
Abstract
Purpose
This study examined how transitions in living arrangements are associated with changes in sleep quality and sleep duration among Chinese older adults.
Major findings
Using four waves of the Chinese Longitudinal Healthy Longevity Survey data (2008–2018), we examined how living arrangement transitions affect sleep among 10,473 observations from older adults (65+). Cox models showed that older adults who remained living with household members (hazard ratio [HR] = 0.66, 95% CI: 0.53–0.81; p < .001) or transitioned to living alone (HR = 0.71, 95% CI: 0.57–0.89; p = .003) had significantly lower risks of experiencing a decline in sleep quality compared to those who transitioned to institutional care. Although similar patterns were observed for sleep duration, these associations were not statistically significant.
Conclusions
Older adults transitioning to institutional care may warrant additional monitoring and supportive care regarding sleep health during residential transitions.
Introduction
As China undergoes an accelerated demographic transition, the proportion of older adults in its population is increasing rapidly. The number of individuals aged 60 and above is projected to grow from 254 million in 2019 to 402 million by 2040, comprising approximately 28% of the total population (World Health Organization, n.d.). Meanwhile, the burden of chronic diseases among older adults has also intensified (Han et al., 2020). By 2019, nearly 75% of individuals aged 60 and over were affected by noncommunicable conditions such as cardiovascular disease, diabetes, and hypertension(World Health Organization, n.d.), which together account for around 80% of deaths in this age group(Thomas et al., 2020). These trends have intensified concerns about the health and well-being of China's aging population. Given the growing burden of chronic disease, it is increasingly important to understand the roles of modifiable biological and social behavioral factors such as sleep health and living arrangements in promoting healthy aging through family- or community-based interventions.
Sleep health is a fundamental component of healthy aging and is closely associated with multiple health outcomes. This is especially concerning given the emerging trend of shorter sleep duration and declining sleep quality among Chinese older adults (Pan et al., 2023). For older adults aged 65 years and above in China, a sleep duration of 7 to 8 h per day is recommended for optimal health with maximum health benefits achieved at 7.5 h of sleep (Song et al., 2024), while sleeping less than 5 h or more than 9 h is not advised (Hirshkowitz et al., 2015). A sleep duration of 7–8 h may protect against disability in activities of daily living (ADL), while both shorter and longer durations are associated with increased risk of ADL (Cai et al., 2025), all-cause mortality (Du et al., 2021), and frailty (Song et al., 2024) in this population. Additionally, poor sleep quality became increasingly prevalent among older Chinese adults, rising from 34.87% in 2008 to 47.67% in 2018(Tao et al., 2023). Poor sleep quality among Chinese older adults is linked to a range of adverse outcomes, including cognitive decline (Qian et al., 2025), memory impairment (Ma et al., 2020), and reduced physical functioning (Chang et al., 2025). Without timely interventions, worsening sleep quality may accelerate the onset and progression of chronic health conditions in later life (Lee et al., 2022).
Identifying social and environmental factors that affect sleep can guide targeted interventions to promote healthy aging. Among these, living arrangements are crucial, influencing daily routines, emotional well-being, and social support (Zhou et al., 2018). According to the 2020 census, the first to examine the living arrangements of Chinese older adults aged 60 and above, 43.7% live with a spouse, 23.1% live with both spouse and child, 16.6% live with a child only, and 12% live alone. Institutional living remains rare at 0.7%, significantly below the government's target of 3% (Zhao, 2023). Living arrangements significantly impact health outcomes among older Chinese adults. Those living alone, with relatives, or in institutions tend to experience poorer emotional health and higher risks of depression compared to those living with family (Jia et al., 2023; Ren & Treiman, 2015; Zhang & Zhang, 2015). Residing in or transitioning to institutional care has been linked to an increased risk of mortality (Feng et al., 2017). These findings help lay the groundwork for understanding how living arrangements may also influence sleep outcomes in later life.
Prior research on Chinese older adults has shown that those living with family members are more likely to report better sleep quality and longer sleep duration than those living alone (Lee et al., 2020). Gender differences were also observed, with older women living alone reporting poorer sleep quality than their male counterparts (Griffin et al., 2022). Additionally, for men experiencing poor sleep quality, co-residence with others appeared to offer a protective effect against mild cognitive impairment (Yang et al., 2023). However, most existing studies have primarily focused on static living arrangements measured at a single point in time (Lee et al., 2020), while less attention has been paid to how transitions in living arrangements are associated with changes in sleep outcomes over time. This issue is particularly important in China, where rapid population aging, declining fertility, and changing family structures have substantially reshaped living arrangements among older adults (Lei et al., 2015; Zhao, 2023).
To address these gaps, this study utilized four waves of data (2008–2018) from the Chinese Longitudinal Healthy Longevity Survey (CLHLS) to examine how changes in living arrangements are associated with changes in sleep quality and duration among Chinese older adults. This study contributes to literature in three ways. First, it adopted a longitudinal perspective by examining living arrangement transitions rather than static living arrangements (Lee et al., 2020). Second, it investigated changes in sleep-related outcomes over time instead of sleep status at a single time point. Third, rather than treating living arrangements and sleep as static conditions, this study modeled transitions in both residential status and sleep outcomes over time using repeated longitudinal observations. This transition-based approach enables a more dynamic assessment of how changes in living arrangements are associated with subsequent changes in sleep health among older adults. We hypothesized that changes in living arrangements are significantly associated with changes in sleep quality and duration. By adopting a within-person longitudinal framework, we aimed to identify how transitions in living arrangements were associated with subsequent changes in sleep quality and sleep duration over time and provide evidence-based recommendations to inform policies that support sleep health among older adults in China.
Method
Data Source
We extracted data from four waves collected at different time points (2008 wave: 2008–2009; 2011 wave: 2011–2012; 2014 wave: 2014; 2018 wave: 2017–2018) from the CLHLS dataset. The CLHLS is a nationally representative, large-scale longitudinal study focused on the health and longevity of older adults in China, initiated by international researchers at Duke University's Center for the Study of Aging and Human Development. Participants were randomly selected and interviewed in person by trained investigators after providing informed consent. The survey collected comprehensive information covering demographic and socioeconomic characteristics, health status, lifestyle behaviors, economic conditions, and social support networks. The CLHLS sample covers approximately 85% of the older adult population across 631 counties and cities in 22 provinces and major urban areas in China (Zeng, 2012).
To examine changes in living arrangements, we included participants who were interviewed in at least two consecutive waves between 2008 and 2018. At the baseline interview, respondents were required to provide complete information on three key variables: participant ID, interview year, and living arrangement (specifically indicating that they lived with household members). In the follow-up interviews, only those who also provided complete responses to all relevant items were retained. This allowed us to track transitions in living arrangements such as shifting from co-residence to living alone, institutional care, or continue to live with household members.
We excluded individuals under 65 years of age. The final analytic sample included 6,900 unique participants, contributing a total of 10,473 person-wave observations with complete data on all variables of interest (see Online Appendix Figure 1 for a flowchart of the sample selection process).
As the original CLHLS study and its design had already been approved by the institutional review boards of Duke University and Peking University (IRB00001052-13074), and since we used de-identified, publicly available data for this analysis, the current study did not involve human subjects. Therefore, additional IRB approval was not required.
Outcome Variables
We included two self-reported sleep measures: sleep quality and sleep duration. Sleep quality was assessed with the question, “How about the quality of your sleep?” rated on a 5-point scale from “very bad” to “very good.” Consistent with previous sleep-related studies using the same dataset, responses of “good” or “very good” were classified as good sleep quality, while all other responses were classified as not good (Gu et al., 2010; Lee et al., 2020). Sleep duration was assessed by asking, “How many hours do you usually sleep each day?” Responses were recoded into a binary variable: 7–8 h (recommended sleep duration for older adults) and not within 7–8 h, based on guidelines from the National Sleep Foundation and prior studies on optimal sleep for older adults (Hirshkowitz et al., 2015; Lee et al., 2022).
Primary Predictor
The primary predictor was a living arrangement transition, describing changes among individuals who initially lived with household members. Based on follow-up status, they were categorized into three groups: (1) stayed with household members, (2) became alone, and (3) transitioned to institutional care.
Covariates
We included a range of sociodemographic variables as covariates in the analysis: age (categorized as 65–80 = 0, 81–95, and above 95), gender (female = 0, male), educational attainment (no = 0, yes), marital status (others = 0, including divorced, widowed, or never married; married), community of residence (rural = 0, urban), and geographical region (Central-South = 0; other categories include East, North, Northeast, and West, based on major provinces and metropolitan areas). Geographical region was included to account for regional differences in socioeconomic development, healthcare access, and living environments that may affect sleep and living arrangement patterns among older adults (Lee et al., 2020). To account for health-related factors, we included the number of inpatient treatments for chronic conditions in the past two years (none = 0, 1–2, and more than 2). We also included ADL as an indicator of physical functioning, as previous longitudinal studies have identified functional limitations as significant risk factors for sleep-related problems among Chinese older adults (Lee et al., 2022). ADL impairment was defined as requiring assistance or supervision in at least one of six basic self-care activities, including bathing, dressing, eating, indoor mobility, toileting, and continence. Participants who were able to perform all six activities independently were classified as having no impairment coded as 0 (Xu et al., 2026). Life satisfaction was included as a continuous variable measured on a 5-point scale (1 = very poor to 5 = excellent) to reflect psychological well-being. Current health behaviors, including smoking, drinking, and exercise, were also included and coded as binary variables (no = 0, yes = 1). Detailed coding information for all variables is provided in Online Appendix Table 1.
Analytical Strategies
As illustrated in Figure 1, Cox two-state regression models were applied to examine the associations between living arrangement transitions and changes in sleep quality and sleep duration among Chinese older adults. This approach accommodates repeated observations and time-varying transitions between states, making it suitable for longitudinal analyses of dynamic living arrangements and sleep outcomes (Lee et al., 2024; Xu, 2025). Compared with conventional survival models, this framework better captures recurrent and reversible transitions over time. Details of the reversible two-state framework used in this study are presented in Online Appendix Figure 2.
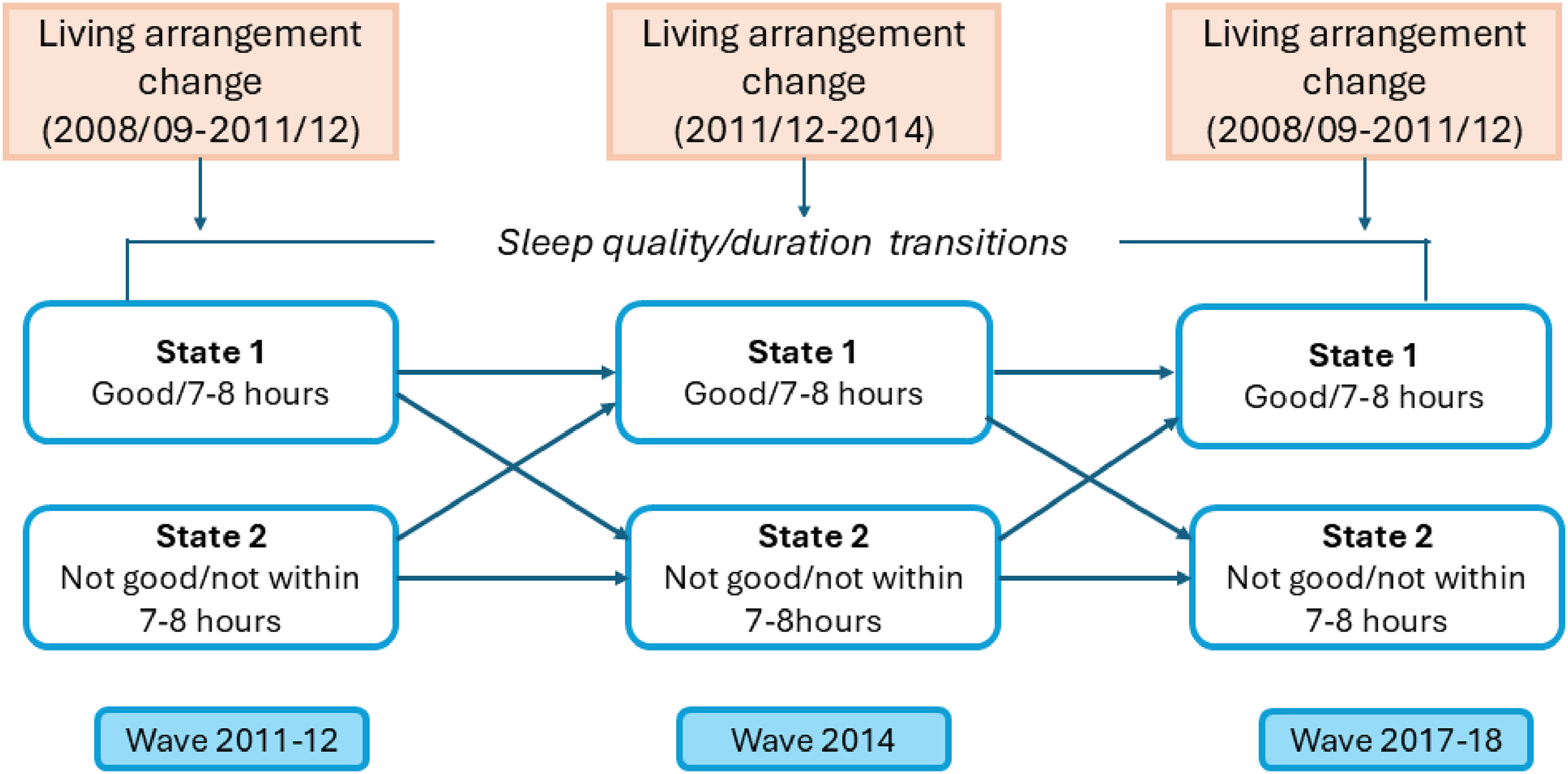
Two-state sleep quality/duration transitions by living arrangement changes.
At each observation, participants who had co-resided with household members in the previous wave were classified according to subsequent living arrangement transitions, including remaining with household members, becoming alone, or transitioning to institutional care. For sleep quality, transitions were defined as: (1) from good to not good, and (2) no change (not good to not good) (Lee et al., 2022). For sleep duration, transitions were (1) from 7 to 8 h (meeting the recommended duration) to not within 7–8 h, and (2) no change (remaining outside the recommended range). The probability of remaining in a given sleep-quality state was defined as the complement of the probability of transitioning to the alternative state at that observation. For example, the probability of remaining in good sleep quality was calculated as 1 minus the probability of transitioning from good to not good sleep quality, whereas the probability of transitioning from not good to good sleep quality was defined as 1 minus the probability of remaining in the not good state. The same transition mechanism was applied to sleep duration. Given its public health relevance, our primary focus was on Chinese older adults whose sleep quality declined from good at baseline to not good at follow-up, as well as those who initially met the recommended sleep duration (i.e., 7–8 h per day) but did not meet this recommendation at follow-up.
Following previous social-behavioral studies using the same dataset, we conducted statistical analyses using unweighted data, as the CLHLS sampling scheme does not include key compositional variables needed for proper weighting (Gu et al., 2010). Moreover, weighted regression may inflate standard errors (SEs) and yield less accurate estimates (Vermunt & Magidson, 2007). Adjusted hazard ratios (HRs) and 95% confidence intervals (95% CIs) were reported. All statistical tests were two-tailed with a significance level of 0.05. Analyses were performed using R version 4.2.1. Sensitivity analyses were conducted after excluding participants who transitioned to institutional care to assess the robustness of the findings.
Results
Sample Characteristics
Table 1 shows the associations between sleep quality and adherence to the recommended daily sleep duration (7–8 h) across the 2011–2012, 2014, and 2018 waves of the CLHLS. In each year, participants with good sleep quality were more likely to meet the recommended duration, with all associations statistically significant (p < .001). Figure 2 shows the trends in mean sleep quality and duration from 2011 to 2018, stratified by living arrangement transitions. Participants who transitioned to institutional care exhibited the most fluctuation, with a peak in 2014 followed by a sharp decline by 2018. In contrast, individuals who became alone or stayed with household members showed relatively stable but slightly declining trends.
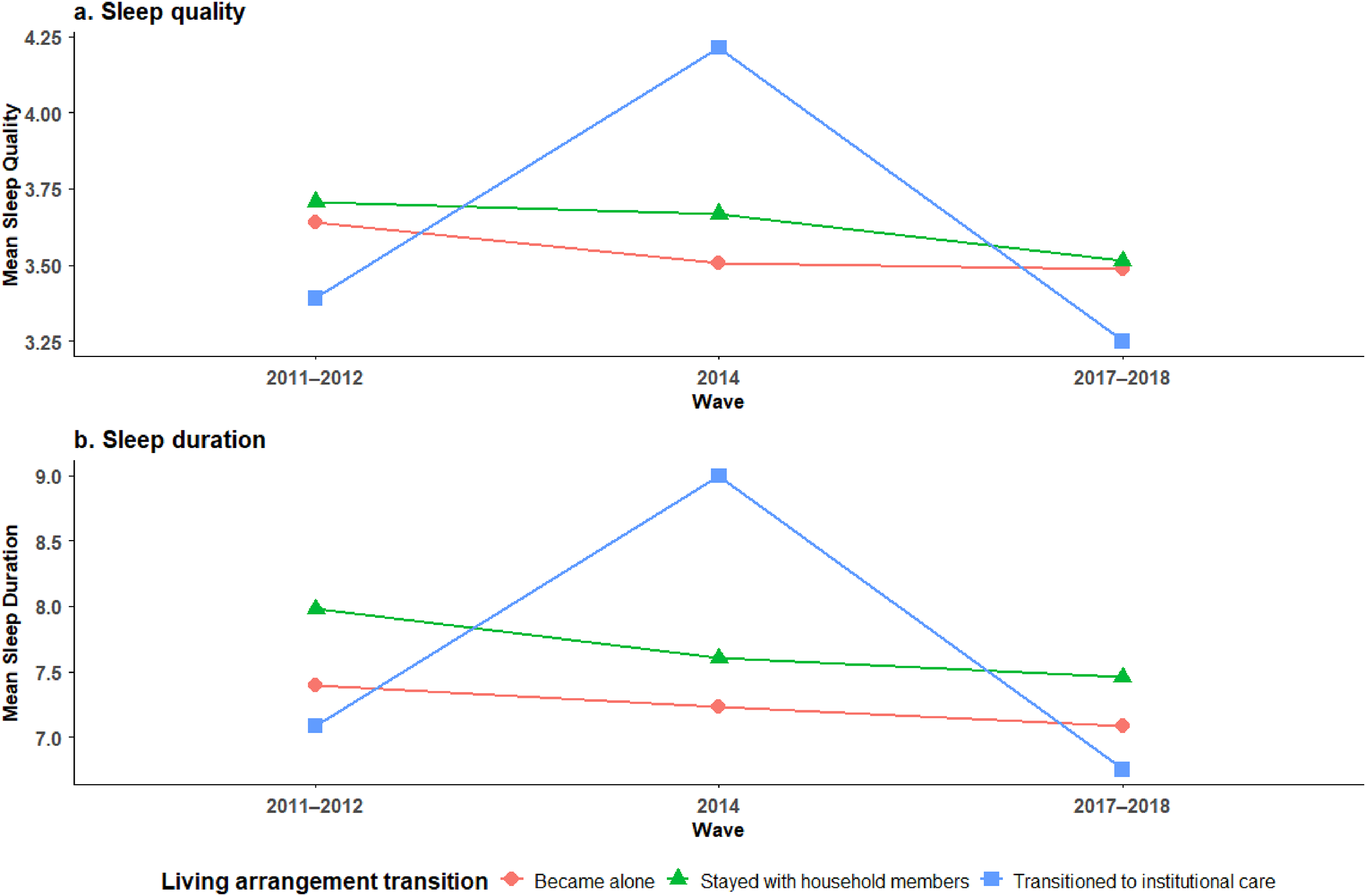
Changes in mean sleep quality and duration across waves by living arrangement transition status.
Observations and Correlation of Sleep Quality and Recommended Daily Sleep Duration by Survey Year.
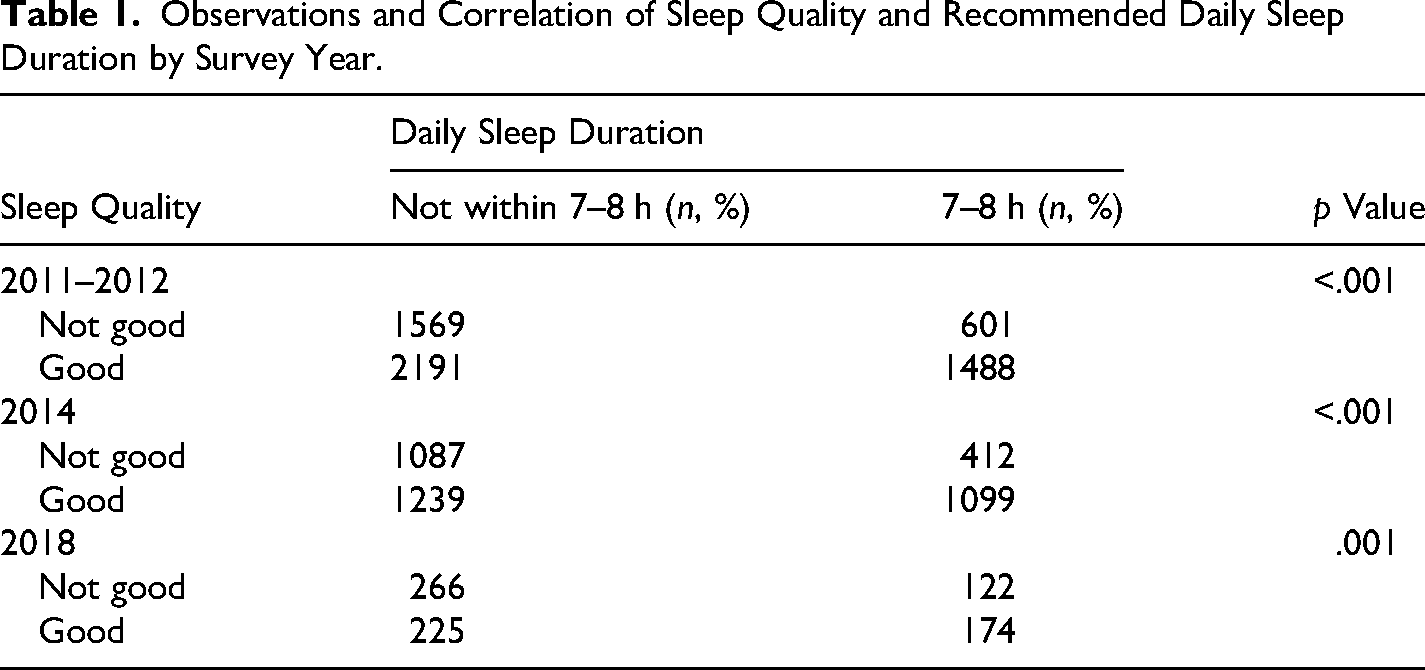
Table 2 summarizes the characteristics of the analytic sample, comprising 10,473 observations from 6,900 older adults. Most participants stayed with household members (90.24%), while 9.15% became alone and 0.61% transitioned to institutional care. The majority were aged 65–95, with 42.92% aged 81–95 and 41.30% aged 65–80. About half were female (51.01%) and had no formal education (51.65%). Over half were unmarried (50.92%) and lived in urban areas (53.69%), mainly in Central-South (36%) and East China (39.24%). Most reported no smoking (80.89%), no alcohol use (82.54%), and no regular exercise (64.33%). In addition, 74.43% had not required inpatient treatment in the past two years, and 76.72% reported no ADL impairment. The average life satisfaction score was 3.81 (SD = 0.81). Overall, 61.26% reported good sleep quality and 37.2% slept 7–8 h daily.
Sample Characteristics by Living Arrangement Among Chinese Older Adults: The Chinese Longitudinal Healthy Longevity Survey, 2008–2018 (N = 10,473).
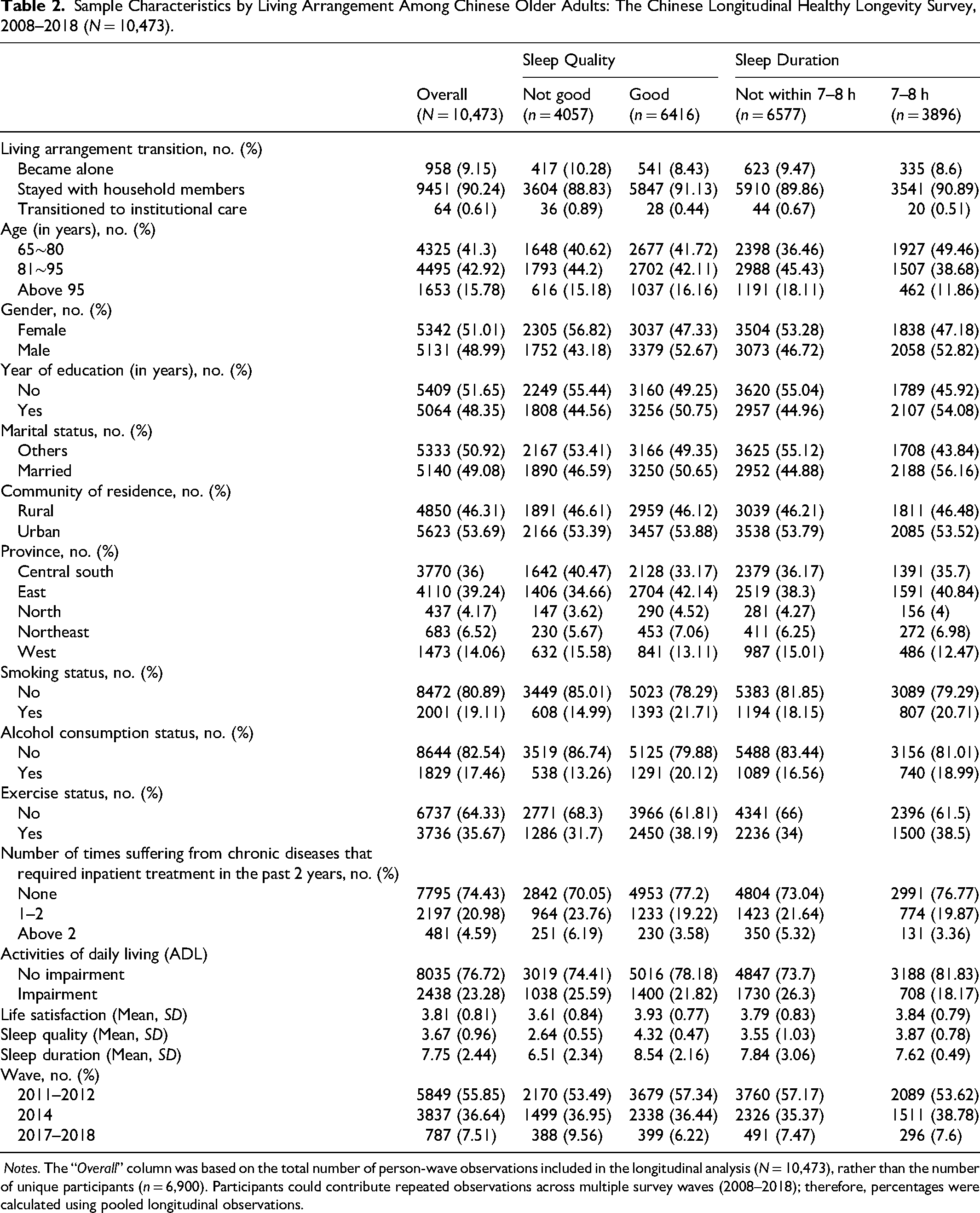
Detailed distributions of key variables by sleep quality and duration are also provided in Table 2.
Associations Between Living Arrangement Transitions and Changes in Sleep Quality and Sleep Duration (2008–2018)
Table 3 presents the associations of changes in living arrangements with declining sleep quality and sleep duration among older Chinese adults from 2008 to 2018. In the first model, compared to those who transitioned to institutional care, older adults who remained with household members (HR = 0.66, 95% CI: 0.53–0.81; p < .001) or became alone (HR = 0.71, 95% CI: 0.57–0.89; p = .003) had significantly lower risks of transitioning from good to not good sleep quality. Factors associated with a lower risk of declining sleep quality included being male (HR = 0.90, 95% CI: 0.84–0.96; p = .002), exercising regularly (HR = 0.88, 95% CI: 0.83–0.94; p < .001), and reporting higher life satisfaction (HR = 0.75, 95% CI: 0.73–0.78; p < .001). In contrast, having multiple chronic conditions requiring inpatient care was associated with increased risk of declining sleep quality (all HRs > 1; p < .001).
Associations of Living Arrangement Changes With Sleep Quality and Sleep Duration Among Chinese Older Adults: The Chinese Longitudinal Healthy Longevity Survey, 2008–2018.
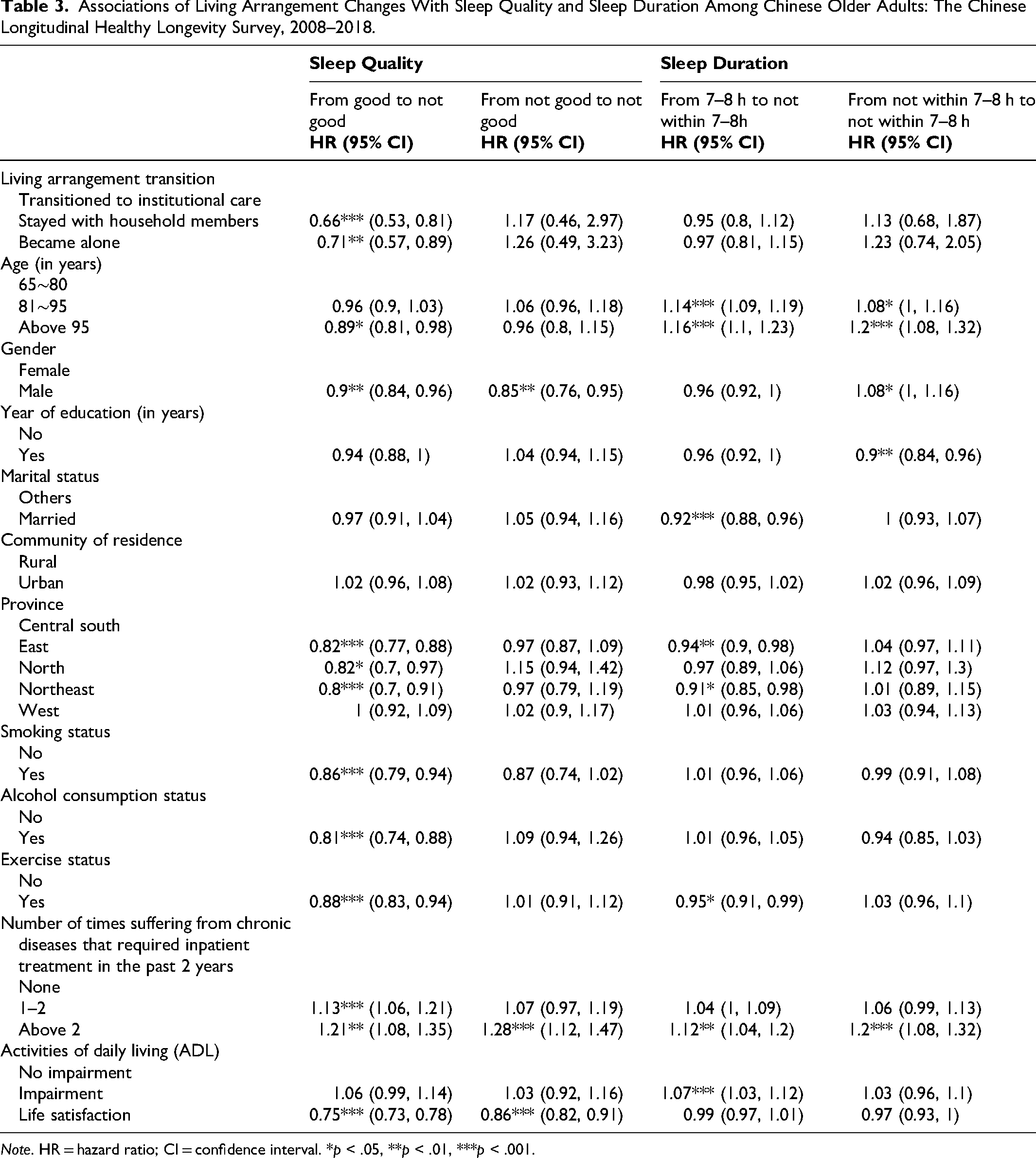
Note. HR = hazard ratio; CI = confidence interval. *p < .05, **p < .01, ***p < .001.
In the second model, changes in living arrangements were not significantly associated with the transition from meeting to not meeting the recommended sleep duration (7–8 h). However, older adults aged 81–95 (HR = 1.14, 95% CI: 1.09–1.19; p < .001) and above 95 (HR = 1.16, 95% CI: 1.10–1.23; p < .001), as well as those with more than two chronic inpatient episodes (HR = 1.12, 95% CI: 1.04–1.20; p = .003), were more likely to not meet the recommended sleep duration range. Factors associated with a lower likelihood of not meeting the recommended sleep duration included being married (HR = 0.92, 95% CI: 0.88–0.96; p < .001) and living in eastern provinces (HR = 0.94, 95% CI: 0.90–0.98; p = .003).
Given the relatively small number of institutional-care transitions (0.61% of observations), sensitivity analyses were conducted after excluding this subgroup. The overall direction of the associations between living arrangement transitions and sleep outcomes remained generally consistent with the primary analyses, although some associations were attenuated and no longer statistically significant (see Online Appendix Table 2).
Discussion
We used nationally representative longitudinal data from the CLHLS and applied Cox two-state regression models to examine how changes in living arrangements were associated with self-reported sleep quality and adherence to recommended daily sleep duration. The primary contribution of this study lies in its transition-based longitudinal framework. Unlike prior studies that primarily examined static living arrangements or cross-sectional sleep outcomes, we focused on within-person transitions in both residential status and sleep health over time. This approach enabled us to capture the dynamic nature of later-life living arrangements and examine whether residential transitions were associated with changes in sleep quality and sleep duration. Our results indicated that, compared to older adults who transitioned to institutional care, those who remained with household members or lived alone had a significantly lower risk of experiencing a decline in sleep quality. A similar pattern was observed for sleep duration, although the associations did not reach statistical significance. Nonetheless, the direction of the HRs suggests a potentially favorable association between non-institutional living arrangements and maintaining optimal sleep duration. To our knowledge, few studies have simultaneously modeled transitions in both living arrangements and sleep outcomes among older Chinese adults using a longitudinal within-person framework.
These findings align with previous large-scale studies in China, which have consistently shown a high prevalence of poor sleep quality among institutionalized older adults (67.3%) (Zhu et al., 2020), compared to community-dwelling older adults (less than 35%) (Dong et al., 2018; P. Wang et al., 2020). A plausible explanation for this disparity is that individuals who move into institutional care tend to be older (86.3% were aged 81 or above in our study) and have more chronic conditions (33.4% had at least one chronic illness), both of which are known risk factors for poor sleep (Gnädinger et al., 2018). Additionally, environmental discomfort and standardized care routines in institutional settings may negatively affect sleep (Gentili et al., 1997). Prior research has identified sleep disturbances, low sleep efficiency, and prolonged sleep latency as common problems in nursing homes (Eser et al., 2007; Orhan et al., 2012; Zhu et al., 2020), with nocturia and environmental disruptions frequently cited as contributing factors (Ersser, 1999).
In contrast, the association between living arrangement transitions and sleep duration were not statistically significant. Nevertheless, HRs below 1 suggest a potential protective effect of remaining with household members or becoming alone in helping older adults maintain sleep duration within the National Sleep Foundation's recommended range of 7–8 h per day (Hirshkowitz et al., 2015).One possible explanation for the lack of statistical significance is that sleep duration may be less sensitive than sleep quality to psychosocial (e.g., retirement, social disengagement, and emotional distress) and environmental (e.g., household composition and noise levels) changes (Li et al., 2018; Miner & Kryger, 2020; Stewart & Arora, 2017; Y. Wang et al., 2021; Yue et al., 2022). Instead, sleep duration may be more strongly influenced by biological, behavioral, and medical factors such as chronic diseases (Gu et al., 2010), medication use (Holbrook et al., 2000), circadian rhythm disruptions (Mander et al., 2017), and lifestyle factors including diet and physical activity (Liu et al., 2025; S. Wang et al., 2017), Moreover, aging itself is associated with a progressive decline in total sleep duration (Edwards et al., 2010). A meta-analysis of 21 studies found that older adults in China average only 6.82 h of sleep per night (Lu et al., 2017), falling short of the 7.6 h observed in a nationwide Chinese adult sample (Chu et al., 2023). These age-related changes also encompass shifts in sleep architectures, including earlier bed and wake times, lighter sleep, more frequent nocturnal awakenings, and a reduced proportion of restorative slow-wave sleep (Li et al., 2018). These physiological changes contribute to poorer overall sleep quality in older adults (Gadie et al., 2017). Therefore, while changes in living arrangements may be related to maintaining optimal sleep duration, potentially through social support or emotional well-being, these associations may be too subtle or indirect to detect statistically, particularly given the strong influence of biological aging on sleep patterns.
Additionally, the relatively small proportion (0.61%) of transitions to institutional care observed in this study is consistent with the current eldercare pattern in China, where most older adults rely primarily on family-based care rather than formal institutional services (Zhao, 2023). Cultural preferences for family caregiving, together with the limited availability and affordability of long-term care services, may be related to this pattern (Zhang & Yang, 2024). In the sensitivity analyses excluding institutional-care transitions, the direction of the associations remained generally consistent with the primary findings, although some estimates were attenuated after the reference category changed. Continued co-residence with household members remained associated with more favorable sleep outcomes.
Our findings show that changes in living arrangements were more strongly associated with sleep quality than sleep duration, possibly because sleep quality is more sensitive to emotional, social, and environmental factors. Older adults experiencing residential transitions, particularly transitions into institutional care, may represent a potentially vulnerable group with respect to sleep health and may benefit from additional sleep-health monitoring and supportive services. Community- and family-based support programs that promote emotional well-being and reduce loneliness during major life transitions may also be relevant to sleep health in later life (Koffel et al., 2023).
There are several limitations in our study. First, sleep quality and duration were assessed using two self-reported items rather than objective measures or validated scales such as the Pittsburgh Sleep Quality Index, which may introduce recall or reporting bias. Second, sleep quality and sleep duration were dichotomized to fit the Cox two-state regression framework and maintain model interpretability. However, this approach may have resulted in some loss of information and may not fully distinguish heterogeneous sleep patterns, particularly differences between short and long sleep duration. Future studies with larger sample sizes may consider multi-state modeling approaches or more refined sleep classifications to further examine heterogeneous sleep patterns among older adults. Third, transitions in living arrangements were categorized into three broad groups, which may oversimplify important differences; for example, co-residing with a spouse versus adult children may have varying impacts on sleep. Future studies should consider more detailed classifications of household composition. Fourth, although we examined changes in living arrangements, the CLHLS does not provide information on the timing, duration, or underlying reasons for these transitions (e.g., widowhood, financial hardship, or health decline) (Hall et al., 2008; Monk et al., 2008), all of which may independently influence sleep outcomes. Fifth, residual confounding related to transitions into institutional care cannot be fully excluded. Although we additionally adjusted for ADL limitation (Lee et al., 2022), older adults entering institutional care may still differ from those remaining in community settings in terms of underlying health conditions, cognitive status, and social support factors that may influence sleep outcomes. In addition, the relatively small institutional-care group should be considered when interpreting these findings. Finally, as with all observational studies, the findings should be interpreted as associations rather than causal effects. Future studies using objective measures of sleep and more granular tracking of household dynamics are warranted to better understand the causal mechanisms underlying these associations.
Conclusion
In conclusion, our study adds new evidence to the existing literature by focusing on how changes in living arrangements, rather than static living environments, are associated with sleep health among older adults in China. Using recent nationally representative longitudinal data from the CLHLS, we found that staying with household members or living alone, compared with transitioning to institutional care, was associated with a lower risk of declining sleep quality over time. While similar patterns were observed for sleep duration, these associations were not statistically significant. These findings underscore the importance of considering dynamic residential transitions when evaluating sleep health in later life and suggest that older adults undergoing institutional-care transitions may require additional attention regarding sleep health and supportive care. Further research is warranted to examine underlying mechanisms and explore these associations across different cultural and contextual settings.
Supplemental Material
sj-docx-1-ahd-10.1177_00914150261458268 - Supplemental material for How Changes in Living Arrangements Are Associated With Changes in Sleep Quality and Duration Among Chinese Older Adults: Results From a Longitudinal Study (2008–2018)
Supplemental material, sj-docx-1-ahd-10.1177_00914150261458268 for How Changes in Living Arrangements Are Associated With Changes in Sleep Quality and Duration Among Chinese Older Adults: Results From a Longitudinal Study (2008–2018) by Cai Xu in The International Journal of Aging and Human Development
Supplemental Material
sj-docx-2-ahd-10.1177_00914150261458268 - Supplemental material for How Changes in Living Arrangements Are Associated With Changes in Sleep Quality and Duration Among Chinese Older Adults: Results From a Longitudinal Study (2008–2018)
Supplemental material, sj-docx-2-ahd-10.1177_00914150261458268 for How Changes in Living Arrangements Are Associated With Changes in Sleep Quality and Duration Among Chinese Older Adults: Results From a Longitudinal Study (2008–2018) by Cai Xu in The International Journal of Aging and Human Development
Footnotes
Ethical Considerations
This study utilized de-identified, publicly available data and did not involve direct interaction with human subjects. As such, additional approval from an Institutional Review Board (IRB) was not required.
Consent to Participate
Not required for this study.
Consent for Publication
Not required for this study.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
The secondary data utilized in this study were extracted from the publicly available data of the Chinese Longitudinal Healthy Longevity Survey (CLHLS).
Supplemental Material
Supplemental material for this article is available online.
Code Availability
Available on request.
Author Biography
References
{kind=link}
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.