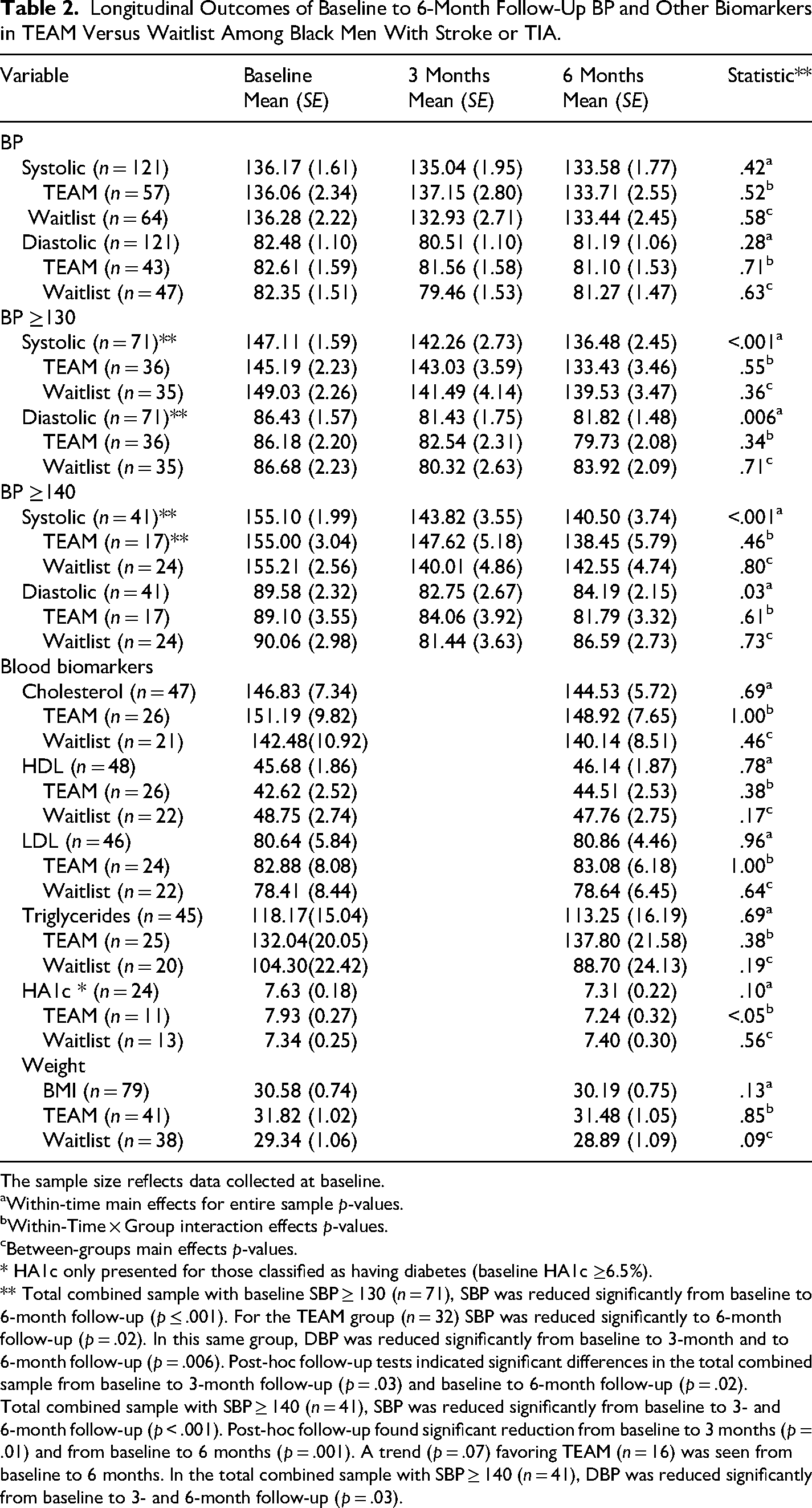
The sample size reflects data collected at baseline.
Within-time main effects for entire sample p-values.
Within-Time × Group interaction effects p-values.
Between-groups main effects p-values.
* HA1c only presented for those classified as having diabetes (baseline HA1c ≥6.5%).
** Total combined sample with baseline SBP ≥ 130 (n = 71), SBP was reduced significantly from baseline to 6-month follow-up (p ≤ .001). For the TEAM group (n = 32) SBP was reduced significantly to 6-month follow-up (p = .02). In this same group, DBP was reduced significantly from baseline to 3-month and to 6-month follow-up (p = .006). Post-hoc follow-up tests indicated significant differences in the total combined sample from baseline to 3-month follow-up (p = .03) and baseline to 6-month follow-up (p = .02).
Total combined sample with SBP ≥ 140 (n = 41), SBP was reduced significantly from baseline to 3- and 6-month follow-up (p < .001). Post-hoc follow-up found significant reduction from baseline to 3 months (p = .01) and from baseline to 6 months (p = .001). A trend (p = .07) favoring TEAM (n = 16) was seen from baseline to 6 months. In the total combined sample with SBP ≥ 140 (n = 41), DBP was reduced significantly from baseline to 3- and 6-month follow-up (p = .03).
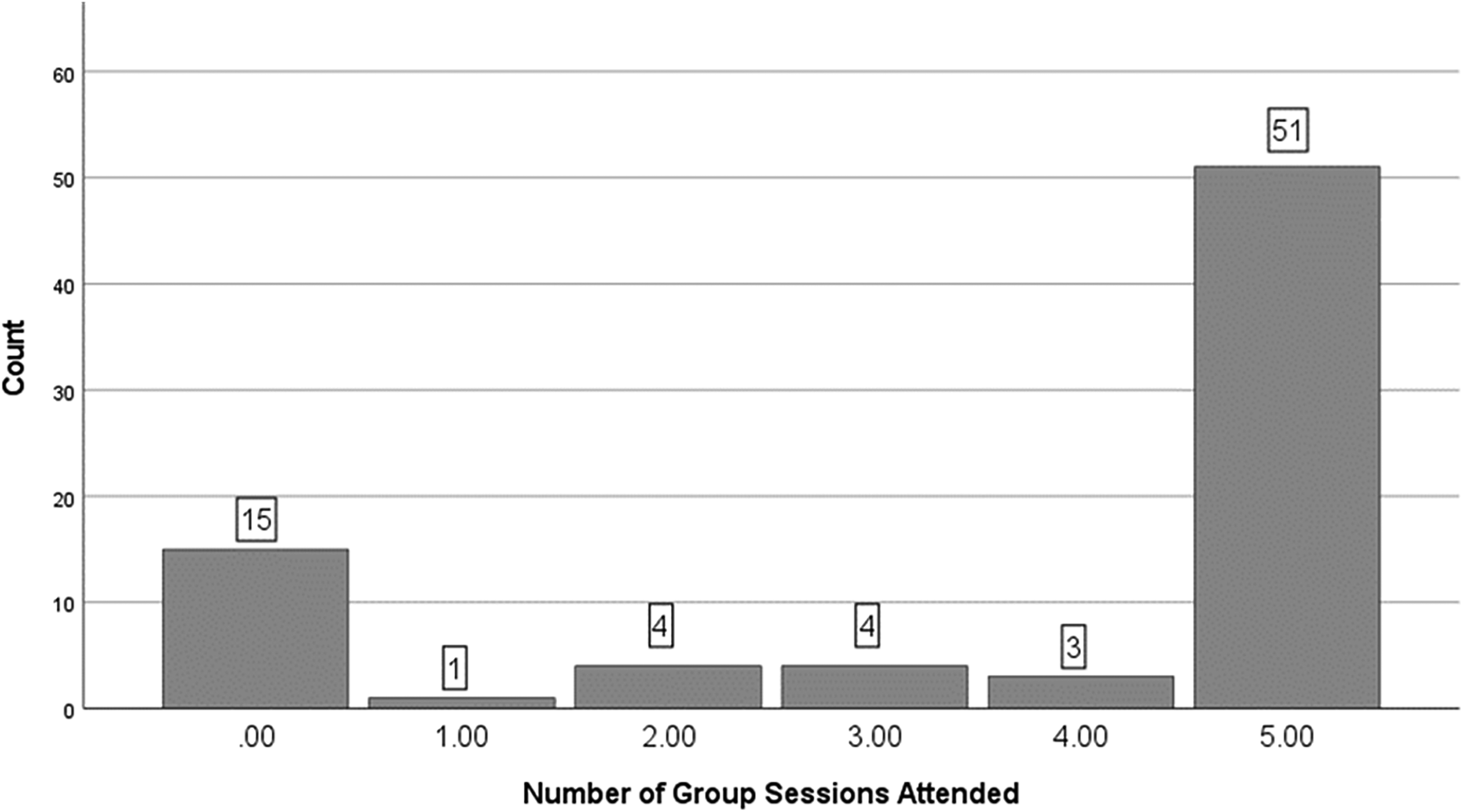
Attendance and Safety
Overall, TEAM sessions were moderately well-attended (Figure 2). In the TEAM randomized group and including makeup sessions there were 51 (65.4%) individuals who attended all five group sessions, three (3.8%) who attended four sessions, four (5.1%) who attended three sessions, four (5.1%) who attended two sessions, one (1.3%) who attended one session, and 15 (19.2%) who attended zero sessions. The mean number of attended sessions in TEAM was 3.7 (SD 2.0) sessions.
During the screening to 6-month follow-up period of the RCT, there were 27 individuals who experienced either an SAE or an AE. Some individuals had multiple AEs or SAEs. There were a total of 31 SAEs, including 22 (71.0%) due to underlying medical conditions, one (3.2%) due to psychological conditions (psychiatric or substance use problems), five (16.1%) due to combined medical and psychological conditions, and three (9.7%) where the underlying precipitant was not clear. There were no deaths in the 6-month follow-up period. There was a total of 18 AEs, including 12 (66.7%) due to underlying medical conditions, three (1.7%) due to psychological conditions (psychiatric or substance use), one (5.6%) due to combined medical and psychological conditions, and two (11.1%) where the underlying precipitant was not clear. There were no study –related AEs or SAEs as confirmed by an external data safety monitoring committee.
Primary Outcome and Key Secondary Outcomes
As noted in Table 1, we compared the sample that received the TEAM intervention (mean age 61.3 years, SD 9.2) and the sample that received the ETAU intervention (mean age 61.1 years, SD 9.8). Given the relatively high rate of missing data, sensitivity analysis was conducted to identify predictors of missing BP values. The sensitivity analysis compared those included in the primary SBP analyses (n = 121) to those who were not included (n = 39). As noted in Table 3, men with less education were more likely to be missing ≥2 time points of BP data, having a mean of 13.3 (SD 2.3) years of education versus 14.2 (SD 2.1) years of education in men with no missing BP data (p = .03). Additional predictors of missing BP data were living alone (N = 35, 29.4% for men with no missing data vs. N = 20, 54.1% missing data, p = .006) and being prescribed fewer antihypertensive medications (N = 1.6 (SD 1.4) for men with no missing data versus N = 0.8 (SD 0.8) for men with missing data, p < .001).
Sensitivity Analysis of Baseline Descriptive Data on Participants Missing BP Data at More Than One Research Visit.
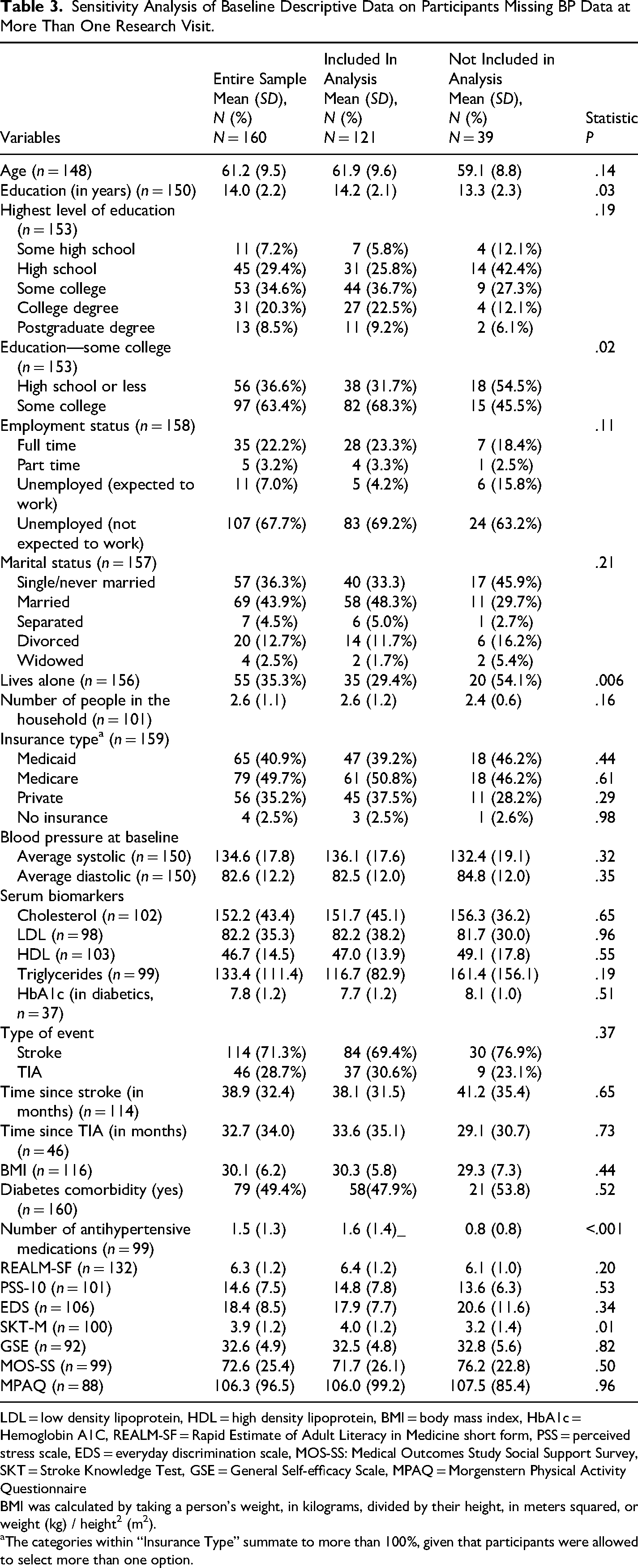
LDL = low density lipoprotein, HDL = high density lipoprotein, BMI = body mass index, HbA1c = Hemoglobin A1C, REALM-SF = Rapid Estimate of Adult Literacy in Medicine short form, PSS = perceived stress scale, EDS = everyday discrimination scale, MOS-SS: Medical Outcomes Study Social Support Survey, SKT = Stroke Knowledge Test, GSE = General Self-efficacy Scale, MPAQ = Morgenstern Physical Activity Questionnaire
BMI was calculated by taking a person's weight, in kilograms, divided by their height, in meters squared, or weight (kg) / height2 (m2).
The categories within “Insurance Type” summate to more than 100%, given that participants were allowed to select more than one option.
Table 2 shows changes in SBP and in the other biomarker changes of DBP, serum laboratory values and in BMI. As noted in the entire sample with available BP data (N = 121), SBP was numerically reduced over time from a mean of 136.2 (SE 1.61) at baseline to a mean of 133.6 (SE 1.8) at 6- month follow-up, however this difference was not statistically significant (p = .42). There was no significant difference between TEAM versus Waitlist in SBP change from baseline to 6-month follow-up.
Given the relatively good BP control at baseline and possible floor effects for change in BP over time, we also conducted post-hoc analyses examining the sub-groups of RCT participants who had elevated baseline BP using the clinically relevant SBP thresholds of 140 and of 130 (Harrison & Touyz, 2025). As noted in Table 2, in the total combined sample who had a baseline SBP ≥ 130 (n = 71), SBP was reduced significantly over time from a mean of 147.1 (SE 1.6) at baseline to a mean of 136.5 (SE 2.5) at 6-month follow-up (p ≤ .001). Post-hoc follow-up tests indicated significant differences from baseline to 6-month follow-up (p < .001). For the TEAM intervention (n = 32) there was a significant reduction in SBP over time from a mean of 145.2 (SE 2.2) at baseline to a mean of 133.4 (SE 3.5) at 6-month follow-up (p = .02). In the total combined sample of individuals who had a SBP ≥ 130, DBP was reduced significantly over time from a mean of 86.4 (SE 1.6) at baseline to a mean of 81.4 (SE 1.8) at 3-month follow-up to a mean of 81.8 (SE 1.5) at 6-month follow-up (p = .006). Post-hoc follow-up tests indicated significant differences in the total combined sample from baseline to 3-month follow-up (p = .03) and baseline to 6-month follow-up (p = .02).
In the total combined sample who had a baseline SBP ≥ 140 (n = 41), SBP was reduced significantly over time from a mean of 155.1 (SE 2.0) at baseline to a mean of 143.8 (SE 3.6) at 3-month follow-up to a mean of 140.5 (SE 3.7) at 6-month follow-up (p < .001). Post-hoc follow-up tests indicated significant differences from baseline to 3-month follow-up (p = .01) and from baseline to 6-month follow-up (p = .001). A trend in the means (p = .07) for the TEAM intervention (n = 16) was identified from baseline (mean = 155.0, SE = 3.0) to month 6 (mean = 138.5, SE = 5.8). In the total combined sample who had a SBP ≥ 140 (n = 41), DBP was reduced significantly over time from a mean of 89.6 (SE 2.3) at baseline to a mean of 82.8 (SE 2.7) at 3-month follow-up to a mean of 84.2 (SE 2.2) at 6- month follow-up (p = .03).
As noted in Table 2, there was no difference between TEAM versus Waitlist on changes from baseline to 6 months on DBP, BMI and most blood biomarkers, although it must be noted that there was considerable missing biomarker data. An exception with respect to comparison of blood biomarkers was greater change in HA1c among men with diabetes randomized to TEAM (mean of 7.9 (SE 0.3) at baseline versus mean of 7.2 (SE 0.3) at 6 months) versus Waitlist (mean of 7.3 (SE 0.3) at baseline versus mean of 7.4 (SE 0.3) at 6 months), p < .05. As with the other blood biomarkers, the sample with HA1c was small (N = 24).
Other Outcomes
Table 4 shows changes in process factors targeted by TEAM and in lifestyle factors relevant to stroke risk. Longitudinal assessment of the FTN is not included given the small sample. Longitudinal assessment of alcohol use based on risk level and cannabis use as measured by the ASSIST is not shown (and were not significant). The only significant change in the entire sample from baseline to 6 months was improvement in stroke knowledge (p = .02) There were no significant differences in TEAM versus Waitlist in change from baseline to 3 and to 6 months in any of the process factors or in life-style factors.
Longitudinal Outcomes of Baseline to 6-Month Follow-up in Self-Management Processes and Life-Style Factors in TEAM Versus Waitlist Among Black Men With Stroke or TIA.
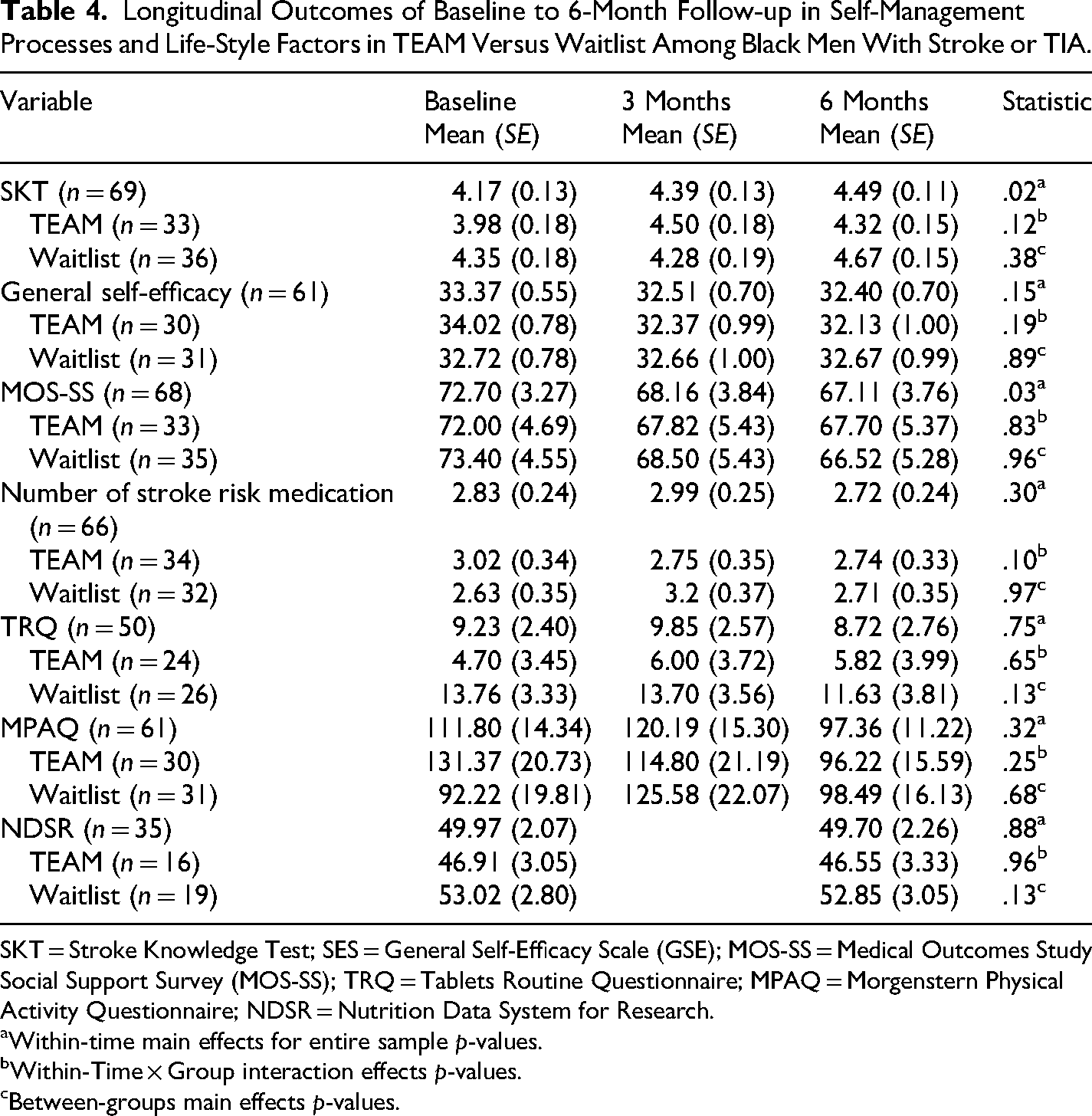
SKT = Stroke Knowledge Test; SES = General Self-Efficacy Scale (GSE); MOS-SS = Medical Outcomes Study Social Support Survey (MOS-SS); TRQ = Tablets Routine Questionnaire; MPAQ = Morgenstern Physical Activity Questionnaire; NDSR = Nutrition Data System for Research.
Within-time main effects for entire sample p-values.
Within-Time × Group interaction effects p-values.
Between-groups main effects p-values.
TEAM Intervention Participant Satisfaction
There were 27 men who completed the TEAM intervention satisfaction survey. Of these, 26 (96.3%) strongly agreed or agreed that TEAM was useful, while one (3.7%) was neutral. With respect to general comprehensiveness, and whether TEAM covered all/most of the important issues, 27 (100.0%) men strongly agreed or agreed. With respect to whether TEAM covered all/most of the issues important to the individual's particular situation, 25 (92.6%) men strongly agreed or agreed, while two (7.4%) were neutral. With respect to perceived benefit of TEAM exceeding the burden or hassle, 24 (92.3%) men strongly agreed or agreed, while two (7.7%) were neutral. With respect to whether participants would recommend TEAM to others, 26 (96.3%) men strongly agreed or agreed, while one (3.7%) was neutral. With respect to the number of sessions, one (3.7%) felt there were too many sessions, while 14 (51.9%) felt the number of sessions was just right and 12 (44.4%) felt there were too few. With respect to the length of time for each session, one (3.7%) felt the duration was too long, 23 (85.2%) felt the duration was just right, and three (11.1%) felt the duration was too short.
Discussion
A robust body of literature demonstrates extensive racial and ethnic disparities in stroke incidence, prevalence, treatment, and outcomes across the United States (Gardener et al., 2020; Harris et al., 2015; Howard et al., 2016; Ikeme et al., 2022; Jose et al., 2014). In spite of this, there are relatively limited data on how best to support and facilitate recovery for racial and ethnic communities, including Black men who have had a stroke or TIA. A recent scientific statement by the American Heart Association (AHA) (Towfighi et al., 2023) summarized the evidence for interventions to address health disparities throughout the continuum of stroke care (prehospital; acute care; rehabilitation, recovery, and reintegration; transitions in care; and secondary prevention). The AHA review suggested that stroke survivors may benefit from stroke-specific group interventions that enable social support through group encouragement, positive reinforcement and motivation, confidence boosting, and mood enhancement (Flansbjer et al., 2012; Harrington et al., 2010; Nadeau et al., 2013; Ouellette et al., 2004). However, the AHA report also noted that interventions to eliminate health disparities in stroke-related disability remain very limited (Towfighi et al., 2023).
This RCT tested the TEAM intervention, a program intended to improve a key stroke risk factor (poorly controlled BP) among Black male stroke survivors using a multi-pronged approach that featured a supportive group format, remote delivery and attention to behaviors known to heighten risk for recurrent stroke such as exercise, medication adherence, healthy diet, stress management, communication with providers and taping into available family and community resources. While this RCT did not confirm our original hypothesis that TEAM would be associated with significantly lower SBP and other key stroke risk biomarkers as an augmentation to standard medical care, there are several findings that have the potential to both inform clinical care and future research aimed at reducing stroke health disparities.
Our sample descriptive information suggests that even though Black male stroke survivors who are motivated enough to participate in a research study during the COVID pandemic have some protective social determinant of health factors, they also remain at substantial risk for ongoing cardiovascular and cardiometabolic complications. This older male RCT sample was relatively well educated with a mean of 14 years of education, nearly all had health insurance coverage (over 1/3 had private health insurance and < 3% were un-insured) and had moderately well-controlled BP at baseline with a combined total sample mean SBP of 135.3 (SD 17.9). With respect to the generalizability of the RCT sample, a 2023 Pew Research Center report (Pew Research Center, 2024) noted that about one-quarter of the U.S. Black population has a bachelor's degree or higher, slightly lower than the proportion in this RCT sample (28.8%). The U.S. Department of Health and Human Services Office of Minority Health notes that 8.9% of Black individuals have no insurance coverage (Office of Minority Health [OMH], 2024), a much higher rate than in our RCT sample. It is possible that experiencing a stroke would have allowed men in our sample to become eligible for health insurance coverage that they might not otherwise have had. For men over 60, normal serum lipid ranges target a total cholesterol <200, LDL cholesterol for high-risk individuals such as stroke survivors of <70, HD cholesterol >40, and triglycerides <150 (MedlinePlus, 2020). Our RCT sample was within optimal ranges for all of these biomarkers except for HDL where the combined sample had a mean HDL of 82.1 (SD 36.4). In spite of these favorable social determinants and biological sample characteristics, other findings suggest ongoing risk for recurrent stroke and other health complications, including high rates of obesity (mean BMI was 30.1 (6.2) and of diabetes (nearly half the RCT sample), with sub-optimal diabetes control (average HgA1c scores >7) among those with diabetes.
This RCT had a relatively high rate of attrition, with just over 53% of individuals with missed visits or lost to follow-up at the 24-week follow-up timepoint. It must be noted that the COVID pandemic started and was ongoing during the majority of this RCT and necessitated transitioning the TEAM intervention from an in-person delivery model to a remotely delivered virtual format. This telehealth format, while convenient for people with travel or social distancing restrictions, could have increased barriers to research engagement and retention among some men. It has been suggested that the COVID-19 pandemic accelerated the expansion of poststroke telerehabilitation with the potential to minimize disparities in access to care (Appleby et al., 2019). At the same time, it has also been suggested that variability in access to reliable internet and technological resources has the potential to worsen existing health care disparities, as some individuals may have problems in using these technologies (Guzik et al., 2021; Strowd et al., 2021). Men in this RCT who were unable or unwilling to access the TEAM program via internet had the option of using the phone to participate, but this may not have been enough to optimize full engagement over the longer-term. Sensitivity analysis conducted to evaluate predictors of missing data/attrition found that men with less education, those who lived alone and those who were prescribed fewer stroke risk reduction medications were less likely to be retained in the study. It is possible that men with greater psychosocial barriers may need more intensive and/or in-person approaches to engage them over the longer-term.
This trial found that our entire enrolled RCT sample had numeric but not statistically significant improvements in the primary outcome of SBP and that there were no differences in SBP between individuals randomized to the TEAM intervention versus Waitlist control. Rather similar to the TEAM intervention, the SUCCEED program (Secondary Stroke Prevention by Uniting Community and Chronic Care Model Teams Early to End Disparities) uses a team-based intervention (advanced practice professional–community health worker team) that addresses multiple factors, including medication adherence, physical activity, diet, self-management skills, and social isolation in individuals with recent ischemic stroke, TIA, or intracerebral hemorrhage in a safety-net setting (Towfighi et al., 2017, 2021). In an RCT testing SUCCEED versus usual care, the primary outcome of mean SBP improved at 12 months in both experimental and control groups, with no significant differences in the change between groups (Towfighi et al., 2021). In the SUCCEED trial (Towfighi et al., 2021) it was found that although 90% in the SUCEED group received some components of the multi-pronged intervention, only 15% received the intended full dose. Like the TEAM RCT, ready program access to those that are most vulnerable/in need could have resulted in less robust outcomes than expected.
Post-hoc analysis on BP outcomes among sub-groups with elevated BP at baseline using established thresholds (SBP ≥ 140 and SBP ≥ 130) found significant SBP and DBP change from baseline to 6-month follow-up in the group as a whole and in those individuals who participated in the TEAM program. While attention and being in a clinical trial appear to have a positive impact on BP among Black male stroke survivors, specific approaches to optimize engagement in health management in high-risk Black men are needed.
In addition to the high rate of attrition, this RCT had several other methodological limitations that suggest cautious interpretation of results. The fact that there were no study entry SBP inclusion criteria may have contributed to possible BP floor effects and difficulty ascertaining the best target population for the TEAM study. Post-hoc analysis suggests that TEAM might be most appropriate for those with elevated BP above 130. At the same time, post-program TEAM participant satisfaction surveys suggested that men enjoyed the program, found it valuable, and participants may have found benefit beyond changes in BP. Other RCT limitations include the relatively limited time duration and the fact that most of the RCT was conducted during the COVID pandemic. These factors make it hard to generalize the future risk of recurrent stroke for men in the RCC. In spite of these limitations, these RCT findings may help to inform work to address stroke health disparities. Future research might target Black men with poorly controlled BP and other significant risk factors and further explore optimal approaches to address barriers that could impede the ability to engage in and with risk reduction programs.
Footnotes
Ethical Considerations
This study was approved by the local Institutional Review Board (IRB) at University Hospitals Cleveland Medical Center on July 16, 2019 (Number: STUDY20190896).
Consent to Participate
All study participants provided written informed consent prior to participating in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by a research grant from the U.S. National Institute of Nursing Research IR01NR018023-01A1 (PIs Sajatovic and Still).
Declaration of Conflicting Interest
Martha Sajatovic: Research grants within past 3 years: Neurelis, Intra-Cellular, Merck, Otsuka, Alkermes; Consultants in the past year: Alkermes, Otsuka, Lundbeck, Janssen, Teva; Royalties in the past year: Springer Press, Johns Hopkins University Press, Oxford Press, UpToDate. All other authors have no conflicts to declare.
Data Availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on request