
Abstract
Dementia is a prevalent diagnosis, with individuals and their families affected by disease challenges including dementia-related stigma. Dementia-related stigma may lead to isolation, infantilization, discrimination, and a poorer quality of life. Stigma-reduction interventions have been implemented to combat these harms. This meta-analytic review examined seven dementia-related stigma reduction studies, totaling 13 interventions and 26 effect sizes. Overall, treatment groups had nonsignificant reductions in stigmatizing views (g = −.24) and improved quality of life (g = .20). Quality of life was a significant predictor of stigma reduction (β = −1.0732, P = .004), even though a nonsignificant correlation between quality of life and stigma was found (r = −.49, P = .09). This meta-analytic review highlights the difficult-to-change nature of dementia-related stigma, as well as the dearth of consensus among the field when it comes to intervention methods and measurement protocols for nuanced phenomena like stigma or quality of life.
Dementia is not only a prevalent and challenging illness, but also a stigmatized one. There are currently more than 50 million people living with dementia worldwide, and that number is expected to triple by 2050 (Kim et al., 2023). Dementia, though caused by a variety of underlying diseases, refers to the progressive neurological symptoms characterized by cognitive and functional decline such as memory loss (Alzheimer's Association, 2025). Beyond the physical impact of the condition, people living with dementia are also subject to the harm caused by stigmatization (Nandhakumar, 2024). Stigma can be defined as the social disapproval, negative attitudes, and poor reception of a group due to a particular characteristic (Rewerska-Juśko & Rejdak, 2020). In the case of dementia, stigmatization and consequent discriminatory behavior can contribute to social isolation, delay help-seeking behavior and treatment, and lead to feelings of shame, low self-esteem, depression, and anxiety (Nguyen & Li, 2020).
Attempts to reduce dementia-related stigma have been made through a variety of interventions. A major contributor to the stigmatization of dementia is the lack of knowledge that the public has on the condition (Nguyen & Li, 2020). Both education-based and contact-based interventions have shown promise in rectifying this issue, but there is no standardization or consensus (Nandhakumar, 2024; Noguchi et al., 2023). This meta-analysis aims to provide a systematic integration of the available literature on interventions that aim to reduce stigma and increase the quality for people living with dementia.
Stigmatization of Dementia
Stigma has been defined in a variety of different ways over the years and is broadly conceptualized as the social process in which the disapproval of a group leads to harmful consequences (Rewerska-Juśko & Rejdak, 2020). Goffman (1963) first proposed that stigma describes a relationship between an attribute and a stereotype. Stigma manifests through negative beliefs, emotions, and behaviors, and can occur through both public stigma, self-stigma, and courtesy stigma (Siette et al., 2023). The diverse manifestation of stigma can make it a complex issue to address, but one worthy of attention. Public or societal stigma refers to the negative attitudes that are publicly held regarding a group of people, in this case, people living with dementia (Noguchi et al., 2023). Self-stigma describes the internalized acceptance of negative stereotypes, which can result in shame, low self-esteem, and low self-efficacy felt by the person with dementia (Nguyen & Li, 2020). The impact of stigma can even extend beyond the individual diagnosed with dementia, known as courtesy stigma, in which those same negative beliefs and attitudes are directed toward people who are associated with the group in some way, such as family members, caregivers, and health professionals (Siette et al., 2023). Thus, the effects of dementia stigmatization span beyond the millions who are living with a condition, making it a widespread issue in need of rectification.
Stigma management communication (SMC) theory states that all SMC behaviors are reflective of the individual's acceptance or denial of the existence of a stigma and the applicability of a stigma to oneself (Meisenbach, 2010). In regard to dementia, stigmatization is common and can contribute to harmful effects across all domains (Kim et al., 2023). It can contribute to social isolation, shame, embarrassment, feelings of inferiority, distress, poor mental health, lack of confidence, reluctance to seek help for dementia symptoms, delayed treatment, and much more (Nguyen & Li, 2020; Wong et al., 2024). According to SMC theory, there are six major strategies that stigmatized individuals employ based on whether they accept or challenge the stigma's existence and applicability: accepting, avoiding, evading responsibility, reducing offensiveness, denying, and ignoring or displaying (Meisenbach, 2010). Several of these strategies could reduce help-seeking behaviors and deter individuals from getting screened for dementia, potentially leading to problematic downstream consequences such as worsened health outcomes.
Discrimination as a result of dementia-related stigma can take many forms, but is often simply avoidance (Nguyen & Li, 2020). Common stereotypes of people living with dementia include the beliefs that they are incompetent, dangerous, or child-like (Nguyen & Li, 2020; Wong et al., 2024). This can lead to the infantilization and social exclusion of people living with dementia (Nandhakumar, 2024). Even medical providers are affected by dementia-related stigma, exemplified by a lack of empathy or a delayed disclosure of the diagnosis to patients for fear of causing emotional distress (Alzheimer's Association, 2025; Siette et al., 2023). For some individuals, the stigma causes more distress than the actual symptoms of dementia (Wong et al., 2024).
The stigma and discrimination that people living with dementia experience can be compounded by elements like culture, race, and immigration status (Wong et al., 2024). Dementia-related stigma can be especially harmful for already marginalized communities such as ethnic minorities, low-income individuals, culturally and linguistically diverse communities, and sexual and gender minorities (Alzheimer's Association, 2025; Siette et al., 2023). Additionally, sociodemographic factors can influence levels of both dementia-related knowledge and stigma. Kim et al. (2023) found that individuals who were older, male, less educated, and know or knew someone with dementia were found to be more likely to hold stigmatizing beliefs and/or perform discriminatory behaviors. There is also significant variability in the attitudes and beliefs about dementia among different cultures (Nguyen & Li, 2020). For instance, dementia may be attributed to bad luck, normal aging, punishment from God, witchcraft, or the luxury of living until old age, all depending on just where someone is in the world (Nandhakumar, 2024; Nguyen & Li, 2020; Rewerska-Juśko & Rejdak, 2020). Diversity, in both experience and perception, is an important complexity to consider when studying dementia-related stigma.
Among the detrimental effects of dementia-related stigma is its harmful impact on the quality of life (QoL) of both people living with dementia and their family members (Nguyen & Li, 2020). QoL is a valuable metric in understanding an individual's well-being; however, its amorphous definition can make it challenging to quantify. Adjustments to this definition over time have largely been guided by a growing emphasis on the individual's subjective perceptions (Cai et al., 2021). The World Health Organization's (2012) current definition of QoL is “an individual's perception of their position in life in the context of the culture and value systems in which they live and in relation to their goals, expectations, standards and concerns.” The prejudice and discrimination experienced by stigmatized individuals can result in a decreased QoL, such as that it can lead to low self-esteem, social withdrawal and isolation, poor mental health, delayed help-seeking and care access, and more (Nguyen & Li, 2020; Wong et al., 2024). Since dementia-related stigma can affect individuals physically, mentally, and socially, the broadness of QoL indicators helps to encompass the diverse impact that stigmatization results in.
Interventions for Combatting Stigma in Dementia
To reduce the stigmatization of dementia, various intervention strategies have been employed. Such campaigns use similar tactics to HIV/AIDS stigma reduction methods that have shown success for other stigmatizing health conditions (Siette et al., 2023). These include educational interventions, contact-based strategies, or mixed tactics (Nandhakumar, 2024). Like stigma itself, the success and generalizability of these interventions is dependent on context, such as the target audience, cultural background, and the nature of the program (Siette et al., 2023).
Knowledge and awareness of dementia is known to be helpful in reducing stigma, yet studies continue to show that the general public's understanding of dementia is poor (Kim et al., 2023). Educational interventions have been shown to be effective in combatting stigma by providing accurate information about dementia (Noguchi et al., 2023). Different versions of these interventions share the same goal but may vary in their format. They consist of presentations, films, theater performances, intergenerational storytelling, visual arts, factsheets, curriculum-based education, and more (Siette et al., 2023).
Additionally, dementia-related stigma can also be reduced through interacting and engaging with people living with dementia (Noguchi et al., 2023). Such contact interventions can help increase a sense of personhood, especially in contrast to the usual one-sided framing of dementia as an epidemic and a death sentence (Nandhakumar, 2024). Promoting interaction may occur through formal contact-based interventions or may come about through creating environments and opportunities that encourage interaction and engagement (Siette et al., 2023).
Evidence-based and culturally competent interventions have the potential to shift the public perception of dementia, thus reducing stigmatization (Nguyen & Li, 2020). The continued research and development of these interventions is critical, as these negative beliefs and attitudes have harmful effects on the care and QoL for people living with dementia and their families (Rewerska-Juśko & Rejdak, 2020). While the research on dementia-related stigma intervention efficacy is promising, there is still a lack of standardization which limits the ability to compare (Nandhakumar, 2024).
The Current Study
The current study seeks to understand how effective interventions are at reducing dementia-related stigma and improving QoL. Stigma and QoL have been correlated in previous works (Nguyen & Li, 2020; Noguchi et al., 2025). Therefore, it is assumed that stigma and quality of life should be correlated across studies. Additionally, this meta-analysis will examine how having a dementia diagnosis and length of intervention moderate the efficacy of dementia-related stigma reduction interventions. Previous research has shown that a dementia diagnosis can lead to increased levels of self-stigma (Bhatt et al., 2021; Garand et al., 2009). This could create more difficulty in interventions meant to reduce stigma. When investigating intervention length, previous systematic reviews have found that longer intervention lengths with more sessions have proven more effective at reducing stigmatizing attitudes among participants (Mak et al., 2017; Mehta et al., 2015). This meta-analysis aims to answer the following questions:
Methods
The current meta-analysis adheres to PRISMA (preferred reporting items for systematic reviews and meta-analyses) guidelines (Moher et al., 2009).
Transparency and Openness
This study was not preregistered. The first author coded studies, calculated effect sizes, and performed analyses. The second author coded methodological quality of included studies. The first author coded a random sample of studies for methodological quality. The second author coded a random sample of studies for inclusion of study, sample size, proportion female, population size, intervention length, stigma variable, and quality of life variable. The authors were 91.9% in agreement with coding (Cohen's Kappa = 0.788). The study database, dataset, and R script are available via reasonable request to the corresponding author.
Literature Search
The current study utilized strict inclusion and exclusion criteria through TOPICS + M (Johnson & Hennessy, 2019) when planning the search for literature (see Table A1). There were no limits on the population being studied, length of intervention, or publication date. The unlimited population may introduce heterogeneity (e.g., a diagnosed population may report differently than a population that has not had contact with a neurodegenerative disease). However, as dementia-related stigma manifests in public stigma and self-stigma (Kim et al., 2023; Meisenbach, 2010), it is imperative to observe how varying interventions tackle these heterogeneous groups’ perceptions of dementia-related stigma. To account for potential bias related to population experiences with dementia-related illnesses, diagnosis will be analyzed as a moderator. Interventions that were eligible for analysis include educational programming or public health campaigns meant to reduce dementia-related stigma. For outcome variables, dementia-related stigma and quality of life were inclusion criteria. Studies investigating stigma related to dementia, Alzheimer's, and Parkinson's diagnoses were included. Parkinson's disease is not primarily a form of dementia, as it is characterized by motor functions (van der Steen et al., 2019). However, due to limited sample size, studies investigating Parkinson's disease-related stigma were included in analysis if cognitive decline was mentioned. Studies primarily focused on the treatment of Parkinson's motor symptoms (e.g., deep brain stimulation for improved motor function; see Moarrefzadeh et al., 2025) were not included. Stigma related to other illnesses, such as depression or schizophrenia, were excluded from the study. Comparisons were made between treatment and control groups after a stigma-reduction intervention. Therefore, studies that do not include control groups, an intervention aimed at reducing stigma, or post-intervention measures of stigma and quality of life were excluded from analysis.
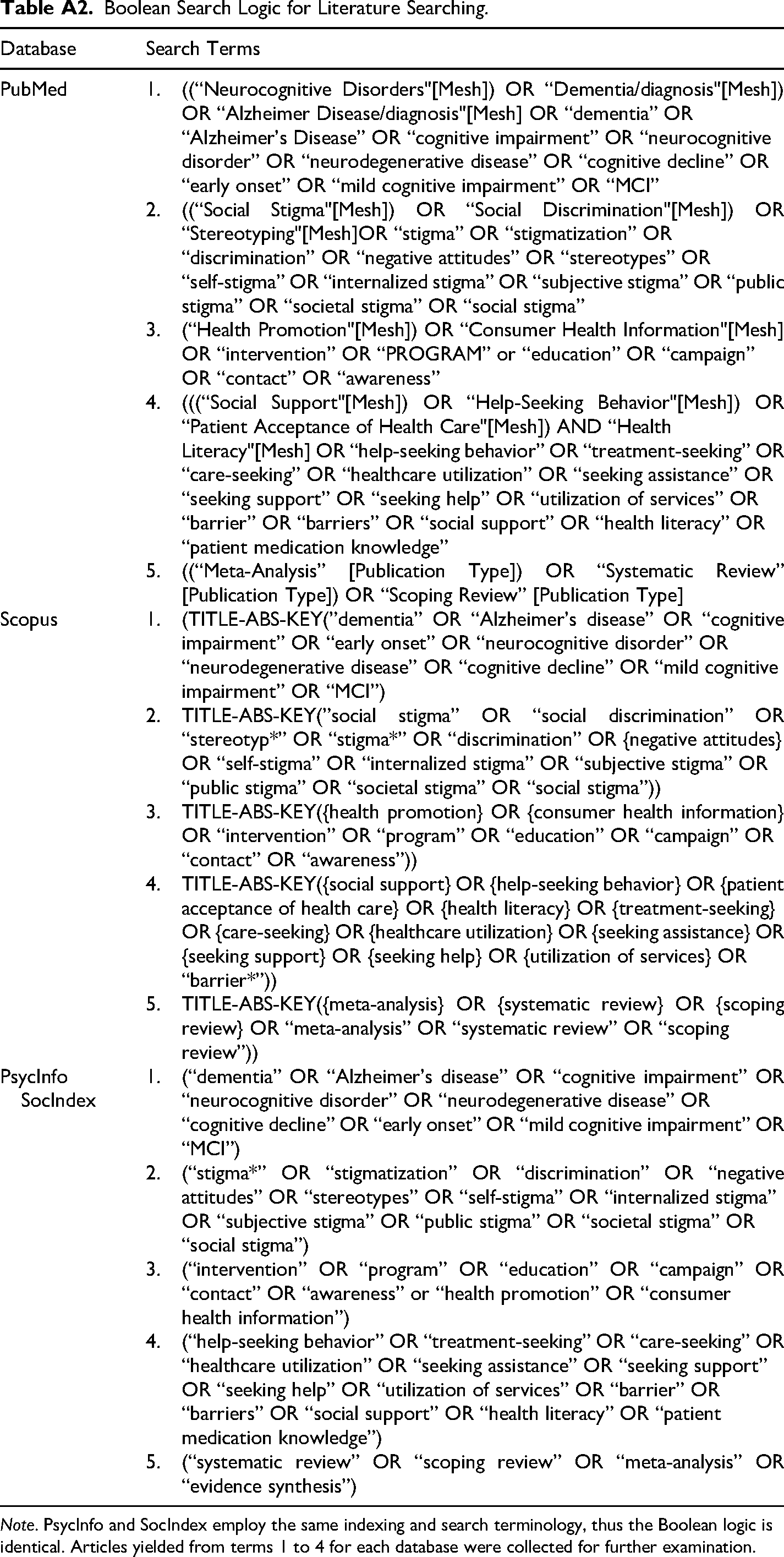
Relevant studies were collected from four databases during the week of October 20 to 24, 2025. Utilizing Boolean search logic (see Table A2), 924 articles were collected: 440 studies from Scopus, 254 studies from PubMed, 167 studies from APA PsycInfo, 59 studies from SocINDEX, and 4 studies from reference back searching (see Figure A1). After removing duplicates (324 articles), 601 titles and abstracts were screened, removing articles based on methodology (e.g., qualitative, narrative review; 310 studies), study design (e.g., cross-sectional survey; 30 articles) or missing variables of interest (e.g., dementia, stigma; 162 articles). Of the 99 articles left for full-text screening, documents were removed if they could not be retrieved (2 studies), did not have an intervention meant to reduce stigma (e.g., testing perceptions; 12 studies), did not use a control group (15 studies), did not have an intervention-based or experimental design (e.g., cross-sectional survey; 45 studies), missing variables of interest (e.g., stigma or QoL; 11 studies) or reported insufficient statistics for effect size calculation (2 studies). This left 7 studies with 13 interventions remaining for analysis.
Coding
Each study was coded based on article, participant, design, and intervention characteristics. Articles were coded for type of publication, year of publication, year of data collection, location (country) of study, and if results could be disaggregated. Participants were coded for sample size, age, proportion white, type of sample (diagnosed with dementia, Alzheimer's disease, or Parkinson's disease; caregiver, proportion exposed to illness), proportion of higher education (above high school), and proportion female. Designs were coded for type of design (e.g., randomized control trial), type of control group (e.g., care as usual), stigma measure, and QoL measure. Interventions were coded for type of intervention, length of intervention, and length of follow-up. Additional measures were collected for both intervention and control groups if included, such as dementia knowledge and statistics reported (e.g., F-test).
Effect Size Calculation and Analysis
Effect sizes (ESs) were calculated from the results provided in the article. For dementia-related stigma and QoL, ESs were calculated as the standardized mean difference (SMD) between the intervention and control group post-intervention and corrected to Hedges’ g (Hedges, 1981). Due to the small sample size of studies included in this meta-analysis, stigma and QoL were assessed broadly. Based on guidelines by Johnson and Eagly (2014), if an article reported multiple measures related to stigma or QoL, multiple ESs were calculated and averaged for an overall ES. Additionally, if studies reported more than one statistic (e.g., M, SD, and t-test), ESs were calculated based on each statistic and triangulated (averaged) for an overall effect. While averaging multiple estimates for overall effect, variance, and error estimates may introduce potential bias, research has shown that the practice is a conservative approach to decrease potential Type 1 error from not taking all reported estimates into account (Moeyaert et al., 2017). For stigma, the sign of ESs was set to negative to signify a reduction is stigma. For QoL, the sign of ESs was set to positive to signify an increase in QoL.
If more than one intervention was conducted in a single study or multiple populations were sampled, results were disaggregated and multiple ESs calculated. This violates non-independence of observations in the ESs. However, given the small sample size included in this meta-analysis, all unique interventions, for example, length or treatment, were included. Studies disaggregated based on population do not violate non-independence of observations of data. The inclusion of multiple populations within the same study offers valuable contributions to the analysis, as they focus on varying diagnoses or relationships to dementia. Therefore, the inclusion of these studies is useful to the understanding of dementia-related stigma reduction programs.
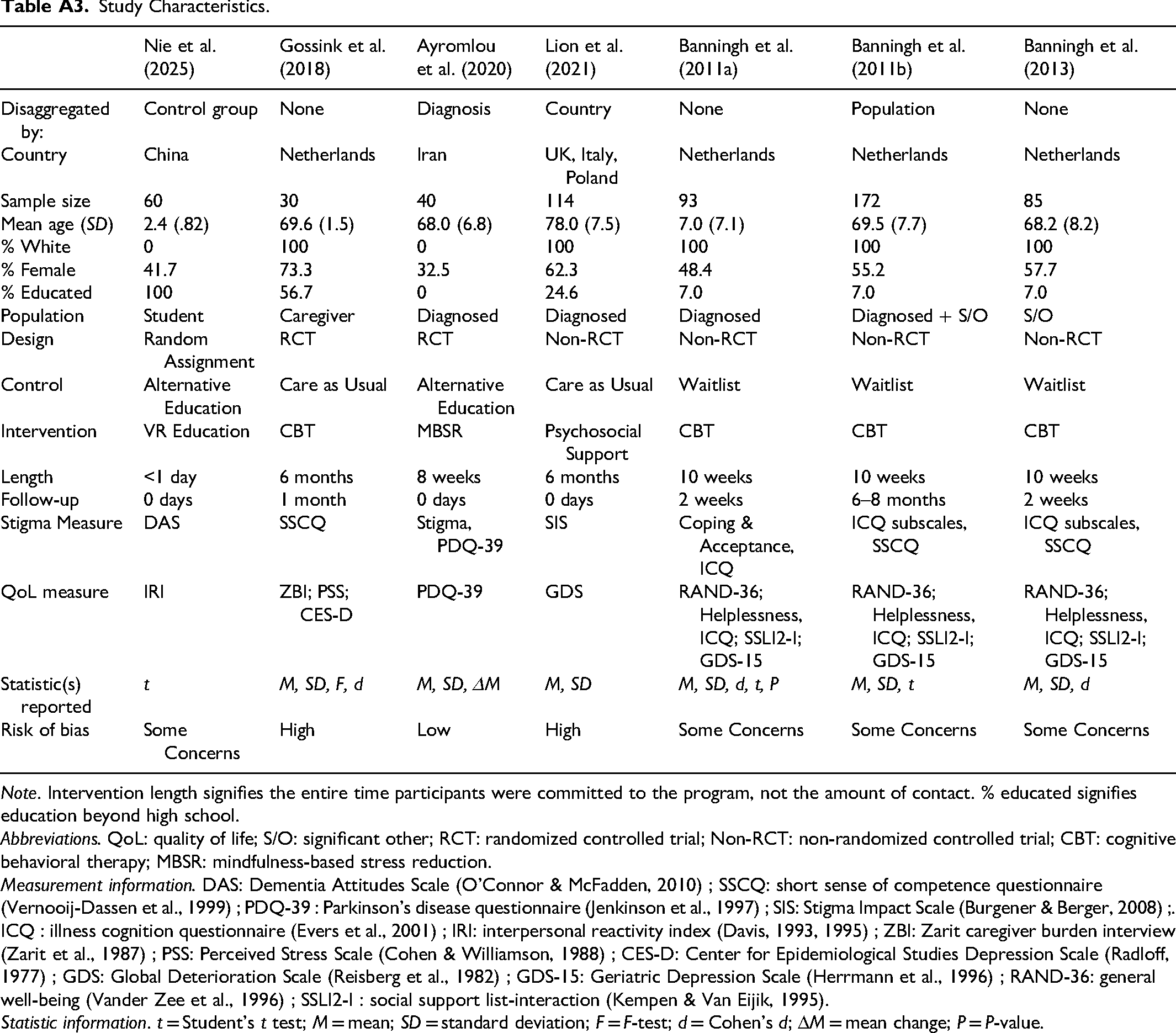
ESs were examined using random-effects models (Lipsey & Wilson, 2001) in metafor (Viechtbauer, 2010). The homogeneity statistic, Q, along with τ2, 95% confidence intervals, and 95% prediction intervals (Borenstein et al., 2017; Huedo-Medina et al., 2006) were calculated to determine the significance of ESs. Small studies bias was analyzed using Egger's test (Egger et al., 1997). Methodological quality was assessed using the revised Cochrane risk of bias (RoB 2.0) tool for RCTs (Sterne et al., 2019). The overall RoB for included studies was classified as low risk, some concern, or high risk (see Table A3). A Pearson correlation test was conducted to examine the relationship between stigma and QoL ESs. A meta-regression was conducted to determine the efficacy of stigma-reduction interventions, with post-intervention stigma ES as the dependent variable, post-intervention QoL as the independent variable, and length of intervention (months) and contact with neurodegenerative disease (proportion) as moderators. The moving constant technique (Johnson & Huedo-Medina, 2011) was conducted to examine ES estimations based on intervention length.
Results
Description of Studies
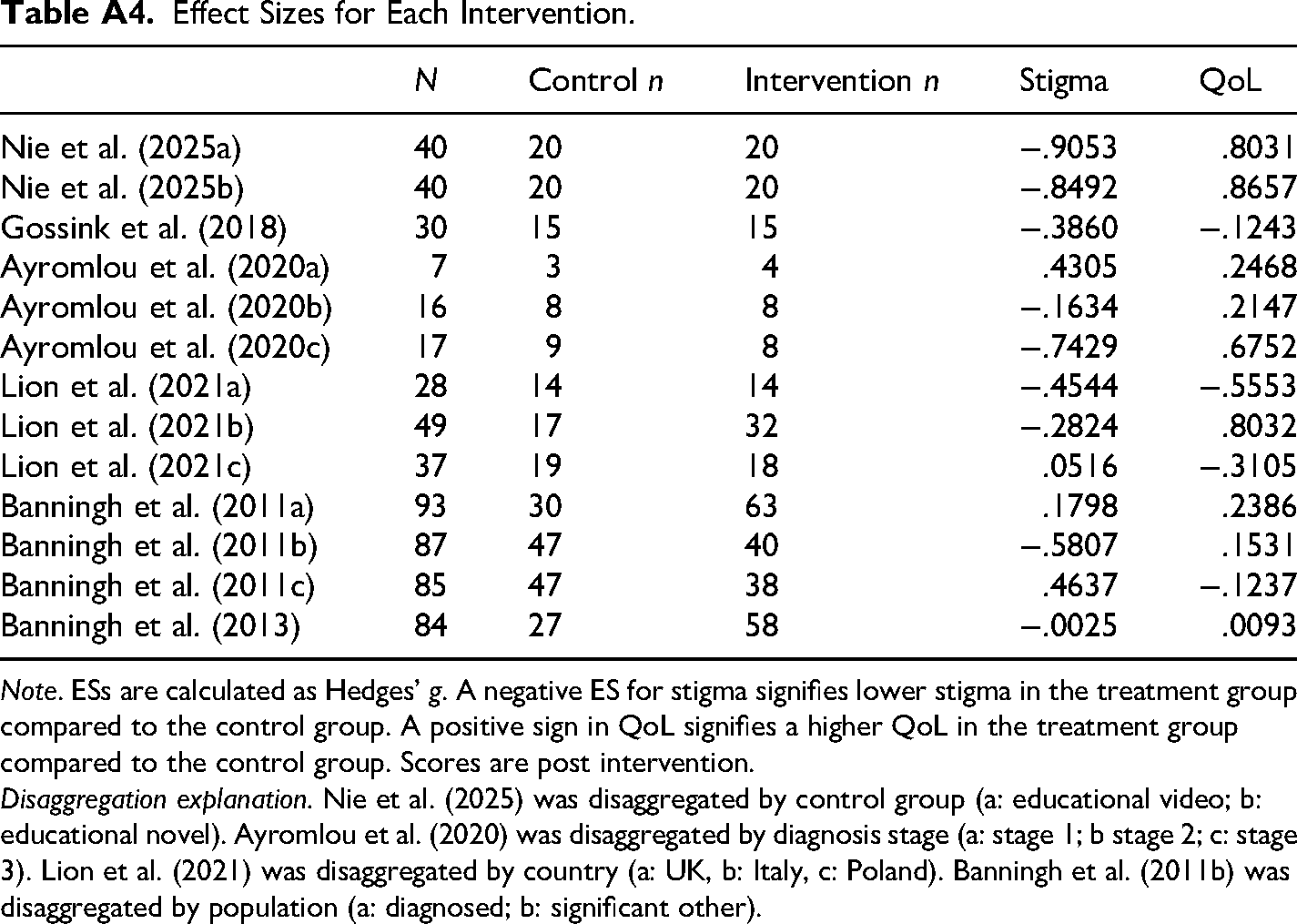
Seven studies, including 13 interventions, 26 effect sizes (see Table A4), and a total sample size of N = 594, were included in this analysis. Studies were published between 2011 and 2025, with four studies being conducted in the Netherlands (57%), one in Iran (14%), one in China (14%), and one conducted internationally in the United Kingdom, Italy, and Poland (14%). The population was 71.4% White (European), 53.0% female, and 55.9% educated beyond high school. The average age of the population ranged 24.0 to 78.0 years (mean of study means = 63.4 years, SD = 19.9), with 56.2% diagnosed with a neurodegenerative disease, 33.5% having a close relationship with someone diagnosed (e.g., significant other or caregiver), and 1.1% having no contact with neurodegenerative diseases. See Table A3 for descriptive information for all studies.
Intervention treatments included educational VR experiences (k = 2), behavioral cognitive therapy (k = 7), mindfulness-based stress reduction (k = 3), and psychosocial support (k = 3). Participants completed interventions spanning an average of four months (M = 116.73 days, SD = 76.55). Of the interventions that included follow-up measures (k = 7), follow-ups occurred on average one month (M = 34 days, SD = 72.8) after the intervention ended. Control group treatments included alternative education (k = 5), care as usual (k = 4), and being put on a wait list for the intervention treatment (k = 6).
Stigma and QoL were assessed using a variety of measures. Stigma was measured using the Dementia Attitudes Scale (DAS; O’Connor & McFadden, 2010), stigma subscale from the 39 item Parkinson's disease questionnaire (PDQ-39; Jenkinson et al., 1997), Stigma Impact Scale (SIS; Burgener & Berger, 2008), coping and acceptance subscales from the illness cognition questionnaire (ICQ; Evers et al., 2001), and short sense of competence questionnaire (SSCQ; Vernooij-Dassen et al., 1999). QoL was measured using the interpersonal reactivity index (IRI; Davis, 1983, 1995), remaining subscales of PDQ-39 (Jenkinson et al., 1997), Zarit caregiver burden interview (ZBI; Zarit et al., 1987), Perceived Stress Scale (PSS; Cohen & Williamson, 1988), Center for Epidemiologic Studies Depression Scale (CES-D; Radloff, 1977), Geriatric Depression Scale (GDS-15; Herrmann et al., 1996), Global Deterioration Scale (GDS; Reisberg et al., 1982), general well-being (RAND-36; Vander Zee et al., 1996), the remaining subscale, helplessness, from ICQ (Evers et al., 2001), and social support list-interaction (SSLI2-I; Kempen & Van Eijk, 1995).
Quantitative Analyses
Following interventions, stigma ESs were nonsignificantly trending negative, indicating a possible reduction of stigma in the treatment group. Similarly, ESs were nonsignificantly trending positive for QoL, indicating a possible increase in QoL in the treatment group. However, both ESs were small, with confidence intervals slightly containing zero (see Table 1).
Mean Effect Sizes for Stigma and Quality of Life Post-Intervention.
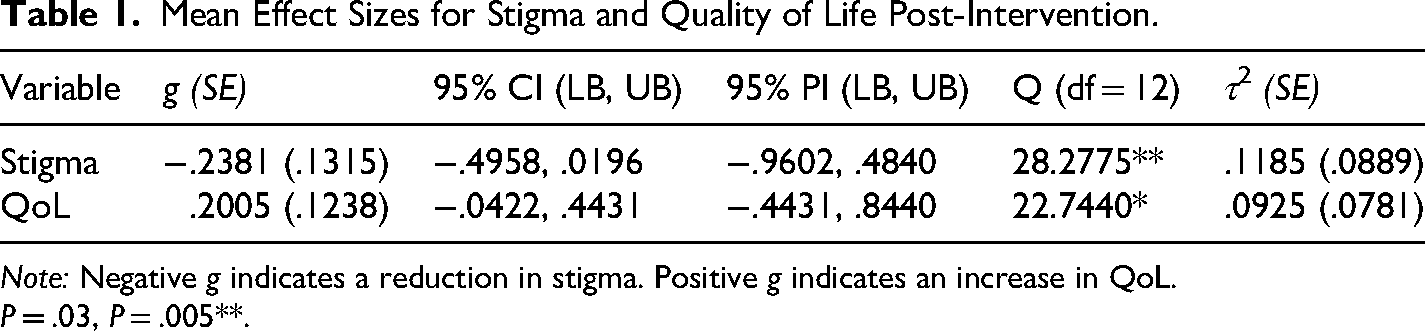
Note: Negative g indicates a reduction in stigma. Positive g indicates an increase in QoL.
P = .03, P = .005**.
When examining ESs for stigma and QoL by intervention, studies contained ESs above and below zero (see Figure 1). Nie et al. (2025) had a significant reduction in stigma and a significant increase in QoL in both interventions. Other studies, such as Banningh et al. (2011b), had significant reductions in stigma for one intervention and significant increases in stigma for others. Overall, many studies contained nonsignificant ESs for stigma and QoL (see Figure A2).
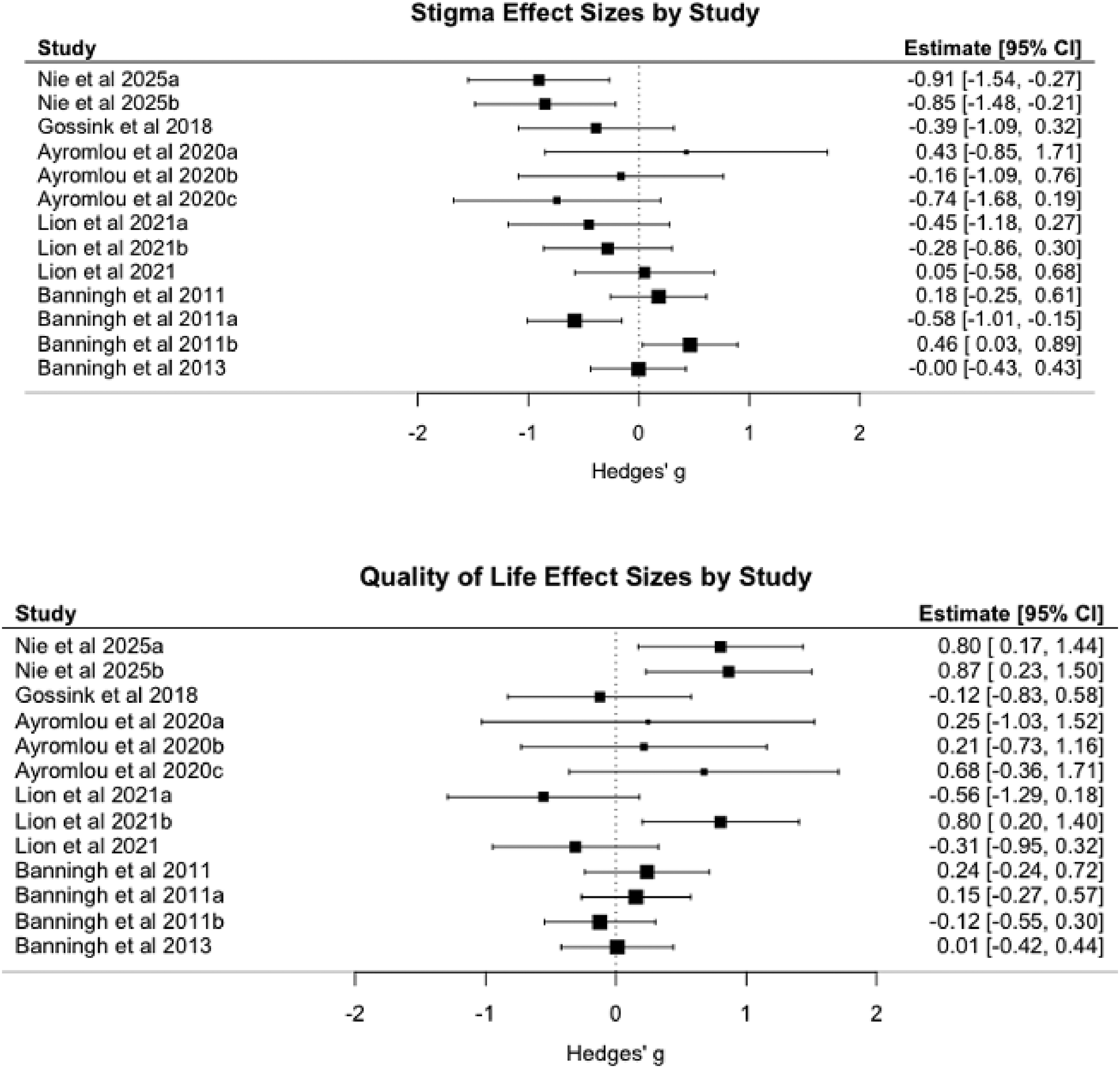
Stigma (top) and quality of life (bottom) effect sizes by study.
Small Studies Bias
Egger's test (Egger et al., 1997) was conducted to examine any bias in ESs in stigma or QoL (see Figure A3). For stigma, Hedges’ g was regressed on its standard error, resulting in a nonsignificant intercept (intercept = .0132, SE = .4171, z = .0318, P = .9747, 95% CI [−.8042, .8307]). The slope of standard error was also nonsignificant (β = −.8110, SE = 1.2812, z = −.6330, P = .5268, 95% CI [−3.3221, 1.7002]). The model accounted for a small amount of heterogeneity (R2 = 3.19%), with moderate heterogeneity remaining (τ2 = .1147, SE = .0901). Therefore, no significant bias was detected for stigma ESs.
For QoL, Hedges’ g was regressed on its standard error, resulting in a nonsignificant intercept (intercept = .3738, SE = .2800, z = 1.3350, P = .1819, 95% CI [−.1750, .9226]). The slope of standard error was also nonsignificant (β = −.4537, SE = .6568, z = −.6908, P = .4897 95% CI [−1.7410, .8336]). The model accounted for no heterogeneity (R2 = .00%), with moderate heterogeneity remaining (τ2 = .1033, SE = .0897). Therefore, no significant bias was detected for QoL ESs.
Relationship Between Stigma and Quality of Life
A Pearson correlation was conducted to determine the relationship between stigma and QoL. After the intervention, stigma and QoL were nonsignificantly trending toward correlation (r = −.4874, t = −1.8513, P = .0911, 95% CI [−.8186, .0869]). This nonsignificant negative relationship suggests that as stigma increases, QoL decreases.
Neurodegenerative Disease Diagnosis and QoL as a Moderator for Stigma Reduction
A random-effects meta-regression was conducted to examine the moderating relationship of neurodegenerative disease diagnosis on QoL and post-intervention stigma. The regression was nonsignificant (see Table 2), with the model accounting for 55.96% of the heterogeneity, QM(3) = 8.2802, P = .0522, leaving moderate residual heterogeneity unaccounted for (τ2 = .0522, SE = .0685, QE(9) = 13.5634, P = .1387). QoL was the only significant predictor (P = .004), with the interaction between QoL and diagnosis being marginally significant (P = .056). Unlike the nonsignificant correlational findings between QoL and stigma (see Figure 2), the meta-regression findings suggest that QoL, when holding diagnosis constant, is a significant predictor of stigma (β = −1.073). The importance of a diagnosis in the relationship between QoL and stigma is further supported by the marginally significant interaction effect of QoL and diagnosis on stigma reduction (β = .984). These analyses are likely underpowered given the small number of studies (k = 13) and large confidence intervals. While power appeared adequate for detecting main effects (e.g., QoL), there was likely not enough power to detect potentially significant interaction effects.
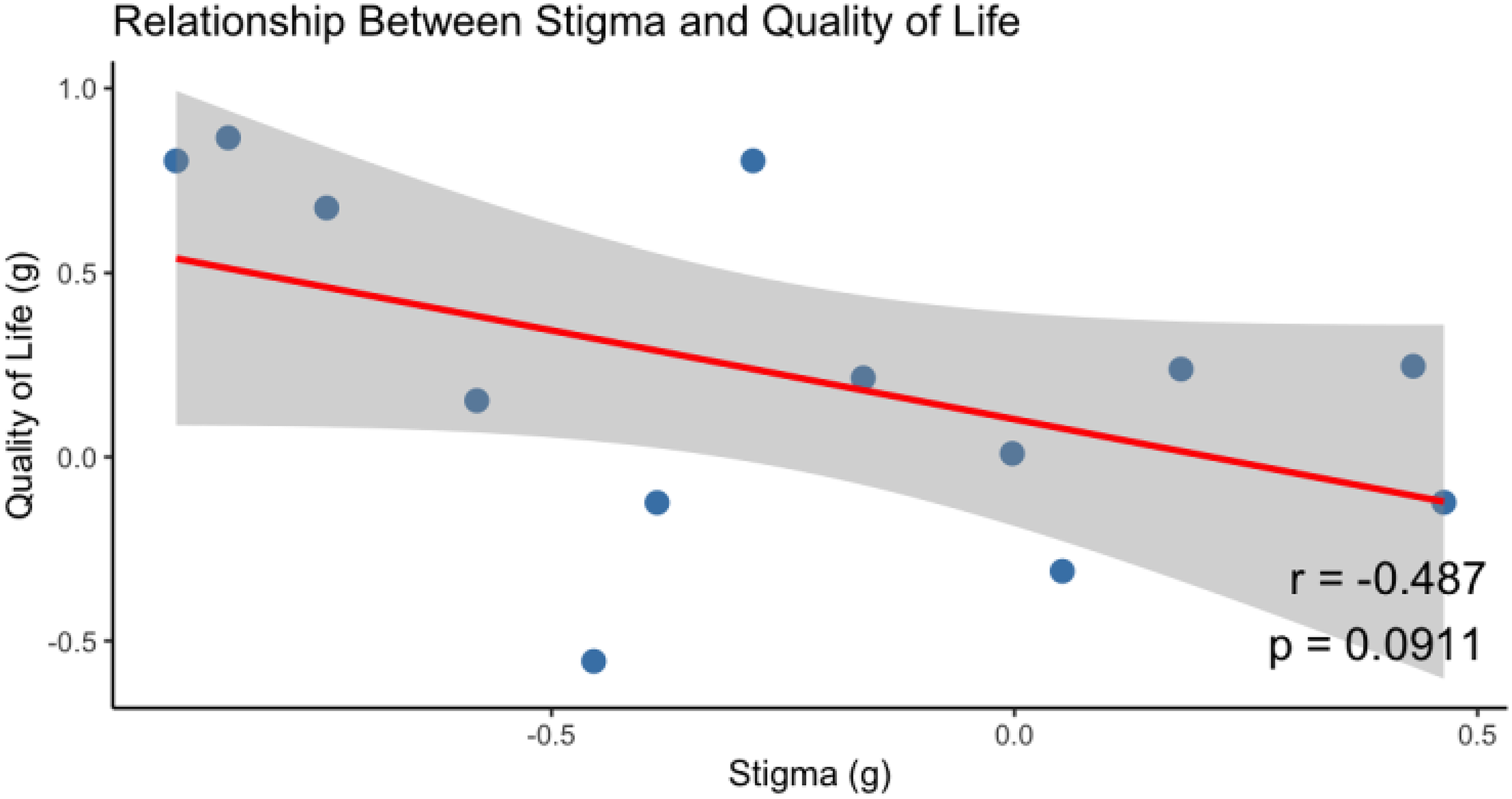
Correlation of stigma and quality of life post intervention.
Meta-Regression of QoL and Diagnosis on Post-Intervention Stigma.
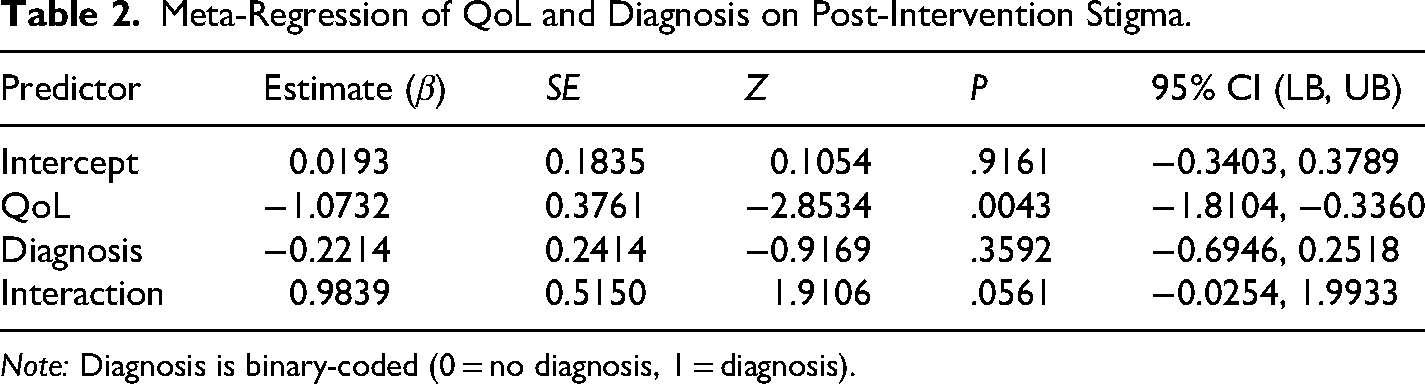
Note: Diagnosis is binary-coded (0 = no diagnosis, 1 = diagnosis).
Intervention Length as a Moderator for Stigma Reduction
The moving constant technique (Johnson & Huedo-Medina, 2011) was conducted to predict post-intervention stigma at varying lengths of the intervention (M = 116.73 days, SD = 76.55, range = 1 day – 6 months). Lengths of intervention were estimated at short (one SD below the mean), average (mean), and long (one SD above the mean). Other covariates (diagnosis, QoL) were held constant at mean values. Predicted ESs increased slightly with intervention length (see Table 3), with short interventions predicting the smallest reduction in stigma (g = −.0869, 95% CI [−.3355, .1616]) and long interventions predicting the largest reduction in stigma (g = −.1005, 95% CI [−.2901, .0891]). Similar to analyses in Table 2, the moving constant technique was underpowered due to low sample size, resulting in wide confidence intervals containing zero.
Impact of Intervention Length on Stigma Reduction.
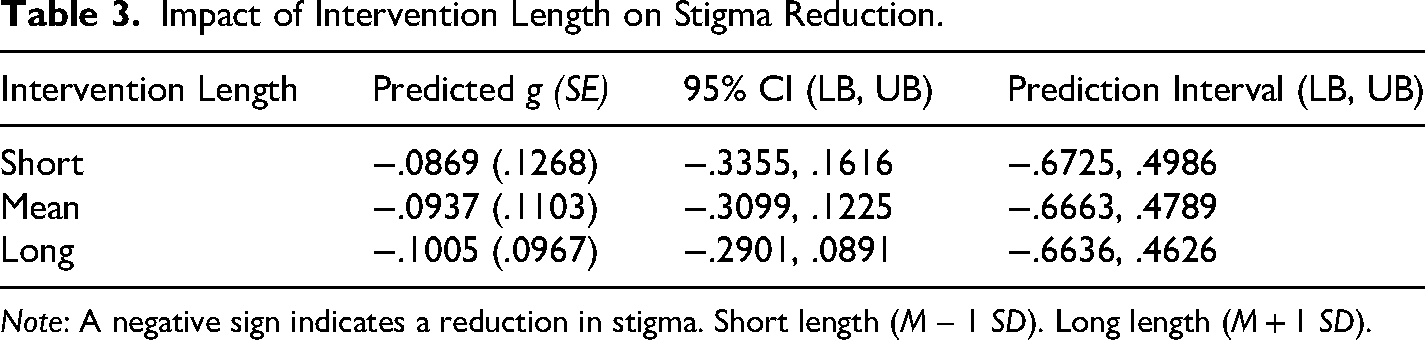
Note: A negative sign indicates a reduction in stigma. Short length (M – 1 SD). Long length (M + 1 SD).
Saturated Model
A random-effects meta-regression was conducted to determine the impacts of all moderators (QoL, intervention length, diagnosis) on stigma reduction post-intervention. The model produced nonsignificant results (see Table 4). The model accounted for a nonsignificant amount of heterogeneity (R2 = 25.97%, QM(6) = 11.9213, P = .2773). Minimal residual heterogeneity was left unaccounted for in the model following analysis (τ2 = .0877, SE = .1045, QE(6) = 11.9213, P = .0637). This model was significantly underpowered, as seen by the large confidence intervals. As such, the current model results offer exploratory analyses for potential relationships between all study variables.
Meta-Regression with QoL, Diagnosis, and Intervention Length Moderators.
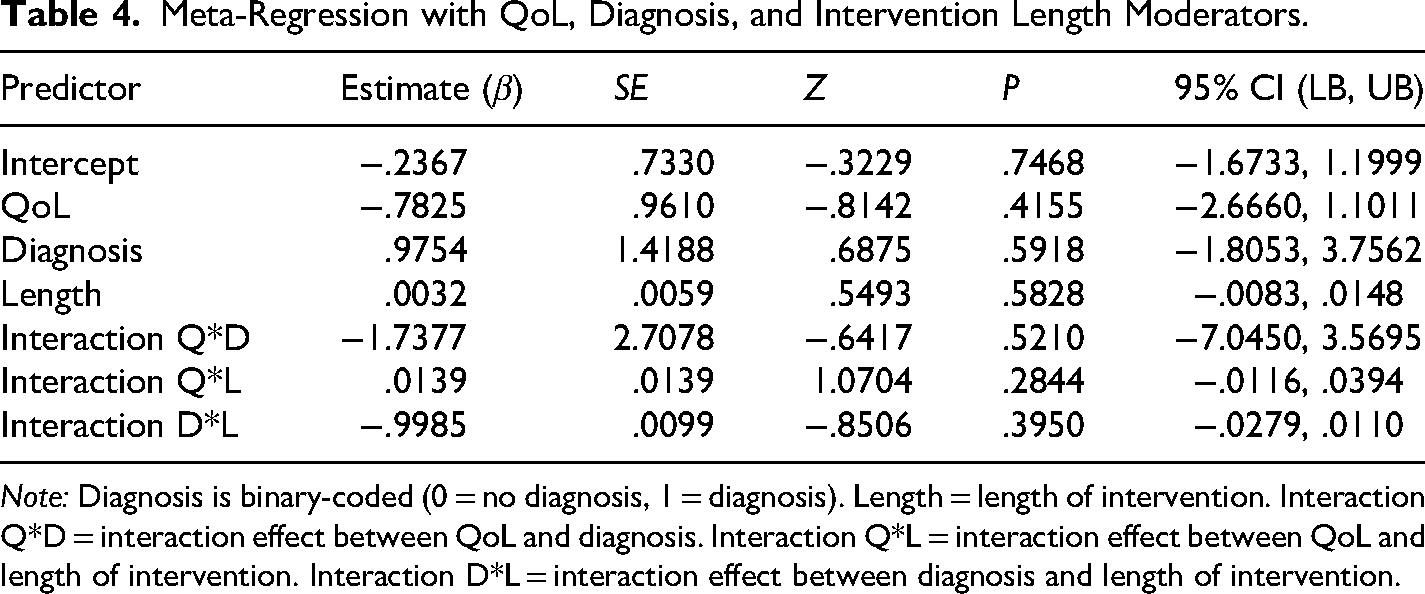
Note: Diagnosis is binary-coded (0 = no diagnosis, 1 = diagnosis). Length = length of intervention. Interaction Q*D = interaction effect between QoL and diagnosis. Interaction Q*L = interaction effect between QoL and length of intervention. Interaction D*L = interaction effect between diagnosis and length of intervention.
Discussion
Despite the robustness of cross-sectional dementia-related stigma research, this meta-analysis identified only a small number of interventions that included interventional methods investigating stigma reduction and QoL, resulting in largely underpowered meta-analytical tests. There were nonsignificant results uncovered, with stigma reduction interventions showing potential trends toward a decrease in stigma and an increase in QoL (Table 1). While QoL had a nonsignificant correlation with stigma (Figure 2), it was a significant predictor of stigma reduction (Table 2). This may be due to the impact of a neurodegenerative diagnosis, with the interaction between diagnosis and QoL being a marginally significant predictor of stigma reduction. Myriad research has connected stigma and QoL in different health contexts (e.g., Nguyen & Li, 2020; Wong et al., 2024). While the current study's regression results corroborate previous research, a significant correlation was not found. It is possible that a larger sample size of studies could have increased the statistical power needed to uncover a significant correlation. This lack of available intervention studies indicates the need for further work in this area. Similarly, dementia diagnostic status and intervention length were nonsignificant predictors of stigma reduction (Table 4). These nonsignificant relationships draw attention to the difficulty of stigma reduction, regardless of the status of the target (e.g., diagnosed) or length of treatment.
Additionally, stigma reduction interventions described in the present work primarily focused on the person experiencing the stigma, which includes the people diagnosed with dementia or their caregivers and loved ones (Table A3). While internalized or self-stigma is prevalent and deserving of attention, community-based interventions should be more widely considered. This meta-analysis indicated a lack of intervention data for targeting public stigma. Inclusion of the wider community, such as those who have little to no interaction with dementia, may be beneficial in making meaningful upstream change that has the power to prevent the cycle of stigma from continuing. In line with SMC theory (Meisenbach, 2010), both public and individual stigma perceptions are critical to our understanding of stigma and the various responses to it.
Implications
The concept of dementia-related stigma is complex, due to the nature of the condition. Dementia is a challenging and progressive disease that still lacks a cure, implying that it is not a condition that is celebrated or embraced. However, this certainly does not warrant the stigma that people affected by dementia face on a regular basis. Stigma has a negative impact on the QoL for people with dementia and their families, such as by creating barriers in accessing care and support (Nguyen & Li, 2020). Despite the known benefits of receiving an early diagnosis, the concern of stigmatization from family, friends, and community members is still a deterring factor for some individuals in seeking testing (Alzheimer's Association, 2025). Among the six strategies described in Meisenbach's (2010) theory of SMC are various ways in which the denial or rejection of a stigmatized identity may prevent someone with dementia or possible dementia from getting the help they need. Dementia-related stigma needs to be combatted in order for meaningful change to occur, both in attempting to improve QoL and increase access to the necessary care and services.
This meta-analysis indicates the dearth of research into dementia-related stigma reduction interventions. There is a lack of consensus on the most efficacious intervention options, methods of measuring outcomes, and length of interventions. Further research and intervention implementation is needed to identify ways to best combat the harmful stigma that negatively impacts a large segment of our society. It is our hope that future research can continue testing and refining stigma-reduction interventions to increase the statistical power required to meta-analytically assess overall intervention effects.
Limitations
No study is without limitations. This meta-analysis is limited by the small sample size of studies. It is possible that more studies meeting the criteria could have impacted the overall mean effects for stigma and QoL, which were both nonsignificantly trending toward significance. Related to this, one study (Nie et al., 2025) violates independence, with the intervention group being compared to two different control group treatments. This intervention produced different effects when compared to each control group's stigma (g = −.9053; g = −.8492) and QoL (g = .8031; g = .8657). Therefore, the disaggregated comparisons are considered worthwhile contributions to the overall meta-analytical sample. Another limitation of this meta-analysis is the study reporting. First, there is a large variety of stigma and QoL measures reported across studies. Geriatric studies appear to have saturated the number of measures used to assess the key variables used in this analysis, utilizing multiple measures focusing on self-stigma, social stigma, and structural stigma. As a result, ESs were averaged across measures, which could have introduced unknown covariates. Additionally, descriptions of interventions, such as contact time and program treatment, were lacking. This decreased the full analysis that could have been completed to determine the efficacy of treatments. Finally, this meta-analysis is limited by the makeup of the sample. First, all studies included are peer-reviewed publications. While no publication bias was found in the sample (Figure A3), it is possible results could have been impacted by the publications included. Additionally, almost all of the studies analyzed were conducted in European countries. As dementia-related stigma is rooted in cultural norms, this likely skewed results of the intervention efficacy. Lastly, populations varied widely, including students, diagnosed, caregivers, and loved ones. While stigma is present in all of these populations, the heterogeneity of the sample could introduce unknown biases related to each population's experiences and perceptions of dementia.
To increase the sample size, this meta-analysis expanded the requirement of dementia-related stigma to also include those diagnosed with Parkinson's disease. One study (Ayromlou et al., 2020) in the sample focused on Parkinson's disease. This study performed a mindfulness-based stress reduction intervention to improve cognitive symptoms (e.g., mental health, cognitive function). This study was compared to other interventions included in the sample (e.g., Lion et al., 2021) and found to share similarities with both the intervention and symptoms being targeted. As a neurodegenerative disease, Parkinson's functions similarly to Alzheimer's disease and related dementias in that it is caused by an accumulation of protein in the brain (Alzheimer's Association, 2025). Parkinson's disease is considered a common cause of dementia, although it is important to note that not all people living with Parkinson's disease experience symptoms of dementia.
Directions for Future Research
Future research should continue investigating the efficacy of dementia-related stigma reduction interventions. Analysis could be improved by a wider literature search, thus improving the small sample limitation and offering additional intervention methods (i.e., variety in treatment, length, or follow-up). Additionally, a larger sample size could allow for additional moderator analysis, such as the efficacy of interventions for individuals who do not know someone with a dementia diagnosis. Furthermore, knowledge of dementia, a common outcome of intervention designs, could serve as a moderator if measured pre-intervention, as literature shows that knowledge of the disease may decrease stigma toward diagnosed individuals (Noguchi et al., 2023).
Another area of future research could investigate different types of study design. While this study investigated intervention efficacy, numerous studies excluded report cross-sectional survey results or qualitative findings. Future analyses could employ correlational analyses to better estimate the relationship between stigma and QoL, as well as test the impact of moderators, such as having a dementia diagnosis. Qualitative findings could highlight the nuances often associated with lived experiences of stigma. A mixed-method meta-analysis would be beneficial to test overall relationships and offer support through meta-synthesis of interview and focus group data.
Conclusion
In conclusion, this meta-analytic review sought to examine the efficacy of interventions for reducing dementia-related stigma and improving QoL. After analyzing seven studies, totaling 13 interventions and 26 ESs, nonsignificant effects were found for both stigma (g = −.24, 95% CI [−.50, .02]) and QoL (g = .20, 95% CI [−.04, .44]). Additionally, QoL was a significant predictor for stigma reduction (β = −1.0732, P = .004), even though stigma and QoL had a nonsignificant correlation (r = −.49, P = .09). This finding could be due to the impact of a dementia diagnosis, with the interaction between QoL and diagnosis being a marginally significant predictor for stigma reduction (β = .9839, P = .0561). Intervention length and confirmed diagnosis were nonsignificant predictors of stigma reduction. Even though the current analyses are limited by the lack of statistical power, results emphasize the deep-rooted stigma impacting individuals affected by dementia, which proves to be difficult to change. Future research should continue testing different interventions to reduce stigma and improve QoL among this marginalized group.
Footnotes
Acknowledgments
The authors thank two librarians, Victoria Helwig and Fyansia Nsilo-Swai, for their assistance creating search terms for the literature search. The authors also thank Dr. Blair T. Johnson for his guidance in the research, analyses, and writing of this meta-analysis.
Ethical Considerations
No IRB was required for this study. The studies included were collected from public databases. This study adheres to PRISMA reporting guidelines.
Consent to Participate
Not applicable.
Consent for Publication
Not applicable.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The study database, dataset, and R script are available via reasonable request to the corresponding author.
Appendix
TOPICS + M. No limits on sample population Education program, intervention, or campaign designed to reduce dementia-related stigma Interventions focused on an unrelated illness (psychiatric disorders, substance abuse, etc.) Interventions or manipulations that are not designed to reduce stigma Changes in dementia-related stigma or attitudes when compared to control group pre/post intervention Studies that do not include a control group Dementia-related stigma reduction Improved quality of life Studies that do not report dementia-related stigma/attitudes or quality of life measures No limits on longitudinal sessions, duration or frequency of intervention No limits on publication/presentation date Pre/post study with control group (RCT or non-RCT) Intervention, experiment, or quasi-experiment Studies lacking a control group Studies lacking an intervention or manipulation meant to reduce dementia-related stigma Dementia Diagnosis Length of intervention Boolean Search Logic for Literature Searching. ((“Neurocognitive Disorders"[Mesh]) OR “Dementia/diagnosis"[Mesh]) OR “Alzheimer Disease/diagnosis"[Mesh] OR “dementia” OR “Alzheimer's Disease” OR “cognitive impairment” OR “neurocognitive disorder” OR “neurodegenerative disease” OR “cognitive decline” OR “early onset” OR “mild cognitive impairment” OR “MCI” ((“Social Stigma"[Mesh]) OR “Social Discrimination"[Mesh]) OR “Stereotyping"[Mesh]OR “stigma” OR “stigmatization” OR “discrimination” OR “negative attitudes” OR “stereotypes” OR “self-stigma” OR “internalized stigma” OR “subjective stigma” OR “public stigma” OR “societal stigma” OR “social stigma” (“Health Promotion"[Mesh]) OR “Consumer Health Information"[Mesh] OR “intervention” OR “PROGRAM” or “education” OR “campaign” OR “contact” OR “awareness” (((“Social Support"[Mesh]) OR “Help-Seeking Behavior"[Mesh]) OR “Patient Acceptance of Health Care"[Mesh]) AND “Health Literacy"[Mesh] OR “help-seeking behavior” OR “treatment-seeking” OR “care-seeking” OR “healthcare utilization” OR “seeking assistance” OR “seeking support” OR “seeking help” OR “utilization of services” OR “barrier” OR “barriers” OR “social support” OR “health literacy” OR “patient medication knowledge” ((“Meta-Analysis” [Publication Type]) OR “Systematic Review” [Publication Type]) OR “Scoping Review” [Publication Type] (TITLE-ABS-KEY(”dementia” OR “Alzheimer's disease” OR “cognitive impairment” OR “early onset” OR “neurocognitive disorder” OR “neurodegenerative disease” OR “cognitive decline” OR “mild cognitive impairment” OR “MCI”) TITLE-ABS-KEY(”social stigma” OR “social discrimination” OR “stereotyp*” OR “stigma*” OR “discrimination” OR {negative attitudes} OR “self-stigma” OR “internalized stigma” OR “subjective stigma” OR “public stigma” OR “societal stigma” OR “social stigma”)) TITLE-ABS-KEY({health promotion} OR {consumer health information} OR “intervention” OR “program” OR “education” OR “campaign” OR “contact” OR “awareness”)) TITLE-ABS-KEY({social support} OR {help-seeking behavior} OR {patient acceptance of health care} OR {health literacy} OR {treatment-seeking} OR {care-seeking} OR {healthcare utilization} OR {seeking assistance} OR {seeking support} OR {seeking help} OR {utilization of services} OR “barrier*”)) TITLE-ABS-KEY({meta-analysis} OR {systematic review} OR {scoping review} OR “meta-analysis” OR “systematic review” OR “scoping review”)) (“dementia” OR “Alzheimer's disease” OR “cognitive impairment” OR “neurocognitive disorder” OR “neurodegenerative disease” OR “cognitive decline” OR “early onset” OR “mild cognitive impairment” OR “MCI”) (“stigma*” OR “stigmatization” OR “discrimination” OR “negative attitudes” OR “stereotypes” OR “self-stigma” OR “internalized stigma” OR “subjective stigma” OR “public stigma” OR “societal stigma” OR “social stigma”) (“intervention” OR “program” OR “education” OR “campaign” OR “contact” OR “awareness” or “health promotion” OR “consumer health information”) (“help-seeking behavior” OR “treatment-seeking” OR “care-seeking” OR “healthcare utilization” OR “seeking assistance” OR “seeking support” OR “seeking help” OR “utilization of services” OR “barrier” OR “barriers” OR “social support” OR “health literacy” OR “patient medication knowledge”) (“systematic review” OR “scoping review” OR “meta-analysis” OR “evidence synthesis”) Note. PsycInfo and SocIndex employ the same indexing and search terminology, thus the Boolean logic is identical. Articles yielded from terms 1 to 4 for each database were collected for further examination. Study Characteristics. Note. Intervention length signifies the entire time participants were committed to the program, not the amount of contact. % educated signifies education beyond high school. Abbreviations. QoL: quality of life; S/O: significant other; RCT: randomized controlled trial; Non-RCT: non-randomized controlled trial; CBT: cognitive behavioral therapy; MBSR: mindfulness-based stress reduction. Measurement information. DAS: Dementia Attitudes Scale (O’Connor & McFadden, 2010) ; SSCQ: short sense of competence questionnaire (Vernooij-Dassen et al., 1999) ; PDQ-39 : Parkinson's disease questionnaire (Jenkinson et al., 1997) ; SIS: Stigma Impact Scale (Burgener & Berger, 2008) ;. ICQ : illness cognition questionnaire (Evers et al., 2001) ; IRI: interpersonal reactivity index (Davis, 1993, 1995) ; ZBI: Zarit caregiver burden interview (Zarit et al., 1987) ; PSS: Perceived Stress Scale (Cohen & Williamson, 1988) ; CES-D: Center for Epidemiological Studies Depression Scale (Radloff, 1977) ; GDS: Global Deterioration Scale (Reisberg et al., 1982) ; GDS-15: Geriatric Depression Scale (Herrmann et al., 1996) ; RAND-36: general well-being (Vander Zee et al., 1996) ; SSLI2-I : social support list-interaction (Kempen & Van Eijik, 1995). Statistic information. t = Student's t test; M = mean; SD = standard deviation; F = F-test; d = Cohen's d; ΔM = mean change; P = P-value. Effect Sizes for Each Intervention. Note. ESs are calculated as Hedges’ g. A negative ES for stigma signifies lower stigma in the treatment group compared to the control group. A positive sign in QoL signifies a higher QoL in the treatment group compared to the control group. Scores are post intervention. Disaggregation explanation. Nie et al. (2025) was disaggregated by control group (a: educational video; b: educational novel). Ayromlou et al. (2020) was disaggregated by diagnosis stage (a: stage 1; b stage 2; c: stage 3). Lion et al. (2021) was disaggregated by country (a: UK, b: Italy, c: Poland). Banningh et al. (2011b) was disaggregated by population (a: diagnosed; b: significant other).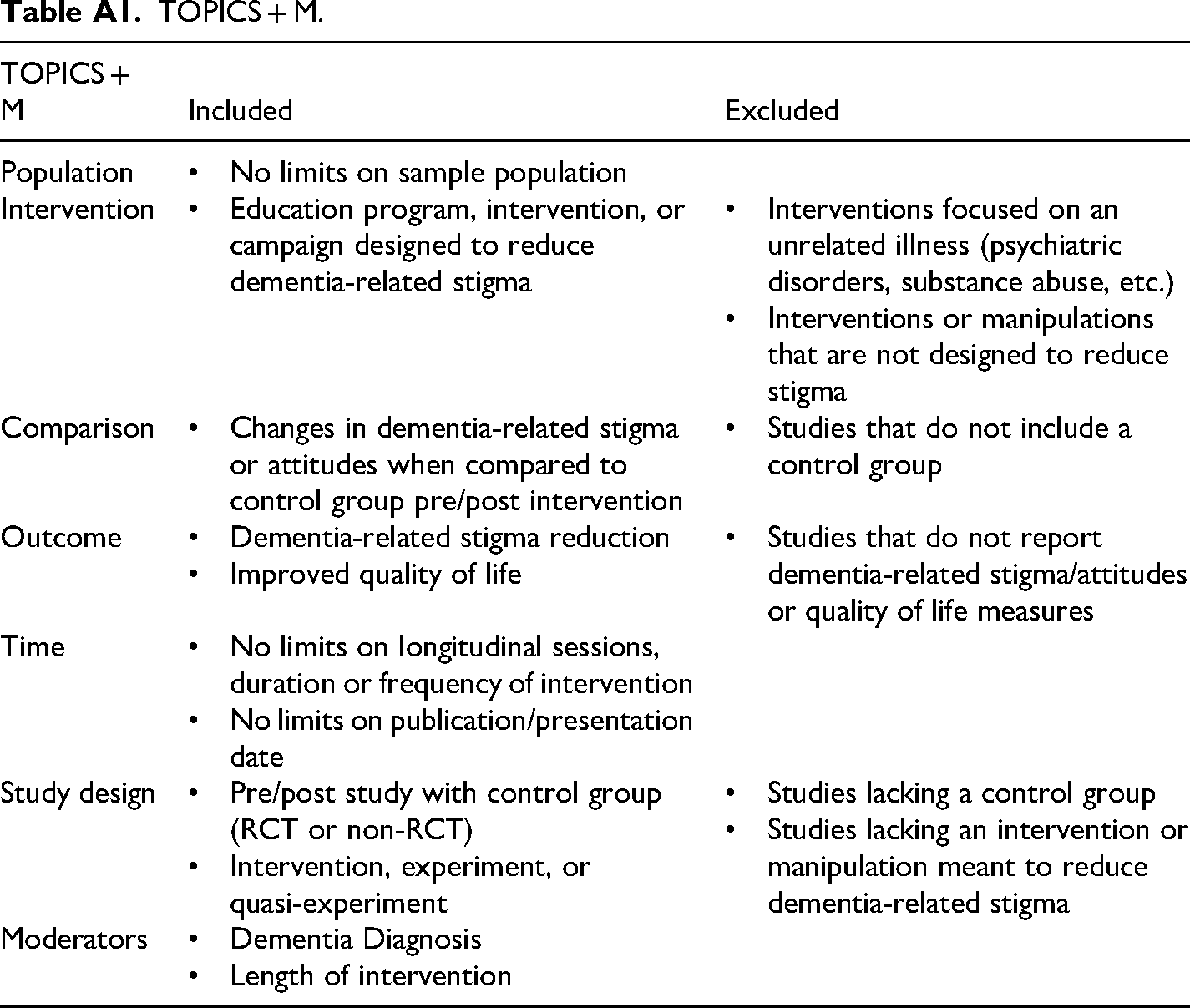
TOPICS + M
Included
Excluded
Population
Intervention
Comparison
Outcome
Time
Study design
Moderators
Database
Search Terms
PubMed
Scopus
PsycInfo SocIndex
Nie et al. (2025)
Gossink et al. (2018)
Ayromlou et al. (2020)
Lion et al. (2021)
Banningh et al. (2011a)
Banningh et al. (2011b)
Banningh et al. (2013)
Disaggregated by:
Control group
None
Diagnosis
Country
None
Population
None
Country
China
Netherlands
Iran
UK, Italy, Poland
Netherlands
Netherlands
Netherlands
Sample size
60
30
40
114
93
172
85
Mean age (SD)
2.4 (.82)
69.6 (1.5)
68.0 (6.8)
78.0 (7.5)
7.0 (7.1)
69.5 (7.7)
68.2 (8.2)
% White
0
100
0
100
100
100
100
% Female
41.7
73.3
32.5
62.3
48.4
55.2
57.7
% Educated
100
56.7
0
24.6
7.0
7.0
7.0
Population
Student
Caregiver
Diagnosed
Diagnosed
Diagnosed
Diagnosed + S/O
S/O
Design
Random Assignment
RCT
RCT
Non-RCT
Non-RCT
Non-RCT
Non-RCT
Control
Alternative Education
Care as Usual
Alternative Education
Care as Usual
Waitlist
Waitlist
Waitlist
Intervention
VR Education
CBT
MBSR
Psychosocial Support
CBT
CBT
CBT
Length
<1 day
6 months
8 weeks
6 months
10 weeks
10 weeks
10 weeks
Follow-up
0 days
1 month
0 days
0 days
2 weeks
6–8 months
2 weeks
Stigma Measure
DAS
SSCQ
Stigma, PDQ-39
SIS
Coping & Acceptance, ICQ
ICQ subscales, SSCQ
ICQ subscales, SSCQ
QoL measure
IRI
ZBI; PSS; CES-D
PDQ-39
GDS
RAND-36; Helplessness, ICQ; SSLI2-I; GDS-15
RAND-36; Helplessness, ICQ; SSLI2-I; GDS-15
RAND-36; Helplessness, ICQ; SSLI2-I; GDS-15
Statistic(s) reported
t
M, SD, F, d
M, SD, ΔM
M, SD
M, SD, d, t, P
M, SD, t
M, SD, d
Risk of bias
Some Concerns
High
Low
High
Some Concerns
Some Concerns
Some Concerns
N
Control n
Intervention n
Stigma
QoL
Nie et al. (2025a)
40
20
20
−.9053
.8031
Nie et al. (2025b)
40
20
20
−.8492
.8657
Gossink et al. (2018)
30
15
15
−.3860
−.1243
Ayromlou et al. (2020a)
7
3
4
.4305
.2468
Ayromlou et al. (2020b)
16
8
8
−.1634
.2147
Ayromlou et al. (2020c)
17
9
8
−.7429
.6752
Lion et al. (2021a)
28
14
14
−.4544
−.5553
Lion et al. (2021b)
49
17
32
−.2824
.8032
Lion et al. (2021c)
37
19
18
.0516
−.3105
Banningh et al. (2011a)
93
30
63
.1798
.2386
Banningh et al. (2011b)
87
47
40
−.5807
.1531
Banningh et al. (2011c)
85
47
38
.4637
−.1237
Banningh et al. (2013)
84
27
58
−.0025
.0093